KEGAWATAN THT Kegawatan THTKL Corpus Alienum n Otalgia






 n")
 Esofagoskopi / n S. PIRIFORMIS")







, cedera karena alat instrumen & ledakan")
 Fraktur Longitudinal→ facial")
, raccoon eyes,")
 to noise n SHNL, tinnitus n Avoidance/")













 n Local Trauma /Nose picking or blowing / surgery Dry air")




















 n Reduksi Fraktur n Stabilisasi Plat and")

")

 Periorbital swelling & pain,")









 Indikasi terjadinya sumbatan jalan nafas(Choking) adalah: ² Tidak dapat bicara")















- Slides: 87
KEGAWATAN THT
Kegawatan THT-KL Corpus Alienum n Otalgia n Abses di bagian THT n Trauma n Komplikasi akibat infeksi THT KL n
BENDA ASING DI THT
ANAMNESIS & PEMERIKSAAN FISIK Umur n Lokasi nyeri n Sesak nafas n Stridor n Disfagia n
PRINSIP BENDA ASING TINDAKAN SEGERA KELUARKAN
PEMERIKSAAN PENUNJANG Harus sesuai indikasi n Foto esofagus n Foto thoraks n Foto jaringan lunak leher n
BENDA ASING DI. . . n LARING Perasat Heimlich / Laringoskopi (Stridor, disfonia) n TRAKEA (Mengi) n BRONKUS Bronkoskopi atau Torakotomi (dispnea, atelektasis a/ emfisema) Bronkoskopi
BENDA ASING DI. . . n ESOFAGUS pembedahan (Disfagia) Esofagoskopi / n S. PIRIFORMIS Laringoskopi n DASAR LIDAH Direct/indirect Laringoskopi
BENDA ASING DI. . . n FARING/TONSIL Ekstraksi Cunam n HIDUNG Ekstraksi dengan pengait n LIANG TELINGA narkosis Ekstraksi dengan/tanpa
NYERI TELINGA AKUT
Anamnesis + Pemfis Nyeri telinga Rasa penuh di telinga Riwayat ISNA Penyakit Sistemik Membran Timpani OMA OE Sirkumskrips OMA OE. Sirkumskrip OE. Difus OE. Maligna Nyeri sendi temporomandibular Nyeri alih / psikogenik OE Difus Tindakan Segera Analgetik Darinase Pus Pem. Penunjang Uji Pendengaran Uji Mikrobiologik Foto Ro. Mastoid OE Maligna Nyeri TMJ Nyeri Alih Nyeri psikogenik Antibiotik Miringotomi/parasintesis Ventilasi (grommet) Pengobatan penyebab Salep pemanas (ichtiol) Antibiotik topikal Antibiotik Sistemik Insisi Bersihkan liang telinga Antibiotika topikal Antibiotika sistemik Steroid topikal Anti pseudomonas dosis tinggi 6 minggu (iv) Terapi anti diabetes Pengobatan penyebab
Corpus Alienum Telinga n n n Serangga Cotton, kertas, organic material Small batteries GK : Discomfort & agitation Secondary complications: infection & mucosal erosion
Corpus Alienum Telinga n n n Matikan serangga tetesi liang telinga dengan minyak/gliserin/AB tts telinga Gunakan Forceps/Hook/pingset untuk mengeluarkan CA Irigasi/spuling telinga ( do not use if organic FB
Hematoma Aurikula n n Biasanya akibat trauma Pembengkakan berfluktuasi kebiruan di daun telinga R/ : Drainase - Aspirasi jarum - Insisi dan drain Bebat Tekan
Rupture membran Timpani n n n Kompresi (tempeleng), cedera karena alat instrumen & ledakan ( blast injuries) D/ - anamnesis - Otoskopi - Hearing test R/ Konseratif -Paper patch - Surgery
Fraktur Os Temporal n n n Cedera kepala (Blunt head injury) Fraktur Longitudinal→ facial n. paralysis, CHL (ossicular chain disruption) Fraktur. Transverse → SNHL, dysequilibrium, CN VII palsy
Fraktur Os Temporal n n Battle’s sign (bluish discoloration of postauricular region), raccoon eyes, hemotympanum, hearing loss, dizziness, CSF otorrhea, CN VII palsy CT temporal bone
Trauma Akustik Sudden exposure (impact or blast) to noise n SHNL, tinnitus n Avoidance/ ear protection n Corticosteroids, carbogen, vasodilators, diuretics, anticoagulants, plasma expanders n
Otitic Barotrauma n n n Gangguan fungsi ventilasi telinga tengah Disfungsi Tuba eusthachius Terjadi peningkatan tekanan udara(descent in flight / scuba diving) Dapat menyebabkan hemotympanum
Derajat Barotrauma Grade o = Normal ear n Grade 1 = MT Hiperemis, retraksi n Grade 2 = MT Petechiae, Hiperemis n Grade 3 = MT hematoma, Bluesness n Grade 4 = Free Blood in The middle ear (Hemotympanum) n Grade 5 = MT Perporasi/Ruptur, Free blood in external ear n
Barotrauma n n Repeated Valsalva maneuver R/ AB, Corticosteroid R/Topical nasal/oral decongestants Myringotomy & Grommet tube insertion may be needed
Sudden Hearing Loss n n SNHL ≥ 30 d. B over 3 contiguous frequencies within 3 days or less Etiology : Viral & Infectious, Vascular, Trauma, Autoimmune, Neurologic
Komplikasi infeksi Telinga Tengah n Extracranial
Acute Mastoiditis n n n preceded by AOM young children severe pain, fever, edema over mastoid area intravenous ATB Myringotomy ± PE tube
Subperiosteal Abscess n n pinna pushed down & outward intravenous ATB Insisi & Ddrainase R/ Mastoidectomy AB/Analgetik/ Cortikcosteroid
Komplikasi telinga Tengah n Intracranial
Corpus Alienum Hidung n n S/ Purulent unilateral nasal discharge D/ Usually lodge on the floor of anterior or middle third
Corpus Alienum Hidung n n n Good visualization: headlamp & nasal speculum R/ Ekstraksi CA : Alligator forceps should be used to remove cloth, cotton, or paper Other hard CA are more easily grasped using bayonet forceps or Kelly clamps, or they may be rolled out by getting behind it using an ear curette, single skin hook, or right angle ear hook
Nasal Fracture n n Trauma hidung : Jatuh. KLL, Pukulan/Tinju Deformitas hidung Edema hidung, ecchymosis, epistaxis Close or open reduction
Abses/Hematoma Septum nasi n n n Trauma, surgery Soft, fluctuant swelling of septum Aspirasi jarum or Insisi dan drainase Tampon hidung bilateral selama 2 -3 hari AB profilaksis
Abses/Hematoma Septum Nasi Insisi dan Drainase Press Septum
Epistaxis (=Perdarahan Hidung) n Local Trauma /Nose picking or blowing / surgery Dry air / Irritants Topical medications (steroids) Foreign body Tumor / polyp n Systemic Blood diseases Hereditary hemorrhagic telangiectasia Drugs (anticoagulants) Hypertension
Sumber perdarahan
Epistaxis n n Initial first-aid Assessment of blood loss Evaluation of cause Procedure to stop bleeding n n Most common → Kiesselbach’s Plexus Squeeze nose 5 -20 mins Insert cotton pledget (with decongestant) Cautery with silver nitrate
Epistaxis First Aid n Conservative Management n n Pinch soft part of nose Lean forward and breathe through mouth Ten minutes Protect yourself n n n Gown Gloves Mask
Treatment n Identifiable Vessel n Nasal cautery n Examine nose n Identify vessel n Apply 1 in 10, 000 adrenaline and 1%lignocaine on cotton wool pledget n Silver nitrate cautery of vessel
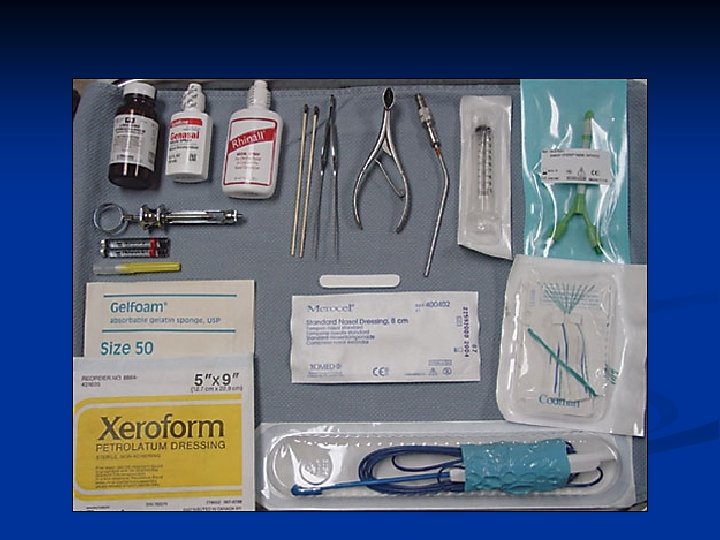
q No Identifiable Vessel Anterior nasal packing n. Local anesthetic & decongestant n. Nasal packing - Vasaline guaze - Absorbable gelfoam - Oxidized cellulose (Surgicel) - Nasal tampon
Anterior nasal packing
Anterior nasal packing n Nasal packing - Vasaline guaze - Absorbable gelfoam - Oxidized cellulose (Surgicel) - Nasal tampon
Anterior nasal packing n Nasal packing - Vasaline guaze - Absorbable gelfoam - Oxidized cellulose (Surgicel) - Nasal tampon
Anterior nasal packing n Nasal packing - Vasaline guaze - Absorbable gelfoam - Oxidized cellulose (Surgicel) - Nasal tampon
Figure 2 Correct insertion of a nasal tampon (note that the direction is along the floor of the nasal cavity). Pope, L E R et al. Postgrad Med J 2005; 81: 309 -314 Copyright © 2005 BMJ Publishing Group Ltd.
Posterior nasal packing n n Topical anesthetic & decongestant Posterior nasal packing Double balloon device Foley catheter
Posterior nasal packing n n Topical anesthetic & decongestant Posterior nasal packing Double balloon device Foley catheter
Posterior nasal packing n n Topical anesthetic & decongestant Posterior nasal packing Double balloon device Foley catheter
Surgical Intervention Septoplasty n Sphenopalatine artery ligation n Anterior ethmoid artery ligation n Maxillary artery ligation n External carotid artery ligation n
Figure 1 Epistaxis management protocol. Pope, L E R et al. Postgrad Med J 2005; 81: 309 -314
Fraktur Le Fort : Le Fort I Garis fraktur berjalan/meluas dari septum nasal ke lateral rima piriformis, berjalan horizontal diatas apikal gigi, melintas dibawah zygomaticomaksilary junction, dan memotong pterygomaksilary junction untuk memotong pterygoid plates.
Le Fort II Fraktur berbentuk piramid dan meluas dari nasal bridge tepat atau dibawah sutura nasofrontal melalui prosesus frontal pada maksila, pada inferolateral melalui os. lakrimalis dan lantai orbita inferior dan rima melalui atau mendekati foramen orbita inferior. Pada inferior melalui dinding anterior sinus maksilaris kemudian melintas dibawah zigoma, memotong fissura pterigomaksilaris dan melalui pterygoid plates.
Le Fort III Garis fraktur dimulai dari sutura nasofrontal dan frontomaksilaris dan meluas ke posterior sepanjang dinding medial orbita melalui nasolacrimal groove dan os. etmoid. Fraktur berlanjut sepanjang lantai orbita di sepanjang fissura orbita inferior dan berlanjut superolateral melalui dinding lateral orbita, melalui zygomaticofrontal junction dan arkus zigomatikum. Intranasal, cabang fraktur meluas melalui dasar lamina perpendicular etmoid, melalui vormer, dan melalui penghubung pterygoid plates ke basis sfenoid.
Manifestasi Klinis Le Fort II Le Fort I Ø Gejala klasik “open bite” Ø Dapat berupa fraktur impaksi, immovable, atau segmen melayang. Ø Hipostesia pada nervus infraorbital Ø Fraktur maksila unilateral Ø Ekimosis pada palatum Ø Maloklusi Ø Pergeseran fragmen fraktur. Ø Guerin’s sign Ø Manifestasi klasik : “Raccoon sign” Ø Hipostesia nervus infraorbital Ø Maloklusi, sering berkaitan dengan ”open bite”. Ø Deformitas dapat terpalpasi pada area rima infraorbita maupun pada sutura nasofrontal. Ø Rinorea cairan serebrospinal Ø Epistaksis Le Fort III Ø Ø Ø Ø Gejala klasik ”dish face” Mobilitas kompleks zigomatikomaksilaris Kebocoran cairan serebrospinal Edema Ekimosis periorbita Masalah visual Perdarahan subkonjungtiva Epifora.
Pemeriksaan Penunjang Foto Polos : Foto polos kepala lateral Temuan pada foto polos : n Foto polos kepala AP Opasitas pada sinus maksila, n Water’s view (film sinus) pemisahan pada rima orbita inferior, sutura zigomatikofrontal dan daerah nasofrontal. n Foto polos servikal lateral n Dari film lateral dapat terlihat fraktur pada lempeng pterigoid
Penatalaksanaan Manajemen Umum n Fiksasi Maksilomandibular (MMF) n Reduksi Fraktur n Stabilisasi Plat and Screw n Cangkok Tulang Primer n Pelepasan Fiksasi Maksilomandibular (MMF) n Resuspensi Jaringan Lunak n
KOMPLIKASI SINUSITIS Orbital complications n Intracranial complications n
Classification of orbital inflammation Stage I II IV V Inflammation Inflammatory edema (periorbital cellulitis) Orbital cellulitis Subperiosteal abscess Orbital abscess Cavernous sinus thrombosis
Complications of sinusitis n n Periorbital cellulitis: periorbital erythema, edema, pain & fever Purulent nasal discharge S. pneumoniae, S. aureus, coagulase-negative staphylococci Broad-speculum antibiotics
Complications of sinusitis n n n Orbital complications (stages II-V) Periorbital swelling & pain, fever Proptosis, chemosis, restriction of ocular movement & visual disturbance
Complications of sinusitis n n n CT scan → subperiosteal & orbital abscess Admission & IV broadspectrum antibiotics Surgery (drainage) if - failed medication - develop abscess - visual drop
Complications of sinusitis Intracranial complications n Cavernous sinus thrombosis, meningitis, extradural abscess, intracranial abscess & subdural empyema n Purulent rhinorrhea, fever, frontal/retroorbital headache n Personality change/lethargy, seizures, N/V, focal neurological deficits
Complications of sinusitis Intracranial complications n Diagnosis → MRI scan with gadolinium n Admission, IV broad-spectrum antibiotics & surgical drainage
Corpus Alienum oropharyx n n Peanuts, coins, batteries, fish bone, meat & bone fish pieces, dentures Location of pain indicates CA
CA Oropharyx n n Fish bones tend to lodge in oropharynx, produced ipsilateral symptoms Esophagus FB localize in midline: dramatic acute dysphagia
Corpus Alienum Esofagus n n n Most CA in esofagus can be identified CA Esophageal : pooling of saliva in piriform X-rays may be helpful in radio-paque objects
Corpus Alienum Esofagus n n Visualized CA can be removed with angled forceps Sharp CA should be removed at the earliest opportunity due to risk of perforation
Corpus Alienun Esofagus n. Coins → removed if in cervical or mid esophagus → removed within 12 hrs if in distal esophagus (ESOFAGOSKOPI) n. Batteries → removed emergency
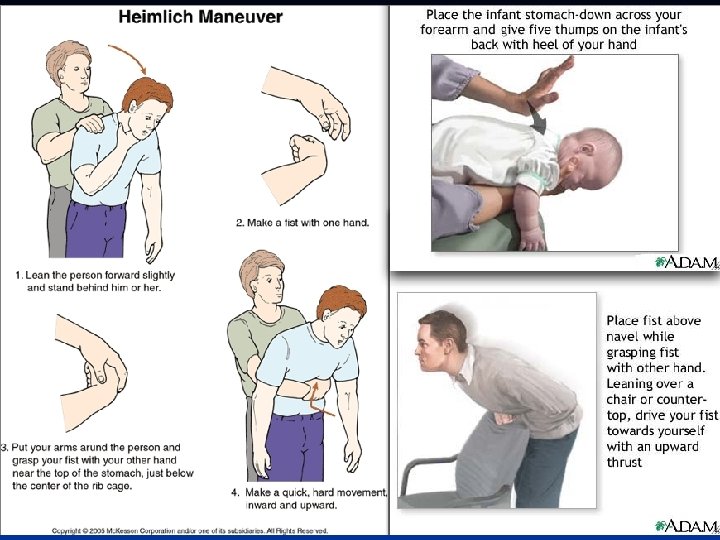
CORPUS ALIENUM LARYNX (CHOKING) Indikasi terjadinya sumbatan jalan nafas(Choking) adalah: ² Tidak dapat bicara dan atau berteriak ² Muka menjadi kebiruan ² Memegang tenggorokan dgn mulut terbuka ² Batuk lemah, susah bernafas, suara dgn frekwensi tinggi ² Bisa tidak sadar (pingsan- Die)
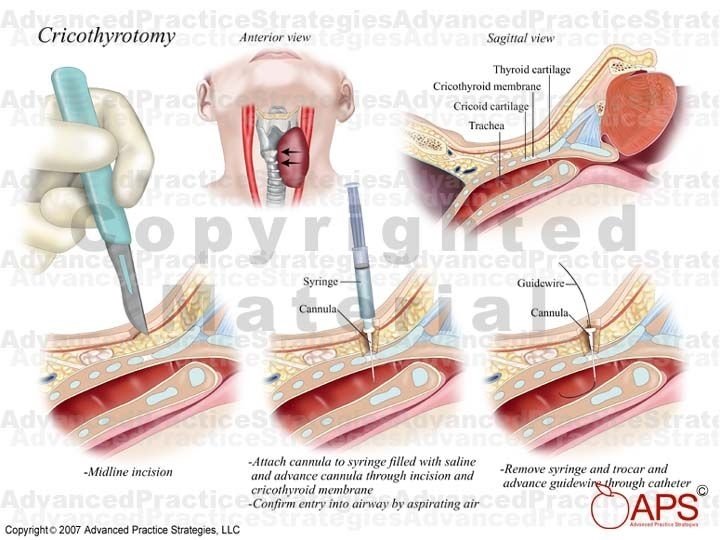
Penanganan Heimlich Manuever n Cricothyrotomy n Tracheostomy n Laryngoscopy Direct + Extraksi CA dgn Forceps n
Tracheostomy
Corpus Alienum Bronchus n n n Sudden onset of coughing, wheezing or stridor in previously healthy child Unilateral wheezing, poor chest movement & reduced breath sound Chest X R: hyperinflate, infection, collapse
Corpus Alienum Bronchus n n n Heimlich manuver Secure airway Endoscopic removal under general anesthesia
Airway Obstruction n Neonatal : Congenital tumors, cysts, webs : Laryngomalacia : Subglottic stenosis Children : Laryngotracheobronchitis : Supraglottitis (epiglottitis) : Foreign body : Retropharyngeal abscess : Respiratory papilloma Adults : Laryngeal cancer : Laryngeal trauma : Epiglottis & deep neck infection
Deep neck infections
Peritonsillar abscess n n Pus forms between tonsils capsule & superior constrictor Group A Streptococcus
Peritonsillar abscess n n n Severe, unilateral sore throat fever Hot potato voice Uvula deviates to opposite side Swollen tonsils
Peritonsillar abscess n n n CBC, throat C/S Antibiotics - Oral - Parenteral needle aspiration or I&D
Ludwig’s Angina n n n Rapid swelling cellulitis of sublingual & submaxillary spaces Dental infection, floor of mouth, salivary gland Fever, edema & erythema of neck under chin & floor of mouth
Ludwig’s Angina n n n Open mouth, Tongue → upward & backward→ airway obstruction Streptococci, Bacteroides, S. aerues Tracheostomy IV antibiotic I&D, tooth extraction
Epiglottitis n n n Age 3 -7 yrs old H. influenzae type B, Group A Streptococcus severe sore throat & fever, dysphagia, drooling Stridor Inspiratoar Breathing with raised chin & open mouth
Epiglottitis n n n CBC: leukocytosis Film lateral neck → thumb shaped epiglottis Avoid tongue depressor Controlled intubation Intravenous ATB
Retropharyngeal Abscess n n n Infants & children Secondary to oropharyngeal infection Severe dysphagia & respiratory distress airway observation IV antibiotic Surgical drainage ( prevent pus aspiration)
TERIMA KASIH