Compartment syndrome elevation of the interstitial pressure in


 • Fractures • Soft tissue trauma •")


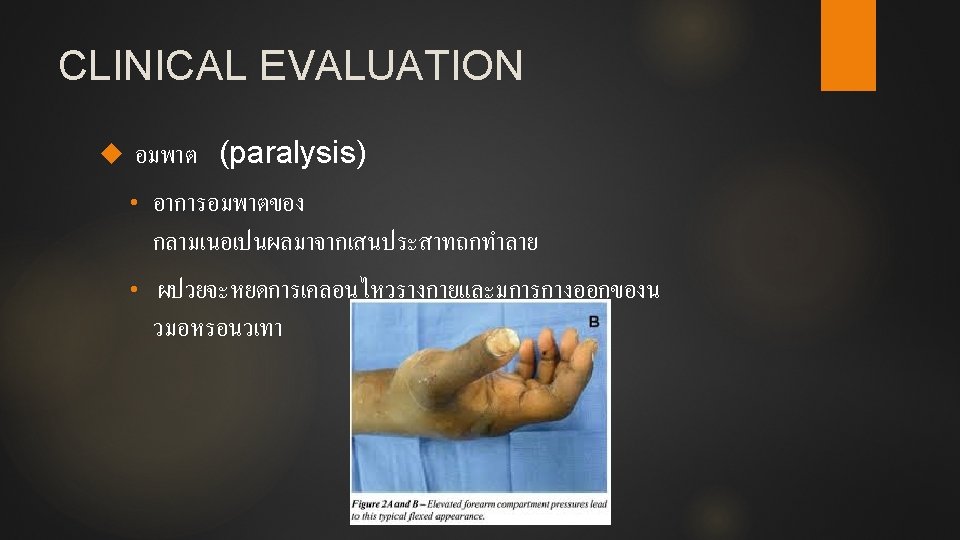
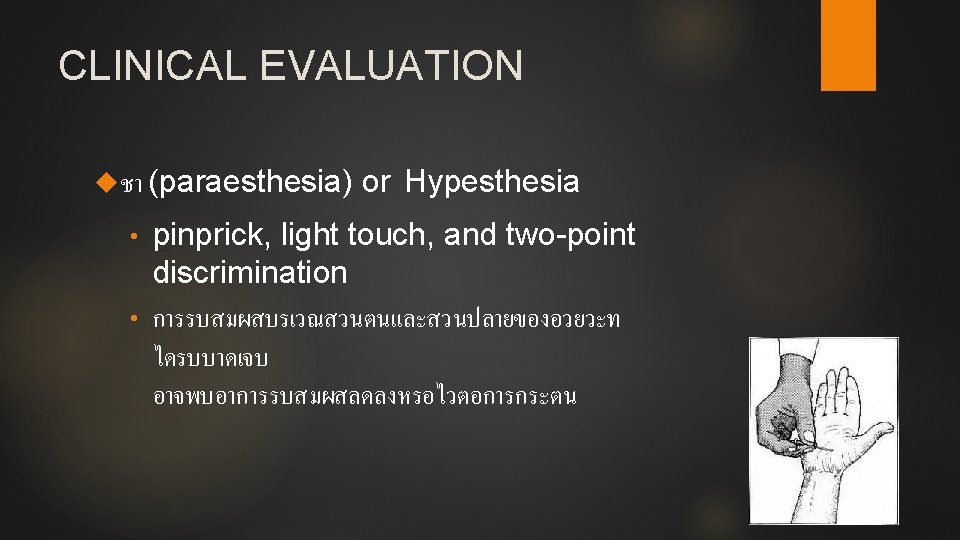
 • อมพาต (paralysis) • ชา (paraesthesia) •")














- Slides: 37
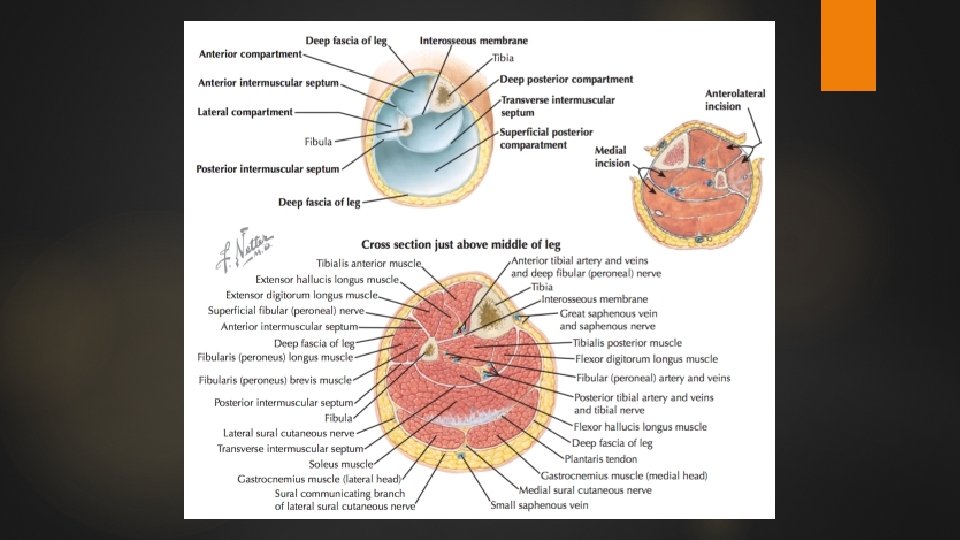
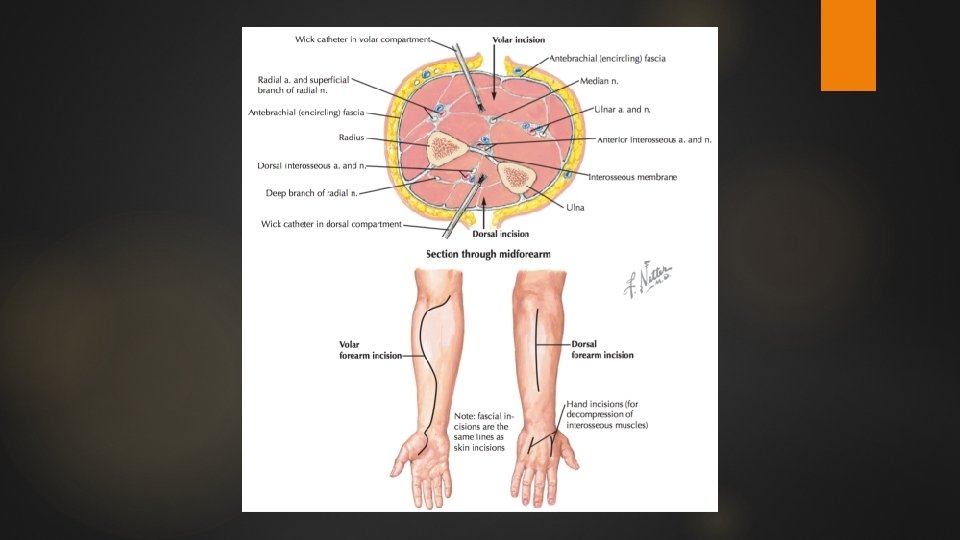
Compartment syndrome ภาวะทความดนภายในชองปดเพมสงขนมากจนกระทงรบกว นตอระบบ ไหลเวยนเลอด และการทางานของเนอเยอออนภายในชองนนๆ (elevation of the interstitial pressure in a closed osteofascial compartment that results in microvascular compromise) สวนใหญพบท Anterior and deep posterior compartments of the leg Volar compartment of the forearm
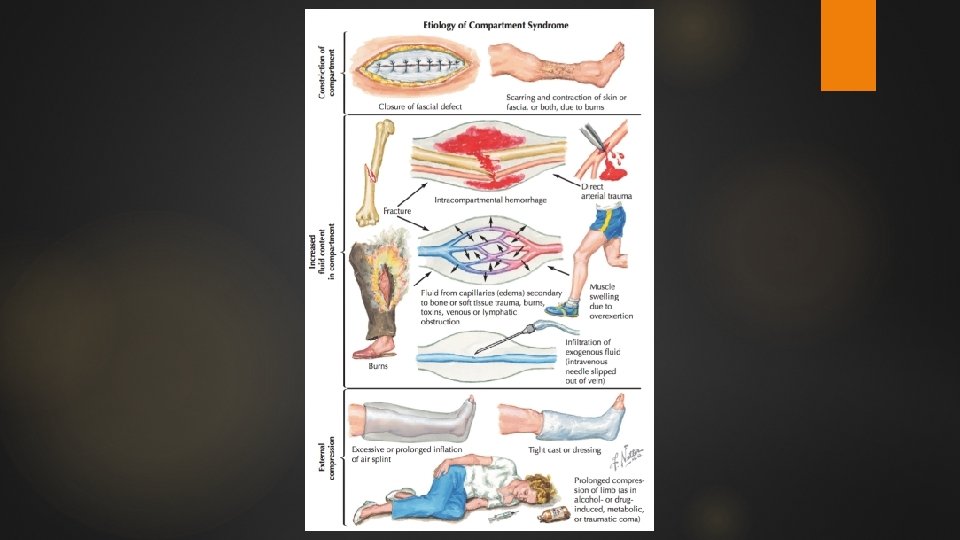
สาเหตของ compartment syndrome สาเหตสวนใหญ (most common causes) • Fractures • Soft tissue trauma • Arterial injury • Limb compression during altered consciousness • Burns
PATHOPHYSIOLOGY
PATHOPHYSIOLOGY Significant muscle necrosis can occur in patients with normal blood flow if intracompartmental pressure is increased to more than 30 mm. Hg for longer than 8 hours. Higher pressures have been shown to cause greater compromise of neuromuscular viability in shorter periods of time.
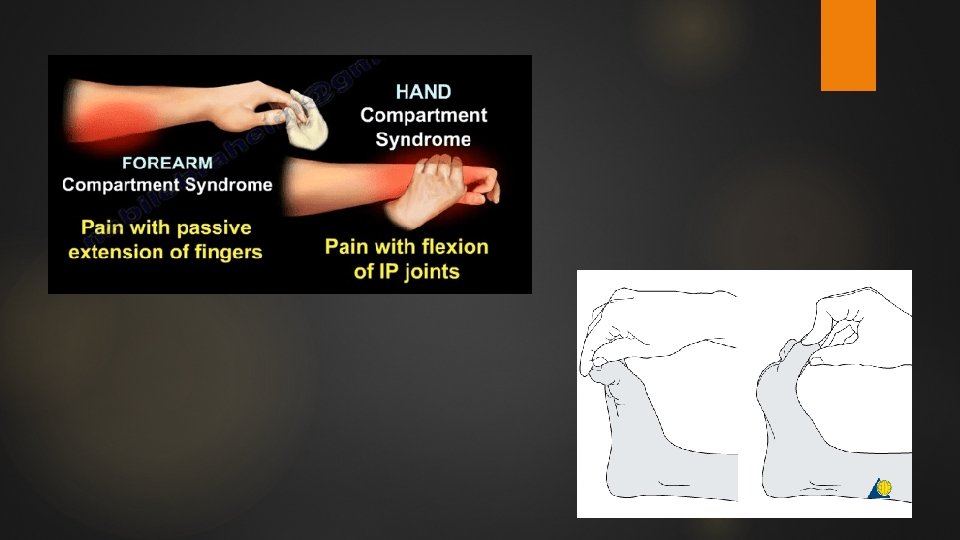
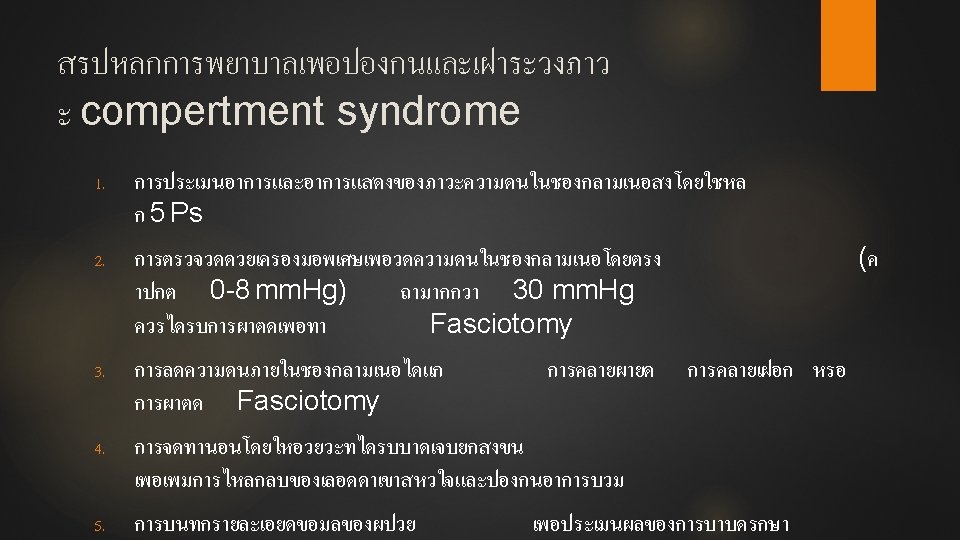
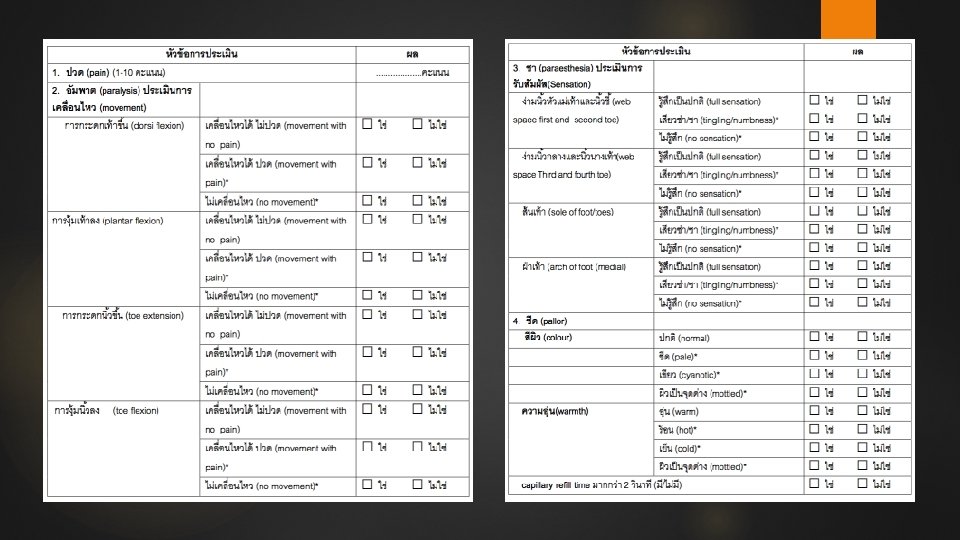
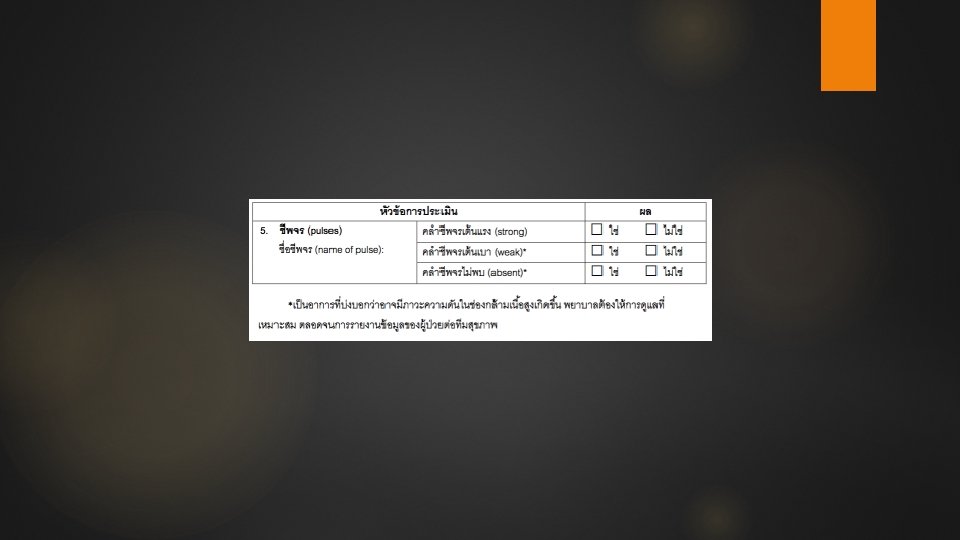
CLINICAL EVALUATION 5 Ps • ปวด (pain) • อมพาต (paralysis) • ชา (paraesthesia) • ชพจร (pulses and/or capillary refill) • ซด (pallor)และอณหภม (temperature)
CLINICAL EVALUATION Absence of clinical findings associated with compartment syndrome is more useful for excluding the diagnosis than the presence of findings is for confirming the diagnosis.
Investigation If compartment syndrome is suspected an adequate examination cannot be performed, pressure levels should be measured
Investigation Noninvasive methods • Ultrasonography measure submicrometer displacement of the fascia wall caused by volume expansion of the muscle compartment (sensitivity 77% , specificity 93%) • Infrared imaging determine temperature diferences between the proximal and distal skin surfaces to help make the diagnosis of compartment syndrome
Investigation Invasive methods • Commercially available pressure monitor • Arterial line manometer • Whitesides three-way stopcock apparatus • Wick monitor
Commercially available pressure monitor
Arterial line manometer
Whitesides three-way stopcock apparatus
Wick monitor
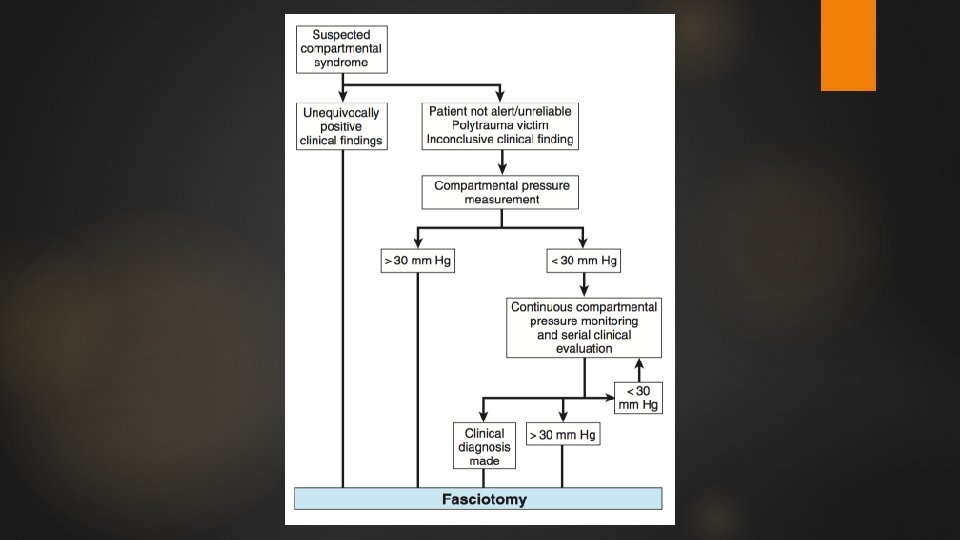
TREATMENT Compartmental pressures are greater than 30 mm Hg in the presence of clinical findings, immediate fasciotomy is indicated In patients with major disruption of the arterial circulation or circumferential full- thickness burns, fasciotomy should be performed at the time of initial surgery
Fasciotomy
Fasciotomy
Fasciotomy
Thank You