Postpartum Complications Postpartum hemorrhage Definition It is defined



































- Slides: 36
Postpartum Complications
Postpartum hemorrhage Definition: • It is defined as excessive loss of blood more than 500 ml in the first 24 hr. after delivery from the genital tract at any time following baby’s birth up to the end of puerperium. • It is the main cause of maternal mortality
Types of Postpartum Hemorrhage: 1. Primary postpartum hemorrhage, which occurs during the first 24 hours after delivery. 2. Secondary postpartum hemorrhage also may be delayed, occurring more than 24 hours after delivery. It can occur as long as 6 weeks after delivery.
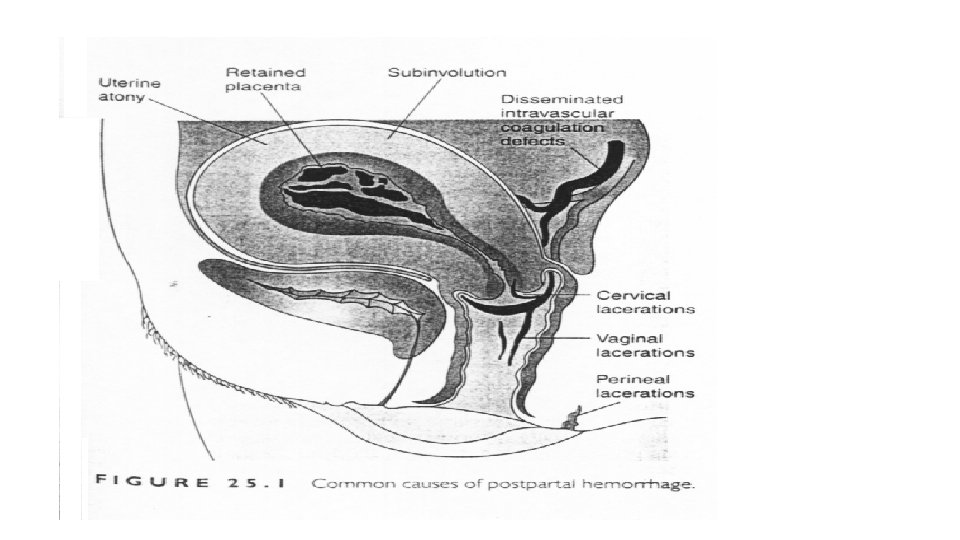
Causes of PPH: Causes: Mnemonic: 4 T's T: Tone diminished: • Uterine Atony represents 70% postpartum hemorrhage. T: Tissue: • Retained Placenta. • Placenta accreta. T: Trauma: Uterine Inversion. Uterine Rupture. Cervical laceration. Vaginal hematoma. T: Thrombin: • Coagulopathy
Predisposing Factors: 1. 2. 3. 4. Previous history of P. P. Hg. Advanced maternal age. full bladder. Multigravida: “Successive repeated pregnancy replaces muscles fibers in the uterus reducing its contractility. So blood vessels become more difficult to compress”. 5. Operative Deliveries: As forceps extraction, ventouse, and CS. 6. Over distension of uterus: as Hydraminos, large fetus and multiple pregnancy. 7. Retained placenta: incomplete delivery of placenta produce bleeding because of this retained segment receive blood Supply. 8. Heavy medication during labor as syntcinon or general anesthesia 9. Maternal anemia: Anemia is associated with debility which is a more direct cause of uterine atony. 10. Pre- eclampsia & eclampsia: due to hypertension. 11. Ketosis: for unknown causes
1 - Primary Postpartum Haemorrhage: Definition: • It is an abnormal loss of more than 500 ml of blood from genital tract occurring during first 24 hours after (delivery of fetus and affecting general condition of mother. Causes of Primary Postpartum Hemorrhage: 1. Atonic uterus. 2. Trauma "laceration or hematoma". 3. Hemorrhagic blood diseases.
1. Causes of Atonic uterus 1. General causes. 2. Local causes. 3. Nervous causes. 4. Idiopathic causes. 5. Hemorrhagic diseases. General Causes: 1. Anemia. 2. Multiparty: reducing uterus contractility. 3. Prolonged Labor: Muscles of uterus became exhausted during 1 st & 2 nd stages of labor so, Uterine muscles loose its contractility. 4. Excessive sedation and deep anesthesia: Sedation & anesthesia will depress high centers, which stimulate uterine contractility
Local Causes: 1. Over-Distension of uterus by: Hydraminos, multiple pregnancy and big fetus. Myometrium become excessively stretched and less efficient during contraction. 2. Uterine-fibroid: This impact efficient uterine action 3. Incomplete placental separation with retained fragments: If placental tissues remain partially embedded in the spongy decidua, efficient contraction and retraction is interrupted retained fragments will ooze blood so produce bleeding. 4. Presence of uterine scar: Scar will stretch fibers and tissues of uterus so it will limit its movement. 5. Blood clots or piece of membranes. 6. Rapid or precipitate labor: When uterus has contracted vigorously during 1 st & 2 nd stages of labor muscle have insufficient opportunity to retract. 7. Placenta Previa: Placental site at lowers segment so the thinner muscle layer contains few oblique muscle fibres. This result in, poor control of bleeding. 8. Abruptio-Placenta: Blood which oozed between muscle fibres interfere with uterine action.
Nervous causes: Full Bladder or Rectum reflexes inhibit uterine contractions. Idiopathic Causes: Past history of postpartum haemorrhage or ante partum haemorrhage. Hemorrhagic Blood Diseases: There are certain blood diseases, which anticipate postpartum Hg: (Leukaemia, Thrombocytopenia, and Fibrinogenemia).
Causes of Trauma during labor: 1. 2. 3. 4. 5. Difficult or precipitate labor. Birth of large baby. Instrumental delivery. Rupture uterus. Inversion of uterus due to "sudden pressure on uterus or repeated massage with CS".
Signs and symptoms of primary postpartum hemorrhage: I. General: As signs and symptoms of hemorrhage: • Tachycardia. • Hypothermia. • Pallor. • Hypotension. • Coldness. • Thirsty. • Restlessness. • Irritability. • Exhaustion and Lassitude.
II. Signs and symptoms indicated from abdominal examination: • If the bleeding is concealed: in uterus atony: 1. Uterus is boggy i. e. soft, distended, no tone. 2. Gradually enlargement of uterus. 3. Squeezing fundus will lead to gush of blood. 4. If the bleeding is revealed: in Trauma 5. Uterus is subinvoluted 6. Uterus is hard, firm, and well contracted 7. Uterus is large.
III Signs and symptoms indicated from vaginal Examination: • In case of Trauma. 1. Cervical birth canal laceration or injury. 2. Bleeding will be bright red in color. 3. Bleeding will be dark red in retained fragments. Diagnostic Measures for primary postpartum haemorrhage: 1. C. B. C. "Complete Blood Count". 2. Cross- matching & blood grouping test. 3. RH- factor test.
Nursing Management of Primary Postpartum Hemorrhage : * Preventive measures During ante partum period: 1. Complete history should be taken to identify high-risk patients who are likely to develop PPH. 2. Improvement of health status specially to raise the hemoglobin level. 3. Hospital delivery of high-risk patients who are likely to develop PPH. e. g. polyhydraminios, multiple pregnancy, grand multiparous, APH and severe anemia. 4. Routine blood grouping and typing for immediate management during emergency. 5. woman who has hemorrhagic blood diseases should give antifibrinolytic factors.
During Intra-partum period: 1. Proper management during labor including: • • Proper assessment. Careful observation for mother and baby. Avoid misuse if oxytocin. Avoid bearing down in 1 st stage. Empty bladder every one hour. Unhurried in delivery of placenta. Prevention of tear by careful episiotomy – support perineum – maintains flexion. 1. Assessment for amount of bleeding.
2. Careful administration of sedatives and analgesic drugs. 3. Prophylactic administration of oxytocic drugs with delivery of anterior shoulder or at the end of third stage. 4. Avoid massaging the uterus before separation of the placenta. 5. Examine the placenta and membranes for completeness. 6. Examine the utero-vaginal canal for trauma and prompt repair if present. 7. Effective management of the fourth stage of labor. 8. No forceps or breech delivery before fully dilatation of the cervix.
Management Control bleeding through the following steps: • Uterine massage. • Exploration of uterus under general anesthesia. • Bimanual compression (Uterus is firmly squeezed between 2 hands). • Tight intrauterine packing to exert direct homeostatic pressure on the open uterine sinuses and to stimulate uterine contractions. • If all the above measures fail to achieve homeostasis a hysterectomy is performed. • In traumatic PPH speculum, examination to find out trauma and homeostasis is achieved by appropriate sutures.
Observation of the Mother: • Record pulse and BP every 15 minutes. • Palpate uterus every 15 minutes to ensure that it is well contracted. • Check temperature 4 hourly. • Examine lochia for amount and consistency. • Examine IV infusion. • Intake and output chart. • Relieve anxiety by explaining her condition and administer prophylactic antibiotics prescribed considering the risk for infection.
Secondary postpartum Haemorrhage: Definition: • It is bleeding which is occurring after the first 24 hours of delivery and up to the end of puerperium Causes of secondary Postpartum Hemorrhage: 1. Retained products of conception as: • Placental fragments. • Accessory lobe. • Placental polyp. • Retained piece of membranes. • Blood cots. • Infection: It is due to separation of septic through site of bleeding: • Placental site. • Caesarian wound. 1. Cervix.
3. 4. 5. 6. Subinvolution of uterus. Choriocarcianoma. Inversion of Uterus Local gynaecological lesions as: • Cervical erosion • carcinoma in Cervix 7. Haemorrhagic blood diseases as: • Leukemia • Thrombocytopenia.
Signs and symptoms of secondary Postpartum Haemorrhage: • General: Tachycardia • and Low grade fever. • Abdominal examination: • Subinvolution of uterus. • Vaginal examination: • Lochia heavier in amount, • fresh in color & offensive • in odor. If infection occurs • retained placenta may • present.
Nursing Management for secondary Postpartum Haemorrhage: • • Call the Doctor. Massage fundus if it is still palpable. Express any clots. Encourage mother to empty her bladder. Give an oxytocin drug as Ergometrine I. V or I. M route. Keep all pieces & lines to assess volume of blood loss. In case of retained products of conception, the patient is given Ergometrine & antibiotic if the bleeding is slight. The products are examined histological to exclude Choriocarcianoma.
Complications of postpartum hemorrhage: • Postpartum shock. • Sheehan’s syndrome
Postpartum Complications Immediate Postpartum complications. 2. Puerperal Infection Description Puerperal infection: • It is elevated the temperature of 38 c or higher after the first 24 hours postpartum on any two of the first 10 postpartum days. • Although a slight fever may occur during the first hours due to dehydration or exertion of labor due to absorption of some waste product of the fetus during delivery and in the 3 rd day due to milk secretion.
Causative organisms 1. Aerobic organisms include beta- hemolytic streptococci, staphylococcus aurous, E. coli 2. Anaerobic organism include clostridium perfringens 3. Microorganisms that can transmit through sexual contact include: Chlamydia trachomatis, Neisseria gonorrheae, and Mycoplasma hominis.
b- Genital tract infections • Endometritis: Inflammation of the endometrium (The inner layer of the uterus). • In most cases of endometritis, the bacteria responsible for pelvic infections are those that normally reside in the bowel, vagina, perineum, and cervix. • Episiotomy • Thrombosis • Mastitis
General Risk Factors: 1. 2. 3. 4. 5. 6. 7. 8. 9. Anemia. Poor nutrition. Lack of prenatal care. Obesity. Low socioeconomic status. Immunosuppression. Diabetes Exhaustion Preexisting pelvic infection
II. Labor Management: 1. Prolonged labor. 2. Prolonged rupture of membranes. 3. Intrauterine fetal monitoring. 4. Frequent cervical examination (Sterile gloves should be used in examinations. 5. Hemorrhage. 6. Retained placental fragment. 7. Intrauterine manipulation. 8. Infection control practice during different stage of labor. Internal fetal monitoring
Clinical manifestations 1. Localized vaginal, and perineal infection: pain, elevated temperature, edema, redness, tenderness and discharge from wound 2. Endometriosis: is the most prominent of these infections. Endometritis is much more common if a small part of the placenta has been retained in the uterus. 3 - Malaise, headache, general discomfort, loss of appetite, large and tender uterus, brownish, red and foul lochia Anorexia, 4 - Suppressed milk secretion Rapid pulse and respiration, elevated body temperature and nay associated with chills
Diagnostic measures for puerperal sepsis: • Blood cultures. • Uterine and / or high cervical cultures. • CBC (complete blood count). • Fasting Blood Sugar. • Urine Analysis. Treatment 1. Antibiotics 2. Bed rest; semi-fowler’s position 3. Supportive therapy 4. Increased fluid intake 5. Aseptic precautions
Prevention of puerperal infection During antenatal period 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Good antenatal care Treatment the vaginal, cervical and sexual transmitted disease, UTI Correct the anemia Eat balance diet, and increase fluid intake Good perineal hygiene Detect and manage diabetic Avoid contact with persons having communicable diseases Hospital delivery of high risk group. Improve standards of maternity services. Follow up and health education. Maintain good personal hygiene
During labor • Used a aseptic technique as hand-washing, gown , sterile equipments , clean delivery area • Administer prophylactic antibiotics as a preemptive strike against infectious bacteria when the membrane rupture • Avoid prolongation of labor by early maternal referral • Prevention of unnecessary or excessive vaginal examination • Avoid unnecessary ( routine ) episiotomy • Encourage voiding and avoid unnecessary catheterization • Good management of placenta separation • Isolate women with infection. • Replace excess blood loss to improve general body resistance. • Isolate women with infection
During postnatal health education before discharge regarding diet , prevention of infection, thrombosis • Administer antibiotic as order • Good wound care • Check vital sign and urine output q 6 hrs • Offer a balanced diet that rich in protein and vitamin C , frequent fluid and early ambulation • Correct anemia • Avid contact with people with respiratory infects • Educate the mothers appropriate aseptic technique as hand washing , breast care , perineal care • Avoid too many visitors. • Frequent changing of sanitary pads.
Nursing interventions 1. Promote resolution of the infectious process a. inspects the perineum 2day for redness, edema, ecchymosed and discharge b. evaluation for abdominal pain, fever, malaise, tachycardia, and foul smelling lochia c. obtain specimens for laboratory analysis report the finding d. offer a balance diet, frequent fluids and early ambulation e. administer prescribe antibiotic 2. Provide client and family teaching a. describe and demonstrate self- care b. stress careful perineal hygiene and hand washing c. inform the client about infection ( sings , causes and treatment) 3. Positioning the woman in semi fowler’s position to help drain lochia.
4. If infection occur continues monitoring 5. If isolation need a. support and encourage the mother (always reports her baby condition, allow family visit with used aseptic technique b. Encourage adequate rest c. Allow her to express her feeling and concern , d. Increase fluid intake 10 cup/day, and eat rich diet with vitamins as B 11, B 6, B 12, Vitamin C