TIROID dr Christin Rony Nayoan Sp THTKL Departemen







 –deteksi")









 • Subtotal")

- Slides: 21
TIROID dr. Christin Rony Nayoan, Sp. THT-KL Departemen IKTHT –KL FKIK UNTAD
C 5 - Th 1 Wanita > Membesar dalam kehamilan dan haid Berat 25 gram
HISTOLOGI STRUKTUR TIROID
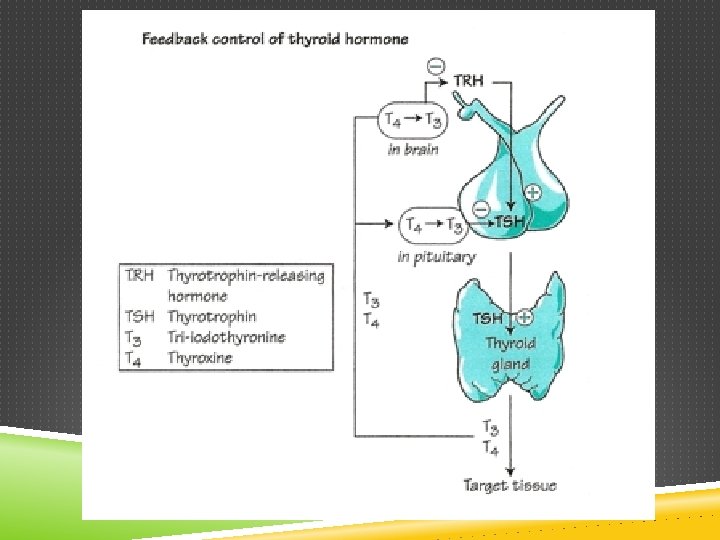
FISIOLOGI
STEPS OF THYROID HORMONE SYNTHESIS 1. IODINE TRAPPING 2. OXIDATION 3. IODINATION 4. COUPLING 5. STORAGE 6. RELEASE
§ Generally, THs: 1. Increases metabolic rate. § 2. Stimulates increased consumption of glucose, fatty acids and other molecules. Increases metabolic heat, by mitochondrial no & activity ATP, 3. Stimulates rate of cellular respiration by: § § § Production of uncoupling proteins. Increase active transport by Na+/K+ pumps. Stimulates O 2 consumption of most of cells in the body.
NODUL TIROID Insiden meningkat seiring usia 2015 650 – 70 % ( jerman) –deteksi probe scanners banyak pada wanita 55 % tidak terpalpasi 33 % ca tiroid tdk terpalpasi ultrasound , pembedahan atau otopsi
EPIDEMIOLOGY Nodules removed surgically – 42 -77 % Colloid nodules – 15 -40% Adenomas – 8 -17% Carcinomas
PREVALENSI KEGANASAN Papillary - 70% Follicular - 15% Medullary - 5 -10% Anaplastic - 5% Lymphoma - 5% Metastatic – rare –Breast, lung, renal, GI, melanoma
CLINICAL EVALUATION High risk factors for thyroid cancer –Head and neck irradiation (including XRT for breast) –Family history of thyroid cancer (Medullary, Gardner’s, Cowden Syndrome) –Dysphonia or dysphagia –Rapid growth –Associated neck masses • 71% of these patients with one or more risk factor had thyroid cancer
PHYSICAL EXAM Complete head and neck exam • Bimanual palpation of thyroid gland cervical chain of lymph nodes Laryngoscope: • Evaluate for vocal cord mobility and symmetry
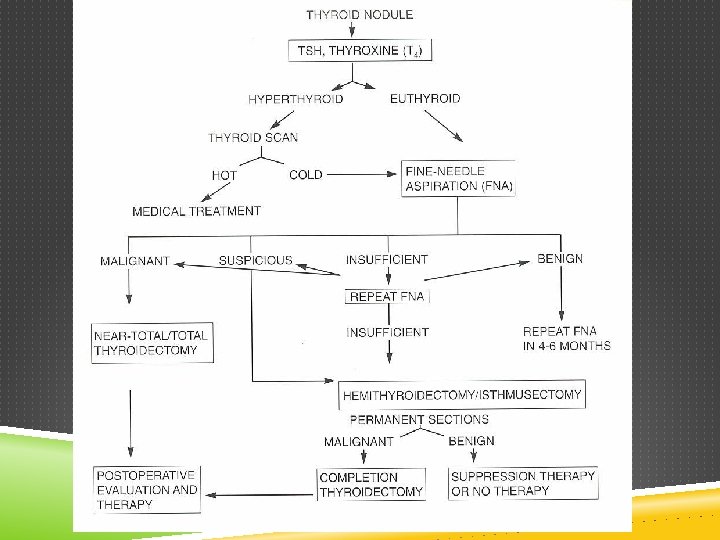
LABORATORY EVALUATION Obtain serum TSH in all patients with nodules If TSH is low, measure free T 4 and T 3 –May be an autonomous nodule or toxic multinodular goiter –May be a cold nodule in the setting of hyperthyroidism –High TSH would suggest Hashimoto’s or other thyroiditis (thyroid antibody may be useful)
INITIAL RADIOGRAPHIC EVALUATION Ultrasound -Identifies multiple nodules -Used to improve accuracy of FNA -Characterizes nodules to stratify FNA
OTHER THYROID IMAGING CT or MRI of Neck –Not useful for evaluation intrathryoidal nodules –Useful for evaluation of local compressive symptoms
NUCLEAR MEDICINE THYROID SCANNING Performed to evaluate nodule function Technetium-99 versus Iodine • 5% of nodules that “trap” Tech-99 are “cold” on iodine scan Most useful in patients with hyperthyroidism Before routine use of FNA – Scan + U/S were tests of choice for evaluation of nodules
FNA Nodules greater than 1 cm • Nodules with suspicious characteristics on ultrasound • Irregular margins • Calcifications • Intranodular hypervascularity Clinical utility of FNA • Easy to perform, cost effective and well-tolerated • Accurately identifies papillary carcinoma in most cases • Accurate for benign diagnoses • False positive rate - 1% • False negative rate - 5%
THERAPIES FOR THYROID NODULES Surgery • Hemithyroidectomy (risk recurrence in multinodular goiter) • Subtotal or total thyroidectomy L-thyroxine • Considered for nodules in hypothyroid and euthyroid patients I-131 • Considered for nodules in hyperthyroid and euthyroid patients
THANK YOU