Management of Haemorrhage in Pelvic fracture Dr Law



















 • Temporarily control arterial haemorrhage and preserve")



 • 6 -8 cm midline incision from pubic")

- Slides: 28
Management of Haemorrhage in Pelvic fracture Dr Law Lok Yin Department of Surgery, Princess Margaret Hospital
Outline • Background information • Evolution of key management principles • Key questions in management algorithms
Pelvic fracture in trauma • • Poly trauma victim • Vehicular, pedestrians injuries, falls • Associated with multiple injuries and different sources of bleeding Haemodynamically unstable pelvic fracture management is challenging and controversial • No universal agreement • High mortality (up to 40%) • organised algorithm can decrease mortality 1. Institutional practice guidelines on management of pelvic fracture Gilliland MD, et al J Trauma 1982; 22: 691 -693 1
Classification of pelvic fracture • Fracture location • Pelvic stability • Direction injury force • Disruption of surrounding soft tissue envelope Young and Tile’s Burgess classification
Young and Burgess classification Mixed type
Bleeding source • Venous • Bone • Arterial
Pelvic fracture management key points • Overlaps with goals of stabilising a polytraumatised patient • Identify source of bleeding • Manage haemorrhagic shock - cause of death • Early reduction and stabilisation of pelvic fracture
Evolution of Concepts in Management of haemodynamically unstable pelvic fracture
Pre-endovascular era • Direct suture control • Bilateral internal iliac arteries ligation • Intraoperative arterial balloon catheterisation • Pelvic packing Very high mortality Definite control of Bleeding from Severe Pelvic Fractures Lewis M. Flint , JR, MD et al Ann Surg June 1979
1970 s - 1980 s • Postmortem dissection and injection studies of internal iliac arteries following fatal pelvic fractures • Single vessel injuries are infrequent • multiple injured vessels with rich collateralisation
Never Touch the Pelvic Haematoma
Endovascular era • Anti-shock trousers Prevent violation of pelvic haematoma • • Formerly advocated operative techniques were discouraged • • Pelvic packing fell out of favour (USA > Europe) Angiogram and embolisation is favoured for those with unstable hemodynamics despite external compression as the source of ongoing bleeding is thought to be arterial in origin
Pre peritoneal Pelvic Packing for Hemodynamically Unstab C. Clay Cothren, MD, Patrick M. Osborn, MD, Ernest E. Moore, MD, Steven J. Morgan, MD, Jeffrey L. Johnson, MD, and Pre peritoneal pelvic packing for Hemodyniacally unstable pelvic fractures: A paradigm shift Cothren CC, et al J Trauma 2007; 62: 834 -839
Pre peritoneal Pelvic Packing for Hemodynamically Unstab C. Clay Cothren, MD, Patrick M. Osborn, MD, Ernest E. Moore, MD, Steven J. Morgan, MD, Jeffrey L. Johnson, MD, an
Pre peritoneal Pelvic Packing for Hemodynamically Unstab C. Clay Cothren, MD, Patrick M. Osborn, MD, Ernest E. Moore, MD, Steven J. Morgan, MD, Jeffrey L. Johnson, MD, and • 139 unstable pelvic fractures in 2 years • No deaths as a result of exsanguination attributed to pelvic haemorrhage • • mortality 25% vs 40% Significant reduction in blood transfusion requirements in post op 24 hrs compared with pre PPP period • independent risk factor for MOD and mortality
J Trauma 2008; 65 : 1012 -1015
Role and timing of angioembolisation • Mainstay treatment / follow up • Many authors suggest early angioembolisation can improve outcomes 1 • Some authors noted 50% mortality despite angiographic success of controlling arterial bleeding 2 • Concern of delay in getting to angiography suite, lengthy procedure • Associated morbidity • arterial injury • tissue ischemia 1. Hemodynamically unstable pelvic fractures White CE, Hku JR et al Injury 2009; 40: 1023 -1030 2. Agolini SF, Shah K, Jaffe J, et al. Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. J Trauma 1997; 43: 395– 9. Cook RE, Keating JF, Gillespie I. The role of angiography in the management of haemorrhage from major fractures of the pelvis. J Bone Joint Surg 2002; 84 B: 178– 82.
Any predicting factors for need of angioembolisation?
• Revised Trauma Score was predictive • Combination of age >60 and major pelvic fracture (butterfly, open book, vertical shear) alone was predictive (odd ratio, 15) • Fracture pattern alone is not predictive Pelvic ring disruptions: prediction of associated injuries, transfusion requirement, pelvic arteriography, complications, and mortality. Starr et al, J Ortho Trauma. 2002; 16: 553 -561 Angiographic embolisation for pelvic fractures in older patients, Kimbrel BJ et al. Tech Surg. 2004; 139: 728 -732 The value of plain radiographs in the prediction of outcome in pelvic fractures treated with embolisation therapy, Niwa T et al. Br J Radiol. 2000; 73: 945950 Predictors of death in patients with life threatening pelvic haemorrhage after successful transcatheter arterial embolisation. Hagiwara A, et al. J Trauma 2003; 55: 696 -703
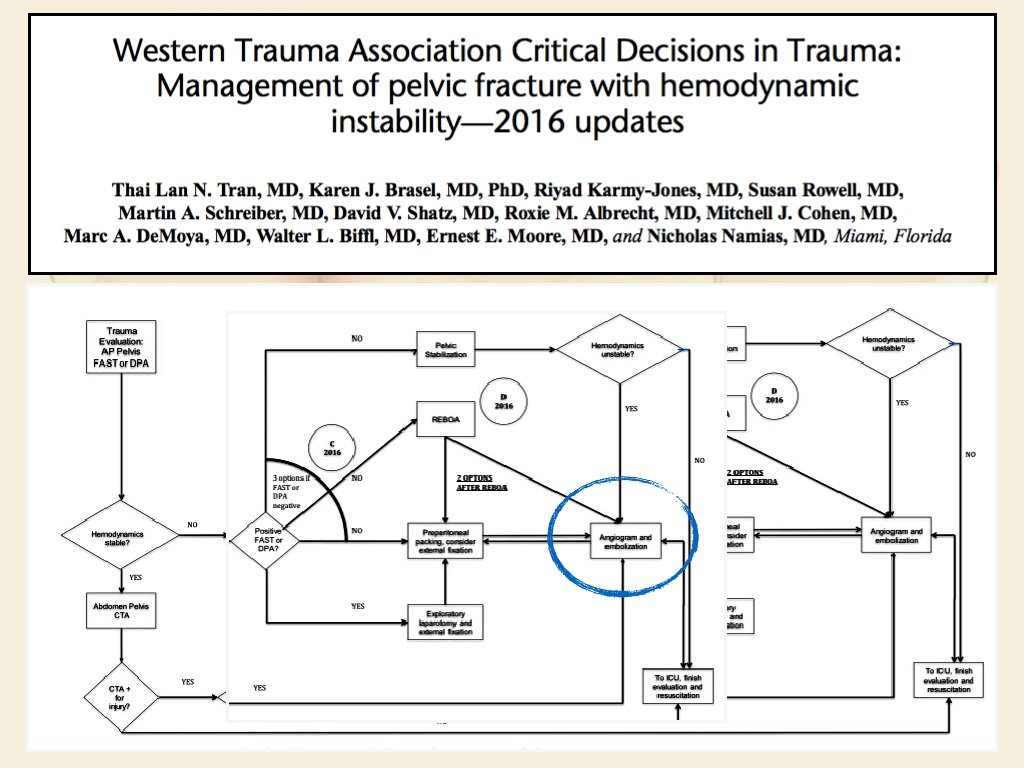
Resuscitative Endovascular balloon occlusion of Aorta (REBOA) • Temporarily control arterial haemorrhage and preserve cerebral and myocardial perfusion • Deploy in Aortic Zone 3 • Role in this algorithm is still unclear
Take home messages • Haemorrhage from pelvic fracture remains a difficult problem • Institutional guidelines has been shown to improve outcomes which should be tailored according to it’s resources • Timing and the role of angiography remains an ongoing debate with conflicting evidences
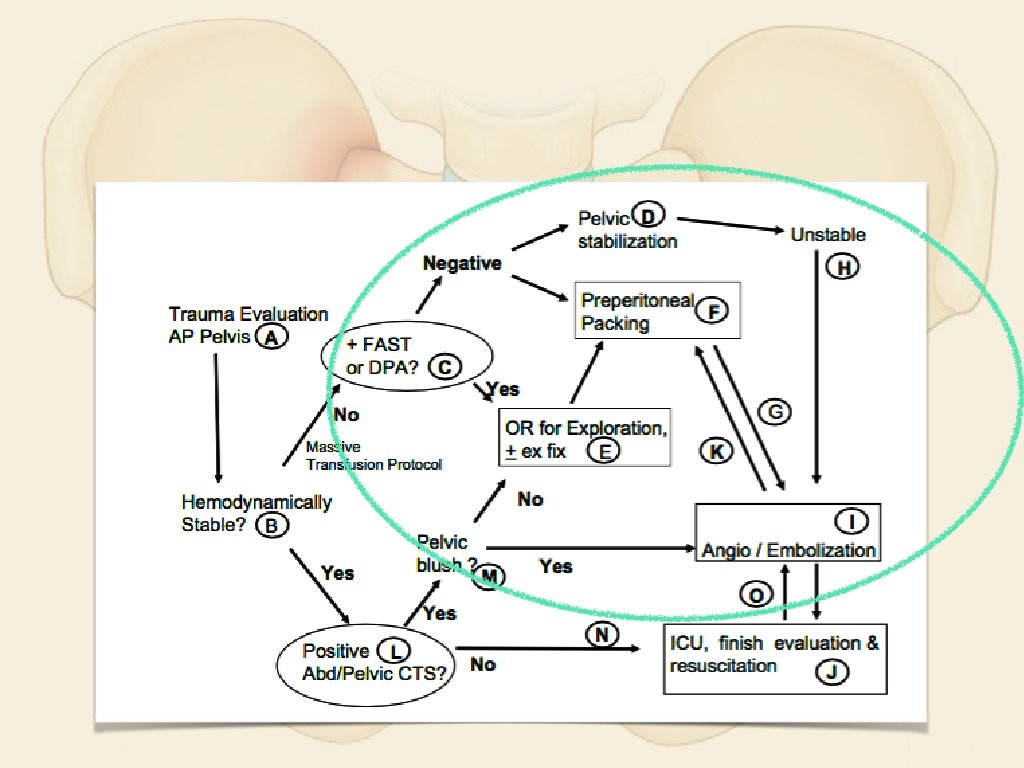
References Young and Burgess Classification of Pelvic Ring Injuries, Timothy B. Alton MD, Albert O. Gee MD Western Trauma Association Critical Decisions in Trauma: Management of pelvic fracture with hemodynamic instability - 2016 updates Pre peritoneal pelvic packing for Hemodyniacally unstable pelvic fractures: A paradigm shift Western Trauma Association Critical Decisions in Trauma: Management of Pelvic fracture with hemodynamic instability Eastern Association for Surgery of Trauma practice management Guidelines for Haemorrhage in Pelvic Fracture - Update and Systematic review Definitive Control of Bleeding from Severe Pelvic Fractures, Lewis M. FLINT, et al Angioembolization for pelvic hemorrhage control: results from the German pelvic injury register. Images https: //classconnection. s 3. amazonaws. com/33/flashcards/602033/jpg/pelvic_arteries_and_veins_(female)__sagittal_view 1314769068739. jpg http: //jksronline. org/Article. Image/2016 JKSR/jksr-74 -236 -g 002 -l. jpg http: //what-when-how. com/wp-content/uploads/2012/08/tmpd 9 b 295_thumb 2222. png http: //www. traumaready. com/wpcontent/uploads/2015/06/REBOA. jpg http: //www. lancsteachinghospitals. nhs. uk/media/images/versions/img 94 joktmu 75205. jpg? bev=2551&nocache=1428502885255 https: //upload. wikimedia. org/wikipedia/commons/thumb/6/63/RTS_Fast_Ref_Chart. jpg/800 px-RTS_Fast_Ref_Chart. jpg http: //orthoinfo. aaos. org/figures/A 00520 F 05. jpg
Thank you
Technique of Preperitoneal Pelvic Packing (PPP) • 6 -8 cm midline incision from pubic symphysis • Divide midline fascia, peritoneum intact • Retract Bladder laterally Pre peritoneal pelvic packing for Hemodyniacally unstable pelvic fractures: A paradigm shift Cothren CC, et al J Trauma 2007; 62: 834 -839
Technique of PPP • Place 3 lap pads on each side of bladder, into true pelvis below the pelvic brim • Close fascia with O-PDS • Close skin • Pack removal 24 -48 hours later Pre peritoneal pelvic packing for Hemodyniacally unstable pelvic fractures: A paradigm shift Cothren CC, et al J Trauma 2007; 62: 834 -839