Management of Neutropenic Sepsis Rebecca Frewin Consultant Haematologist

Management of Neutropenic Sepsis Rebecca Frewin Consultant Haematologist Gloucestershire Hospitals NHS Foundation Trust

Aims of today What Why How • The definition of neutropenic sepsis • Importance for Emergency Clinicians • Outcomes of Neutropenic sepsis • Assessment of neutropenic sepsis • Guidelines for management of neutropenic sepsis • Spot diagnoses

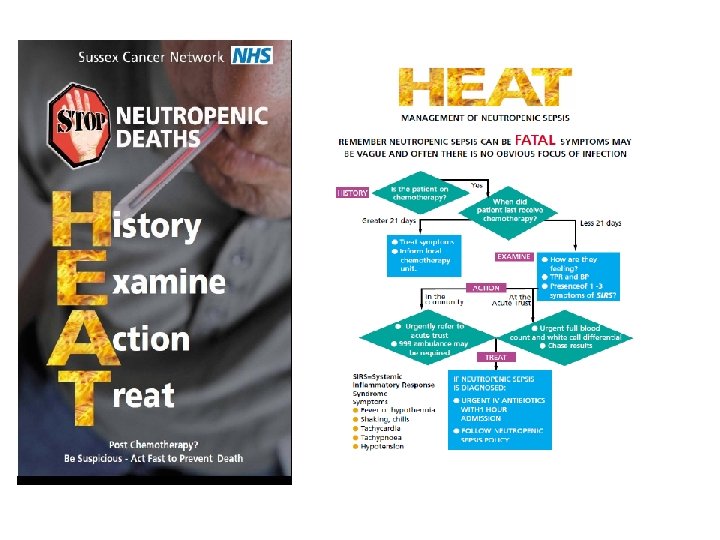
Definition of Neutropenic Sepsis Diagnose neutropenic sepsis in patients having anticancer treatment whose neutrophil count is 0. 5 × 109 per litre or lower and who have either: a temperature higher than 38 o. C or other signs or symptoms consistent with clinically significant sepsis. NICE Clinical Guideline 151: September 2012
 • Patients are often described as being")
Sepsis or Systemic Inflammatory Response Syndrome (SIRS) • Patients are often described as being ‘septic’ or in ‘septic shock’ • Systemic inflammatory response syndrome (SIRS) – – Temperature >38 o. C or <36 o. C Heart rate >90/min Respiratory rate >20 or Pa. CO 2 <4. 3 k. Pa White Cell Count >12 x 10 9/l • Sepsis is defined as SIRS in response to infection • Severe sepsis is sepsis associated with: – Organ dysfunction – Hypotension (systolic BP <90 mm. Hg or >40 mm. Hg from normal) – Organ hypoperfusion (lactic acidosis, oliguria, acute alteration of mental status) • Septic shock describes sepsis with hypotension despite adequate fluid resuscitation

Deaths from Neutropenic Sepsis • 2 deaths/ day from neutropenic sepsis • 60% increase in chemotherapy between 2002 – 2006 • More intensive regimes • Highest death rate is in 65 -79 year olds

Neutropenic sepsis: higher risk of dying in young patients

Where do neutropenic sepsis patients present? SACT Report 2008


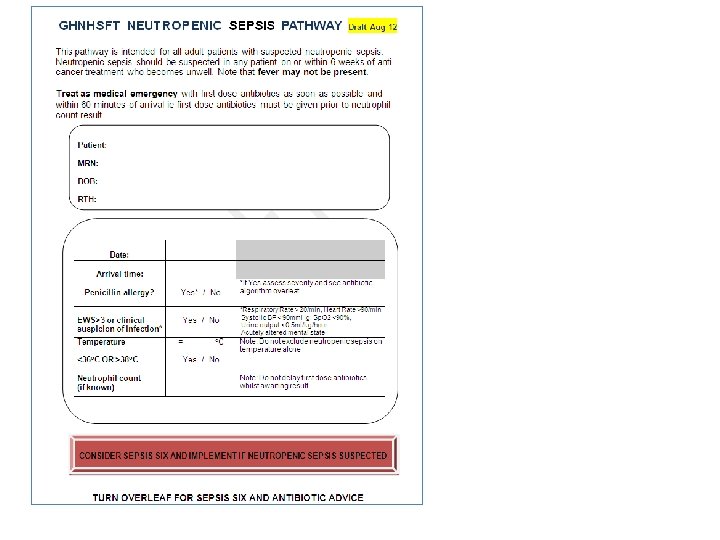
Approach to neutropenic sepsis 1. Assessment Ø Initial assessment Ø Investigations Ø More detailed review 2. Treatment Ø Ø Antibiotics Fluid resuscitation Vasopressors Blood product support

Initial assessment • Brief history – Symptoms – Recent chemotherapy – ‘Normal’ neutrophil count – Late onset neutropenia in rituximab patients • Limited examination – MEWs – not validated in neutropenic patients – Review of any obvious source

Investigations • For CXR, probability of pneumonia in a child without respiratory symptoms was 1. 9% (Phillips et al (2011) • Peripheral blood cultures – 28/228 cultures were positive (Sheienmann et al (2010). The differential time to positivity of cultures between central and peripheral cultures can be indicative of catheter related thrombosis NICE Clinical Guideline 151

Early Lactate-Guided Therapy in Intensive Care Unit Patients adjusted HR= 0. 61; 95% CI, 0. 43 -0. 87; P= 0. 006 Jansen TC. Am J Respir Crit Care Med. 2010; 182: 752– 761. Slide 13 Copyright 2014 SCCM/ESICM

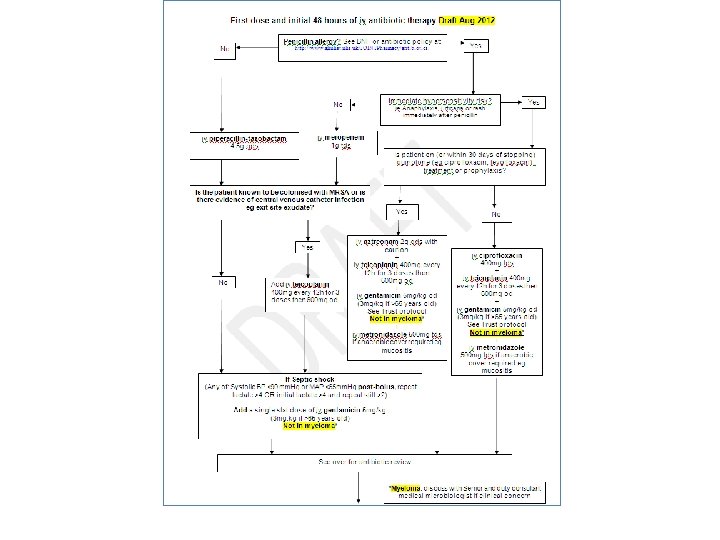
Treatment: antibiotics

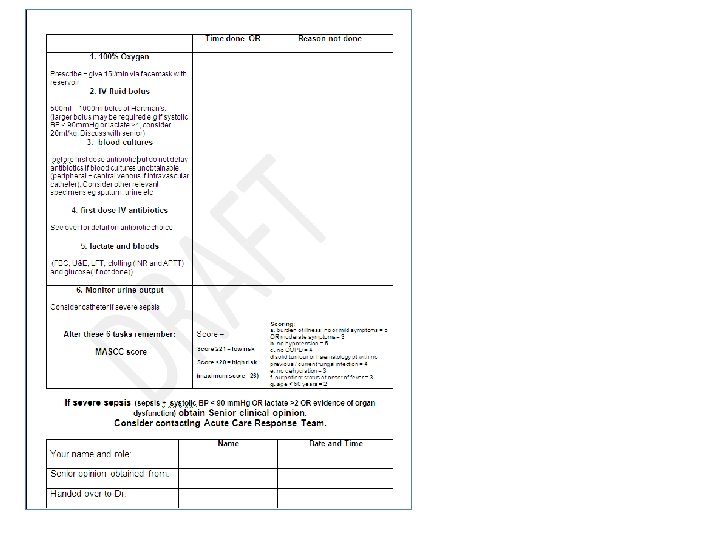
MASCC score in neutropenic sepsis

Initial Resuscitation • During the first 6 hours, the goals of initial resuscitation of sepsis-induced hypoperfusion should include all of the following as a part of a treatment protocol (Grade 1 C): – Central venous pressure 8 -12 mm Hg – Mean arterial pressure ≥ 65 mm Hg – Urine output ≥ 0. 5 m. L/kg/h – Central venous (superior vena cava) or mixed venous oxygen saturation 70% or 65%, respectively Slide 17 Copyright 2014 SCCM/ESICM

Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock Control EGDT Relative Risk (95% Confidence Interval) In-Hospital 46. 5 30. 58 (0. 38 -0. 87) 0. 009 28 -day Mortality 49. 2 33. 3 0. 58 (0. 39 – 0. 87) 0. 01 44. 3 0. 67 (0. 46 -0. 96) 0. 03 60 -day Mortality 56. 9 P Rivers E. N Engl J Med. 2001; 345: 1368 -1377. Slide 18 Copyright 2014 SCCM/ESICM

Fluid Therapy • We recommend an initial fluid challenge in patients with sepsis-induced tissue hypoperfusion with suspicion of hypovolemia to achieve a minimum of 30 m. L/kg of crystalloids (a portion of this may be albumin equivalent). More rapid administration and greater amounts of fluid may be needed in some patients. (Grade 1 C) Slide 19 Copyright 2014 SCCM/ESICM

Fluid Therapy • We recommend crystalloids be used as the initial fluid of choice in the resuscitation of severe sepsis and septic shock. (Grade 1 B) • We recommend against the use of hydroxyethyl starches for fluid resuscitation of severe sepsis and septic shock. (Grade 1 B) Slide 20 Copyright 2014 SCCM/ESICM

Fluid Therapy - Kidney injury • Three multicenter randomized trials showed a significant increase in the risk of acute kidney injury with hydroxyethyl starch as compared with crystalloids. Brunkhorst F. N Engl J Med. 2008; 358: 125 -139. Perner A. N Engl J Med. 2012; 367: 124 -134. Myburgh JA. N Engl J Med. 2012; 367: 1901 -1911. • One multicenter randomized trial did not find an increase in the risk of acute kidney injury with hydroxyethyl starch as compared with crystalloids. Guidet B. Crit Care. 2012; 16: R 94. Slide 21 Copyright 2014 SCCM/ESICM

Fluid Therapy • We suggest the use of albumin in the fluid resuscitation of severe sepsis and septic shock when patients require repeated boluses of crystalloids. (Grade 2 C) Slide 22 Copyright 2014 SCCM/ESICM
")
Meta-analysis: Albumin versus Other Fluids Outcomes Short-term mortality Illustrative comparative risks Relative (95% CI) effect (95% CI) Assumed Corresponding risk Control Other fluids (may be crystalloid or colloid) Study population 342 per 287 per 1000 (249 to 332) 444 per Short-term mortality 1000 (albumin vs crystalloids) 377 per 1000 (324 to 440) Short-term mortality 342 per (albumin vs other 1000 colloids) 1 Grade reduced for imprecision. 195 per 1000 (249 to 396) No. Of Quality of the participants evidence (studies) (GRADE) RR 0. 84 (0. 73 to 0. 97) 1683 ⊕⊕⊕⊝ (11 studies) moderate RR 0. 85 (0. 73 to 0. 98) RR 0. 81 (0. 57 to 1. 16) 1402 (4 studies) ⊕⊕⊕⊝ moderate 1 281 (7 studies) ⊕⊕⊕⊝ moderate 1 Slide 23 Copyright 2014 SCCM/ESICM
 • Norepinephrine is")
Vasopressors • Maintain the MAP >65 mm. Hg (Grade 1 C) • Norepinephrine is recommended as first line vasopressin (Grade 1 B) • Epinephrine may be added to and potentially substituted for norepinephrine when as additional agent is needed to maintain blood pressure (Grade 2 B) • Low dose vasopressin (0. 03 U/min)may be added to norepinephrine with the intent of raising the MAP to target or reducing the norepinephrine dosage • Dopamine should be used only as an alternative vasopressor to norepinephrine only in highly selected patients (eg at low risk of arrythmias and/or a low heart rate) (Grade 2 C)

Meta-analysis of Norepinephrine versus Dopamine Outcomes Illustrative comparative risks* (95% Relative No. of Quality of the CI) effect participants evidence (GRADE) Assumed risk Corresponding risk (95% CI) (studies) Dopamine Short-term mortality 482 per 1000 (440 to 524) RR 0. 91 2043 (0. 83 to (6 studies) 0. 99) ⊕⊕⊕⊝ moderate 1, 2 82 per 1000 (34 to 195) RR 0. 47 1931 (0. 38 to (2 studies) 0. 58) ⊕⊕⊕⊝ moderate 1, 2 15 per 1000 (8 to 27) RR 0. 35 1931 (0. 19 to (2 studies) 0. 66) ⊕⊕⊕⊝ moderate 1, 2 Study population 530 per 1000 Serious adverse events Study population Supraventricular arrhythmias 229 per 1000 Serious adverse events Ventricular arrhythmias Norepinephrine Study population 39 per 1000 *The assumed risk is the median control group risk across studies. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; Strong heterogeneity in the results (I squared = 85%), however this reflects degree of effect, not direction of effect. We have decided not to lower the evidence quality. 2 Effect results in part from hypovolemic and cardiogenic shock patients in De Backer, NEJM 2010. We have lowered the quality of evidence one level for indirectness. 1 Slide 25 Copyright 2014 SCCM/ESICM

Inotropic Therapy • We recommend that a trial of dobutamine infusion up to 20 μg/kg/min be administered or added to vasopressor (if in use) in the presence of: • myocardial dysfunction as suggested by elevated cardiac filling pressures and low cardiac output, or • ongoing signs of hypoperfusion, despite achieving adequate intravascular volume and adequate mean arterial pressure. (Grade 1 C) • We recommend against the use of a strategy to increase cardiac index to predetermined supranormal levels. (Grade 1 B) Slide 26 Copyright 2014 SCCM/ESICM

Blood product support • Maintain Hb >70 g/l with a target of 70 -90 unless extenuating circumstances such as ischaemic coronary artery disease • Give prophylactic platelet transfusions if platelets <10 or <20 with a significant risk of bleeding.

Spot diagnosis in neutropenic patients

Spot diagnosis

Spot diagnosis

Have we covered it all? What Why How • The definition of neutropenic sepsis • Importance for Emergency Clinicians • Outcomes of Neutropenic sepsis • Assessment of neutropenic sepsis • Guidelines for management of neutropenic sepsis • Spot diagnoses
- Slides: 33