Early and definitive treatment of pilon fractures AO










 Medial Posterolateral (Volkmann’s)")
























 • Direct articular reduction •")
- Slides: 39
Early and definitive treatment of pilon fractures AO Trauma Advanced Principles Course
Learning objectives • Formulate a preoperative plan including rationale for imaging, choice of approach, and surgical tactics • Compare the pros/cons of conventional and locked plating and external fixator and describe reduction techniques and tools • Evaluate the role of bone graft substitutes for periarticular defects • Identify common complications • Explore key outcome publications
3
43 B 2 43 C 2 43 B 3 43 C 1
Treatment options • Plaster immobilization • Ankle-spanning external fixator • Articulated external fixator • Limited internal with external fixator • Hybrid ring/small wire external fixator • Open reduction and internal fixation (ORIF)
Staged protocol for ORIF • Patterson et al, 1999 • Sirkin et al, 1999 • 22 C 3 pilon fractures • 56 pilon fractures • Average 24 days to ORIF • Average 14 days to ORIF • No infections • 5. 3% infections
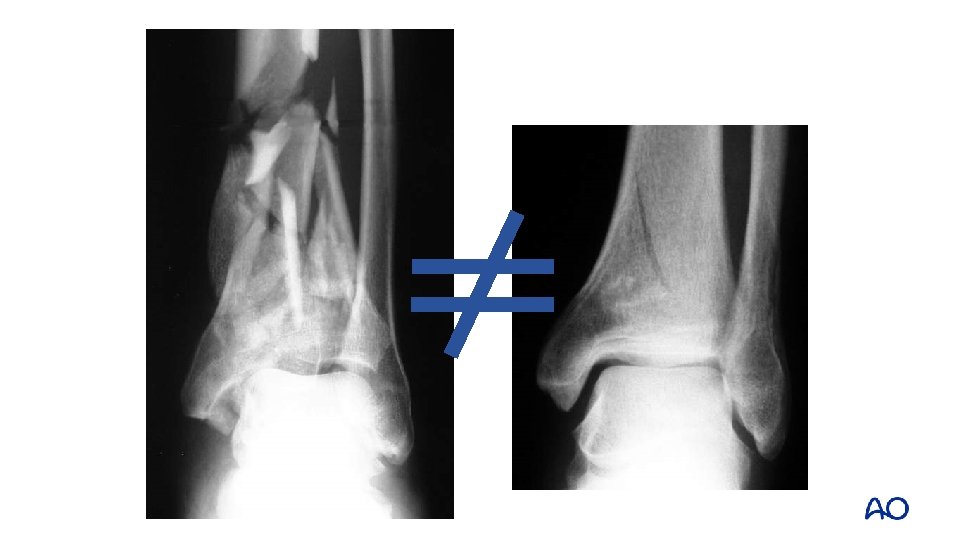
Timing is… Everything!
Bicolumnar posterior distraction Spanning external fixator—medial and lateral to control deformity and reduce the talus correctly
Talus centered
Tension Compression Intact Beware
Fracture pattern—articular Anterolateral (Chaput) Medial Posterolateral (Volkmann’s)
Metadiaphyseal spike • • Often the metadiaphysis can be reduced first This large metadiaphyseal spike may help determine surgical approach as well
Small posterior segment/comminution
Coronal plane Sagittal plane
Direct articular reduction • • Must be anatomical Visualization and reduction are aided by distraction
Reduction assessed on both the AP and lateral views
• • Reduction is improved Lag screws are placed across major articular fracture lines
Reduction strategy • Fix to posterolateral fragment • Rotation of posterolateral fragment • Medial to posterolateral • Central impaction • Anterolateral fragment • Secure articular segment • Span joint to diaphysis
Metadiaphyseal spike • • Often best to fix a large spike directly Allows the joint to be fixed to this fragment
Small posterior segment/comminution Small posterior fragment requires a posterolateral or posteromedial approach
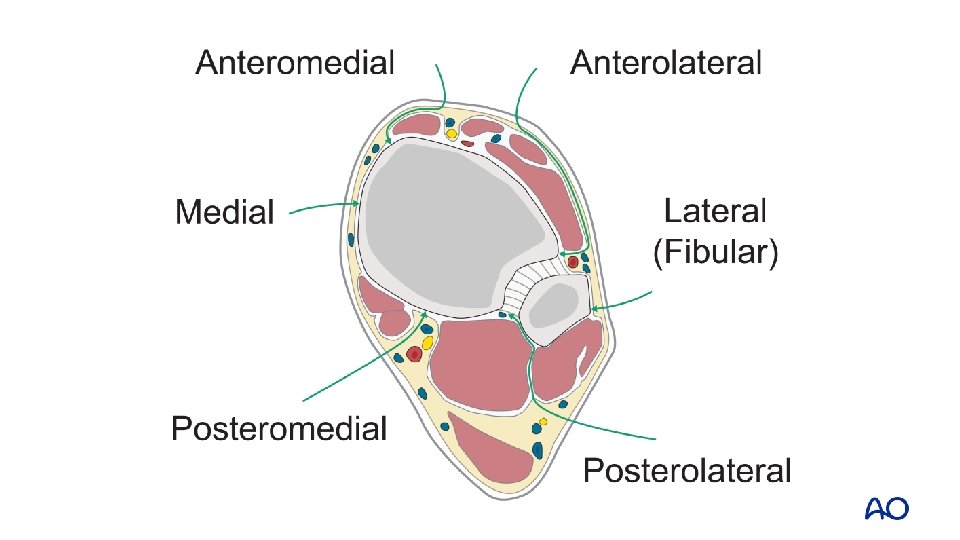
Anteromedial approach • Lateral to tibial crest • Medial to tibialis anterior • Preserve paratenon • Curve at ankle
Anteromedial approach
Anterolateral approach • In line with the 4 th metatarsal • Exposure onto the talar neck • Proximal: superficial peroneal nerve Identify and protect the superficial peroneal nerve!
Anterolateral approach Allows for visualization in the joint as far medial as the medial shoulder, but no further
Anterior fracture line When the anterior fracture line exits medial to the medial shoulder, the anteromedial approach is indicated
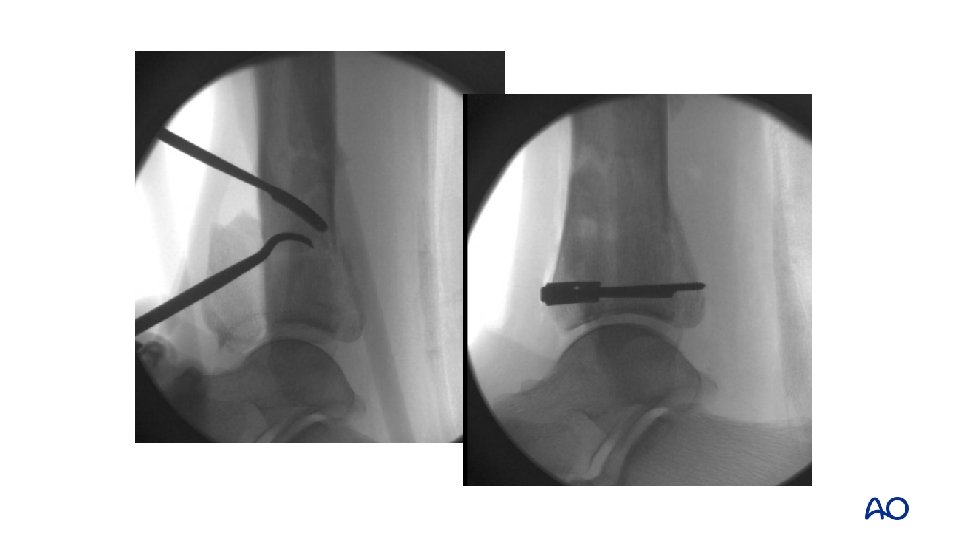
Provisional fixation with K-wires and Weber clamps
• • Lag screw fixation with 2. 4 mm screws Definitive fixation with nonlocking implants after anatomical reduction
Anterior fracture line • • Anterior fracture line lateral to the medial shoulder Anterolateral approach may be suitable
Joint distraction and reduction of posterior fragment
After reduction and provisional fixation, joint fragments are fixed with minifragment plates and screws
Soft-tissue limitation
Varus or valgus? • Varus injuries: medial plate • Valgus injuries: lateral plate • Often both are used in conjunction • Locking plates may give more support for fractures with metadiaphyseal comminution or poor bone quality
Closure
Closure
Postoperative • Well-padded splint • Drains for 48 hours • Early range of motion: ankle and subtalar joints • Nonweight bearing 8– 12 weeks
Take-home messages • Understand the fracture • Choose approach(es) • Direct articular reduction • Soft tissue friendly and effective plate application • (You can and will) avoid complications