COMPLEX REGIONAL PAIN SYNDROME Utkan Aydin MD CMKI





 – CRPS ■ Type")







 2. Continued")













 – 5. 5/100, 000 person/years incidence")


























![Ketamine ■ Psychonautics (from the Greek ψυχή psychē ["soul", "spirit" or "mind"] and ναύτης](https://slidetodoc.com/presentation_image_h/049cd755f98e5d84be36fe49936cb773/image-57.jpg "Ketamine ■ Psychonautics (from the Greek ψυχή psychē [\"soul\", \"spirit\" or \"mind\"] and ναύτης")

 ■ Useful for cold allodynia ■ N‐Acetylcysteine 600 mg three")








- Slides: 67
COMPLEX REGIONAL PAIN SYNDROME Utkan Aydin, MD CMKI Morning Lecture, 11/9/2015
The painful patient ■ Beware of patients being erroneously labeled by physicians ■ Patients can be looking for a disease label to justify their symptoms. ■ They may think it enhances their claim and/or may be seeking the role of sick or injured. They can be manipulating a psychosocial situation. Morton l. Kasdan, ASSH January 2011 Correspondence News
The painful patient ■ Humpty Dumpty sat on a wall, Humpty Dumpty had a great fall. All the king's horses and all the king's men Couldn't put Humpty together again Morton l. Kasdan, ASSH January 2011 Correspondence News
The painful patient ■ Know your patient and evaluate any secondary agenda. ■ Ask ourselves are we really doing this patient help or harm by labeling with RSD (CRPS) without objective bilateral imaging. ■ Evaluate whether we doing the “right thing” - giving the patient a label that is not confirmed with objective findings? ■ Always confirm a diagnosis with clear objective findings. ■ Understand there is nothing wrong with telling a patient you have pain that I cannot explain (Code 729. 5). Morton l. Kasdan, ASSH January 2011 Correspondence News
Terminology ■ Reflex Sympathetic Dystrophy ■ Causalgia ■ Neurodistrophy ■ Shoulder-hand syndrome ■ Sudeck’s atrophy ■ Sympathalgia Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Terminology ■ International Association for the Study of Pain (1994) – CRPS ■ Type I Pain syndrome without identifiable nerve lesion ■ Type II Syndrome with identifiable nerve injury or compression ■ Type III Other syndromes (e. g. fibromyalgia) Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Terminology ■ Type II is a clinical diagnosis – Supported by NCS ■ Type I and Type II can be divided into: – Sympathetically mediated pain – Sympathetically independent pain Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Terminology Pain ■ An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.
Terminology Allodynia Pain due to a stimulus that does not normally provoke pain.
Terminology Causalgia ■ A syndrome of sustained burning pain, allodynia, and hyperpathia after a traumatic nerve lesion, often combined with vasomotor and sudomotor dysfunction and later trophic changes.
Terminology Hyperalgesia ■ Increased pain from a stimulus that normally provokes pain.
Terminology Hyperesthesia ■ Increased sensitivity to stimulation, excluding the special senses.
Terminology Noxious stimulus ■ A stimulus that is damaging or threatens damage to normal tissues.
IASP Diagnosis for CRPS 1. Initiating noxious event (Surgery, fracture etc. ) 2. Continued pain disproportionate to event and beyond a single nerve distribution 3. Edema, skin blood flow abnormality, or abnormal sudomotor activity (e. g. sweating) 4. No other diagnosis Last 3 criteria must be present Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Signs and Symptoms of CRPS ■ Pain starts in one limb but can present in the trunk (spine, abdomen, pelvis) ■ Constant pain, even at rest with intermittent exacerbations. Unexplained and diffuse ■ Severe pain ■ Temperature, color change. ■ Edema ■ Area of pain larger than the primary injury ■ Limited range of motion
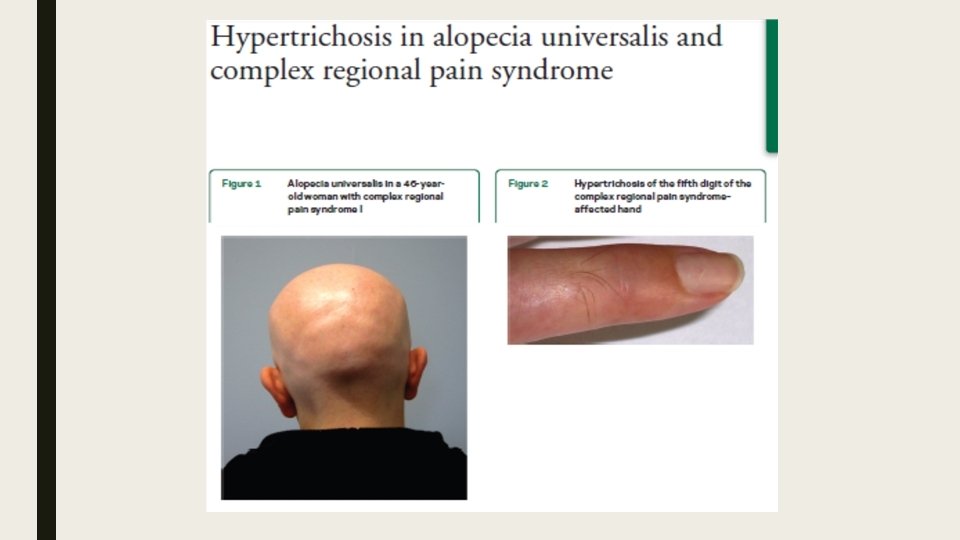
Signs and Symptoms of CRPS ■ Allodynia ‐ pain on light touch ■ Nail growth changes (faster, distorted), hair growth changes (coarser, darker, rapid growth, hair falling), skin changes (atrophy of skin), skin lesions
Muscle symptoms in CRPS ■ Muscle spasms ■ Dystonia ■ Tremors ■ Myoclonus
Best Diagnostic tool ■ A good history and physical examination ■ A repeat examination may be done to come to a diagnosis because of the fleeting nature of some of the symptoms (color change, temperature asymmetry)
Pain physiology 1. Ascending nociceptive signals – Transmitted by Aδ and C afferent fibers – Dorsal horn of spinal cord (modulated) – Spinothalamic tract (cortical modulation) 2. Descending modulation – Periaqueductal gray matter – Nucleus raphe magnus (pons) Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Production of CRPS ■ Cutaneous – Epidermal neurite density – Afferent fiber desity ■ Sensitization of peripheral nerves secondary to excitatory mediators ■ Central sensitization – Spinal neurons ■ Altered symphathetic function – Increased nerve adrenergic receptors – Sympatho-afferent coupling ■ Upregulation of catecholamine receptors (vasoconstriction) ■ Genetic – Somatotopic maps Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
CRPS and Depression ■ CRPS causes suffering and affects mood but is NOT a psychogenic condition – 22 -78% chronic pain patients are depressed ■ Mersky, 1983 – Mood improves with pain resolution ■ Mellick et al. Arch Phys Med Reh 1997 Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Central Sensitization ■ Increase in the excitability of neurons within the central nervous system (CNS) so that normal inputs produce abnormal responses
CRPS Associations ■ Anxiety prior to TKA predictive of CRPS at 1 month ■ Harden et al, Pain 2003 ■ Allergy/Hypersensitivity associated with CRPS in orthopaedic patients – 68% vs 34% in 115 CRPS vs 15 controls ■ Li et al, Orthopedics 2014 ■ Longer duration of anesthesia during limb surgery ■ Sumitani et al, Rheumatology 2013 Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Epidemiology ■ CRPS Type I – incidence: 5. 5 per 100, 000 person-years – prevalence: 21 per 100 K – fractures: ■ prospective studies: 26 -39% ■ retrospective studies: 1 -2 % ? ? ■ CRPS Type II – incidence: 0. 8 per 100, 000 person-years – prevalence: 4 per 100 K – peripheral nerve injury: 1 -5%
Incidence and Demographics ■ Olmsted county, Minnesota (2003) – 5. 5/100, 000 person/years incidence – 20. 7/100. 000 person/years prevalence ■ ■ Median age of onset 46 years Women 4: 1 Upper extremity 2: 1 4 -39% incidence with distal radius fracture Sandroni et al, Pain 2003 Zollinger et al, JBJS 2007 Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Epidemiology ■ CRPS Type I: ~50% work-related – 90% related to Trauma ■ 80% of CRPS type I resolve within 18 months
Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Why Distal Radius Fractures? ■ Increased pressures in the carpal tunnel – 18 mm. Hg (neutral wrist), 27 mm. Hg (20° flexion), 47 mm. Hg (40° flexion) – 2/23 patients ≥ 43 mm. Hg at neutral ■ Gelberman et al, J Trauma 1984 ■ 30/35 cases demonstrated as Type II – 70% CTS, 47% cubital tunnel ■ Monsivais et al JHS (Br) 1993 Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Disease Burden ■ Mean duration of pain: 3 years ■ 30% of patients out of work for ≥ 1 year – Geertzen et al, Acta Orthop Scand Suppl 1998 Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Lankford and Evans - Stages of RSD acute subacute chronic onset exam imaging XR normal 0 -3 mo pain, swelling, warmth, redness, decr ROM, hyperhidrosis 3 -12 mo worse pain, cyanosis, dry skin, stiffness, skin atrophy osteopenia on XR >12 mo diminished pain, fibrosis, glossy skin, joint contractures extreme osteopenia on XR (+) 3 -phase bone scan (incr)
Staging ■ Acute – Aching, burning, hyperemia ■ Dystrophic – Tissue thickening ■ Atrophic – Less pain, cool skin, contracture ■ No clear time-course Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Staging ■ Hot vs Cold ■ Others argue that when pain is gone there is no more CRPS – Compartment syndrome and Volkmann’s Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Recognizing CRPS Patients ■ Anxious, unable to sleep despite narcotics ■ Burning, aching, allodynia ■ Reluctant for physician to touch ■ Temperature changes, swelling, skin color changes ■ Joint contracture Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Differential Diagnosis ■ ■ diabetic, etc ■ ■ Post-traumatic ■ neuralgia ■ ■ anatomically defined territory ■ ■ CNS disorders ■ ■ Neuropathy ■ ■ stroke tumor MS trauma ■ Spinal cord ■ Radiculopathy Plexopathy Nerve entrapment Vasculitis / vascular Psychiatric Toxic Infectious ■ viral ■ fungal ■ Lyme disease ■ Iatrogenic
Work Up ■ Rule out other diagnoses ■ CBC ■ Inflammatory arthropathy / vasculitis: – ESR, CRP – ANA, RF, complement fixation panel ■ DM: glucose, Hgb. A 1 c ■ EMG / NCS ■ vascular studies ■ 3 -phase bone scan (early) ■ Plain XR (late)
Imaging and Diagnostic Testing ■ No single definitive test – Xray: peri-articular demineralization – Triple phase technetium 99 m bone scan ■ Increased periarticular activity in 3 rd phase – Sensitivity (50 -90%), specificity (75 -92%) ■ Thermography after sympathetic block, cold stress test with laser Doppler fluximetry, resting sweat test Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Imaging and Diagnostic Testing ■ Periarticular demineralization following distal radius fracture Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014 www. radiopaedia. com
Sympathetic Mediated? ■ Diagnostic stellate ganglion block or oral sympatholytic challenge – Blocks must produce Horner’s, increased extremity peripheral venous engorgement ■ Influence of sympathetic system in a patient may vary over time Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Treatment ■ Prevention – Avoid tight casts – Protect causalgic nerves – Vitamin C and distal radius fractures Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Vitamin C ■ Antioxidant with capillary protective effect that decreases wall permeability ■ Zollinger, et al JBJS 2007 – Randomized, double blind placebo controlled w/416 patients after wrist fracture ■ Vitamin C doses: 200, 500, 1500 mg – 2. 4% vs 10. 1% CRPS in placebo – Recommend 500 mg for 50 days following distal radius fracture Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Vitamin C ■ Besse, et al F&A Surg, 2009 – 2 groups (total 420 patiens) w/ and w/o Vit C ■ 1 gram post op daily for 45 days ■ 1. 7% incidence vs 9. 6 incidence CRPS ■ Is Vitamin C totally safe? Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Vitamin C use: Jaiman A, Lokesh M, Neogi DS. , 2011 ■ A dose of 1000 mg for 45 days is nearly 10 times the recommended daily dosage of 90– 100 mg ■ Levine et al. studied the relationship between vitamin C doses and steady-state concentrations in healthy young women ■ At doses of 200 mg daily and higher, there was little change in plasma concentrations, with saturation between 200 and 400 mg daily. ■ Circulating neutrophils, monocytes, and lymphocytes contained 0. 5 – 4. 0 m. M concentrations of vitamin C and also saturated between 200 and 400 mg daily
Vitamin C use ■ In a study by Taylor and Curhan, participants consuming 1000 mg/day or more of vitamin C excreted 6. 8 mg/day more urinary oxalate than participants consuming <90 mg/day (P trend < 0. 001) ■ Multivariate relative risk of kidney stone formation for men consuming 1000 mg or greater of vitamin C per day was 41% higher than those consuming less than the recommended dietary allowance of 90 mg/day.
Vitamin C use: Besse JL. 2012 ■ Our study used a 1000 mg Vitamin C protocol for Foot and Ankle surgery, it is logical for us to recommend this dose. ■ For six years, our orthopaedic and traumatologic department has used this protocol for all operations. We can estimate that more than 10, 000 patients received this 1000 mg Vitamin C prevention and we never observed any adverse effects. We only checked history of (uric acid) kidney stone. ■ However I agree that in light of the last Zollinger publication [4], 500 mg of Vitamin C is probably enough.
Treatment ■ As a hand surgeon the greatest impact is to: 1. Make the diagnosis 2. Distinguish type II disease and decompress involved nerves Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Treatment ■ Ideally incorporates a multidisciplinary team: – Hand surgeon – Primary medical providers – Pain specialists – Therapists – Psychologists – Social workers Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Treatment 1. OT and PT – Minimize pain and edema – Maximize comfortable mobility 2. Nerve stimulation (PNS/CNS) – Gate theory ■ Geurts et al, Neuromodulation 2013 3. Nerve blocks (esp. sympathetics) 4. Medication (None FDA approved) – Antidepressants, anticonvulsants, antiadrenergic, steroids, bisphosponates Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Treatment Options ■ Corticosteroids ■ CCBs ■ Calcium-reg drugs ■ Beta blockers ■ Opioids ■ Oral sympatholytics ■ NSAIDs ■ Clonidine ■ TCAs / SSRIs ■ Sympathetic blocks ■ Sodium channel blockers ■ Ketamine ■ GABA agonists ■ Gabapentin ■ Spinal cord stimulator ■ PT/OT ■ Psych
Treatment ■ Bisphophonates – Class of drugs used to treat bone loss. ■ Calcium regulating drugs – in refractory cases ■ Clodronate (300 mg) daily IV for 10 days – pain, swelling, movement range in acute CRPS ■ Alendronate (7. 5 mg) once IV ‐ pain, swelling, movement range in acute CRPS ■ Pamidronate 60 mg IV Forouzanfar T, Koke AJ, Kleef M van, Weber WE. Treatment of complex regional pain syndrome type I. Eur J Pain 2002; 6(2): 105‐ 22. Adami S, Fossaluzza V, Gatti D, Fracassi E, Braga V. Bisphonate therapy of reflex sympathetic dystrophy syndrome. Ann Rheum Dis 1997; 56(3): 201‐ 4.
Treatment ■ Ketamine – CRPS ‐ activation and proliferation NMDA of receptors – Strong NMDA Receptor blocker – One of the safest anesthetic drugs – Powerful analgesic even at low doses – Poor absorption when administered orally. – Effective as IV or submucosal (Troche)
Ketamine
Ketamine ■ Psychonautics (from the Greek ψυχή psychē ["soul", "spirit" or "mind"] and ναύτης naútēs ["sailor" or "navigator"] — "a sailor of the soul") refers both to a methodology for describing and explaining the subjective effects of altered states of consciousness, including those induced by meditation or mind-altering substances.
Low dose Ketamine in CRPS ■ Administered in sub‐anesthetic doses –blocks NMDA receptors without causing too many side effects ■ In CRPS it decreases Central Sensitization ■ Administration: IV, sublingual, nasal ■ Rough estimates – 85% show improvement in daily activities, reduction in their medications and improved lifestyles ■ It is not a cure. It is to be done along with otherapies
N‐ Acetyl Cysteine (NAC) ■ Useful for cold allodynia ■ N‐Acetylcysteine 600 mg three times a day for three months Perez RS, Zuurmond WW, Bezemer PD, Kuik DJ, Loenen AC van, Lange JJ de, et al. The treatment of complex regional pain syndrome type. I with free radical scavengers: a randomized controlled study. Pain 2003; 102(3): 297‐ 307
Opioids ■ Repeated exposure to opioids leads to enhanced pro‐inflammatory cytokine release from glia ■ Taking long term opioids for CRPS is not a good idea. ■ Maybe okay to take it for a short term to get over a flare up
acute subacute chronic opiods; NSAIDs Pain Mgmt? opiods; NSAIDs Pain Mgmt referral NSAIDs amitriptyline 75 mg QHS neurontin 900 2400 mg/d < 6 months: pulsed prednisone Medrol dosepak - *** early PT/OT *** intranasal calcitonin (or bisphonate? ) - lidocaine patch? clonidine gel? (PO if HTN) trial: sympathethectomy (chemical surgical? ) - ketamine infusion psychologic / cognitive therapy DR: Vit. C 500 mg/d x 50 d - spinal cord stimulator?
Outcomes ■ Good outcomes in 94% of 105 patients when treating within 4 months of symptoms – No permanent CNS changes ■ 50% of those untreated for 12 months will have permanent impairment ■ Digit contracture at 3 months correlates with 10 year CRPS morbidity following distal radius fracture Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Outcomes Nerve Decompression for Type II ■ Placzek, et al JHS 2005 – 8 patients at 13 weeks after index procedure – Resolved hypersensitivity, swelling – Improved DASH (71 to 30), VAS (7. 5 to 1. 8) ■ Grundberg and Regan, JHS 1991 – 26/29 patients improved swelling, PIP motion (35 to 76°) and strength Ryan P. Calfee, MD, MSc, Comprehensive Review Course, 2014
Surgery after CRPS ■ Perioperative stellate ganglion block may reduce recurrence – Recurrence 10% vs 72% in 100 patients ■ Reuben et al, 2000
Summary ■ CRPS is likely the end result of a complex interaction of multiple inter-related nervous system changes ■ CRPS leads to marked and prolonged morbidity ■ Vitamin C is effective for prevention of CRPS associated with distal radius fracture
Summary ■ Early treatment of CRPS optimizes outcomes ■ Type II CRPS should be treated with nerve decompression
Thank you !