INTERSTITIAL LUNG DISEASE Dr Ghassan Kawar What is









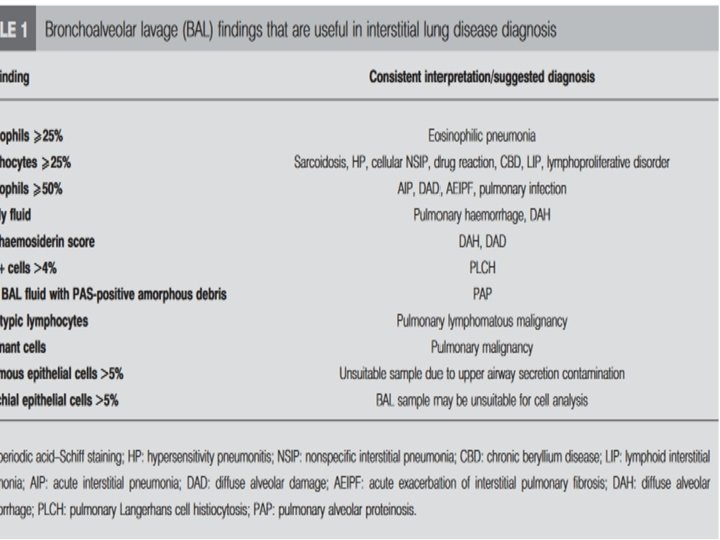
 Eosinophilia (CEP) Autoimmune serologies HP")





- Slides: 37
INTERSTITIAL LUNG DISEASE Dr Ghassan Kawar
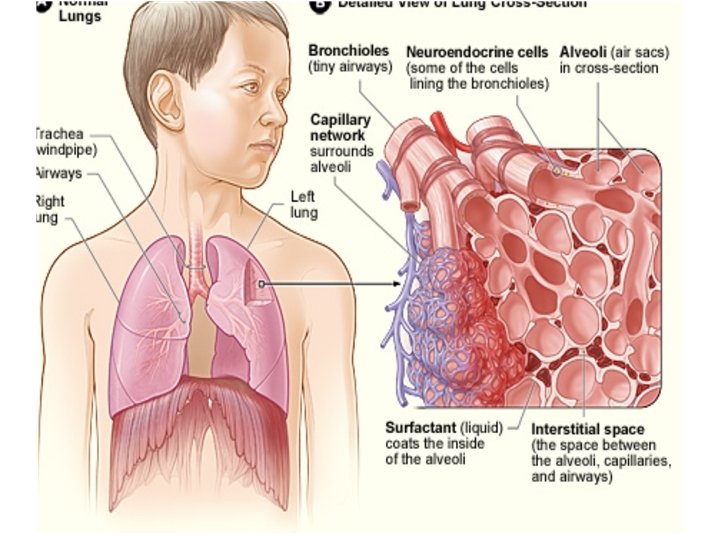
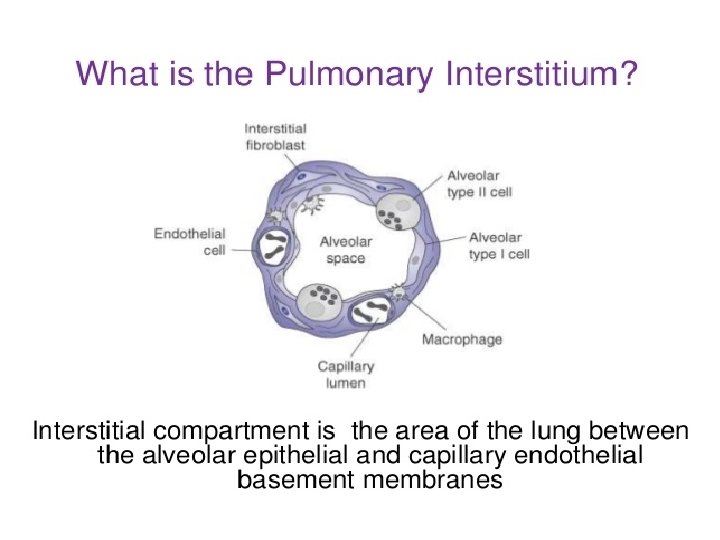
What is the pulmonary interstitium? • Anatomic space that is lined by epithelial and endothelial cells • Contains collagen, elastin, reticulin, ECM • Also in the connective tissue of the lung (interlobular septa, visceral pleura, peribronchovascular sheaths)
Epidemiology
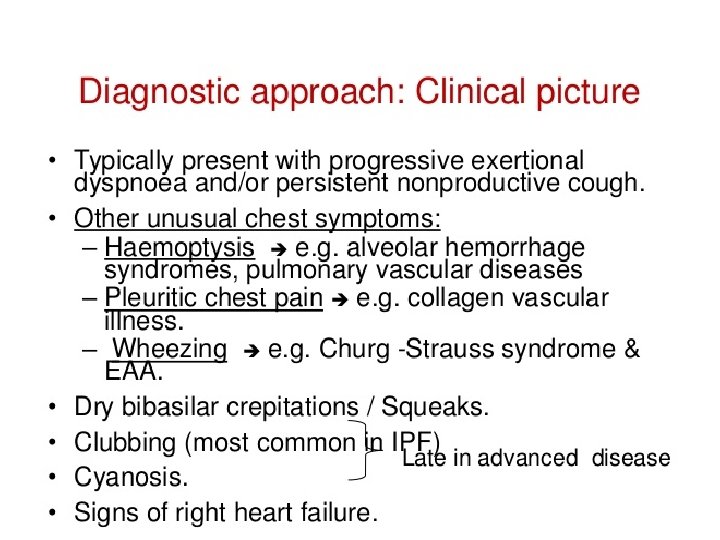
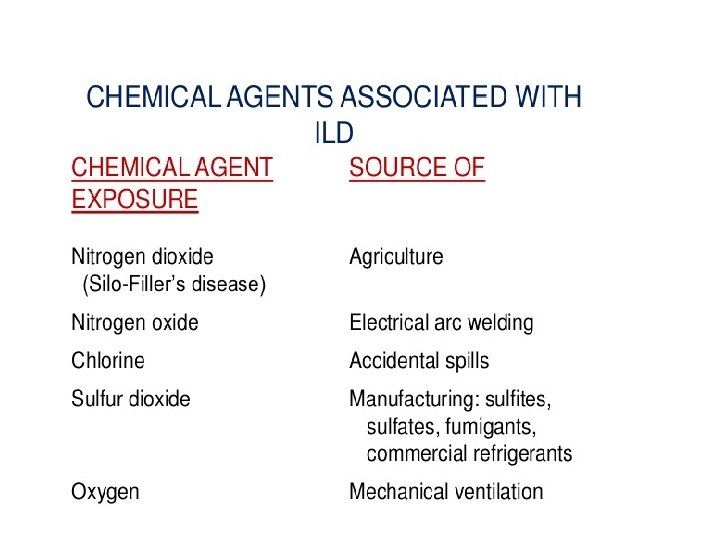
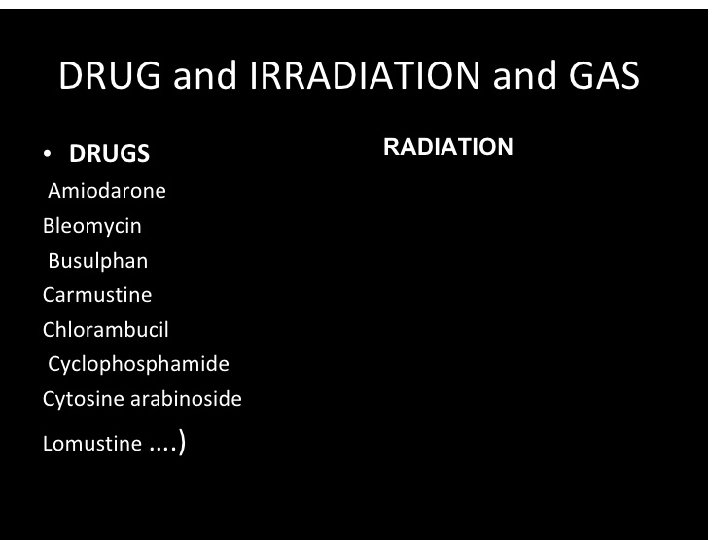
Clinical Evaluation: History • • • • Demographics Age: IPF>50 years, 20‐ 40: CTD, sarcoid, LAM, LCH, familial Female: LAM, CTD‐ILD, Men: RA‐ILD, occupational Onset of Symptoms Timing can guide the differential (acute: COP, CTD‐ILD, chronic: IPF, sarcoid) Smoking History LCH, DIP, RB‐ILD, IPF Family History Premature graying, history of ILD Review of Systems Arthralgias, Raynaud’s, Myositis, Dysphagia/Reflux Drugs Occupational/Environmental Exposures Don’t forget OTC and illicit Birds/Mold Asbestos, Silica
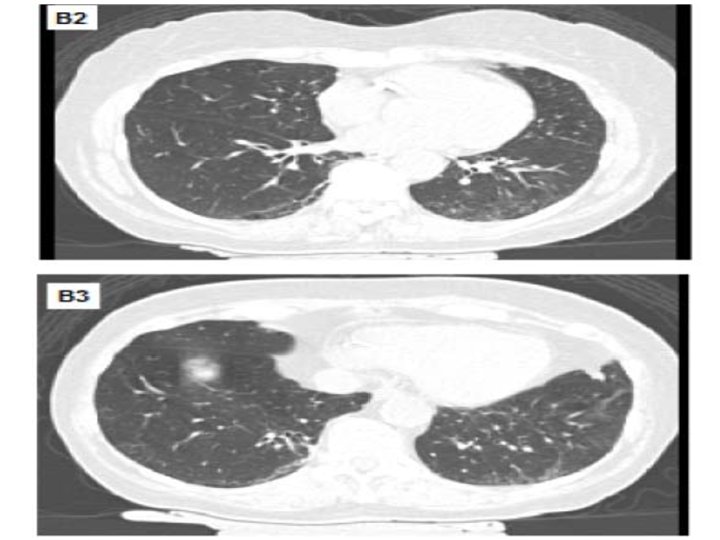
Diagnostic Tests • Imaging • Pulmonary Function Tests • Laboratory • Bronchoscopy • Surgical lung biopsy
Interstitial Lung Abnormalities • Increased lung density on CT scans in patients with no history of ILD • 2‐ 10% of the population • Association with reduction in PFT, exercise capacity, development of ILD, and mortality • Refer to pulmonary
Pulmonary Function Test • • • Spirometry Predicted Observed FVC 3. 72 2. 24 FEV 1 3. 06 1. 78 FEV 1/FVC 82 79 Plethysmography TLC 5. 26 3. 38 Diffusion Diffusing Capacity 29. 01 8. 01 %Pred 60% 58% 96% 64% 28%
Clinical Evaluation: Laboratory Analysis CBC with differential Macrocytosis (telomeropathy) Eosinophilia (CEP) Autoimmune serologies HP precipitans Poor sensitivity and specificity, limited range of antigens tested Genetic testing Selected cases (e. g. BHD), emerging for FPF • Telomere length measurement Emerging • VEGF‐D Lymphangioleiomyomatosis • • •
IPF: Why is diagnosis important? • Median survival ~4 years • Acute exacerbation rate 5‐ 10% per year
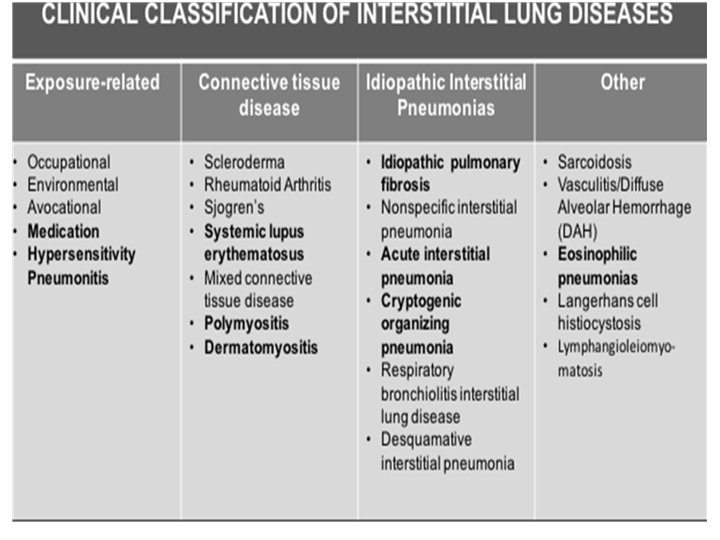
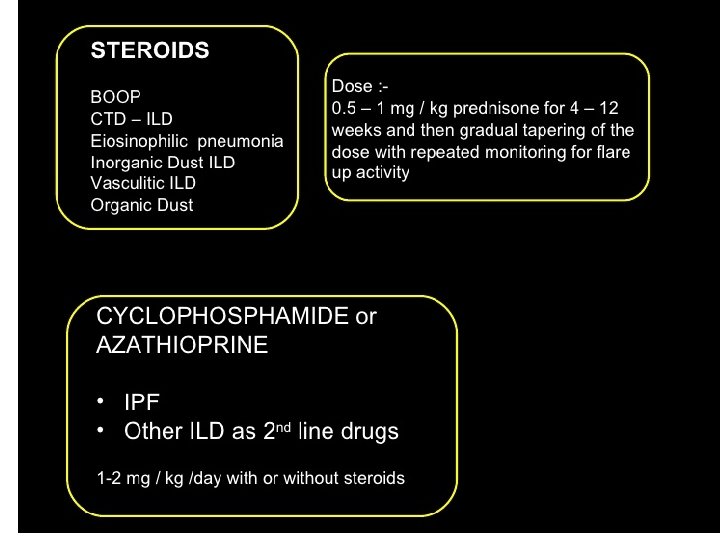
Hypersensitivity Pneumonitis • No consensus diagnostic criteria – Classic imaging + good exposure – Lung biopsy • Described as acute, sub‐acute, and chronic • Over 200 exposures identified: – Typically related to mold or bird products • Treatment – Remove exposure – Prednisone +/‐ mycophenolate or azathioprine
Connective Tissue Disease • CTD • Systemic Sclerosis Rheumatoid Arthritis Diagnosis Esophageal Dilation Consider drug induced lung injury for new/worsening ILD • Dermatomyositis/Polymyositis Myositis may be subtle ILD can come first ANA can be negative • Sjogren’s Syndrome Cysts on HRCT • Lupus ILD is unsual
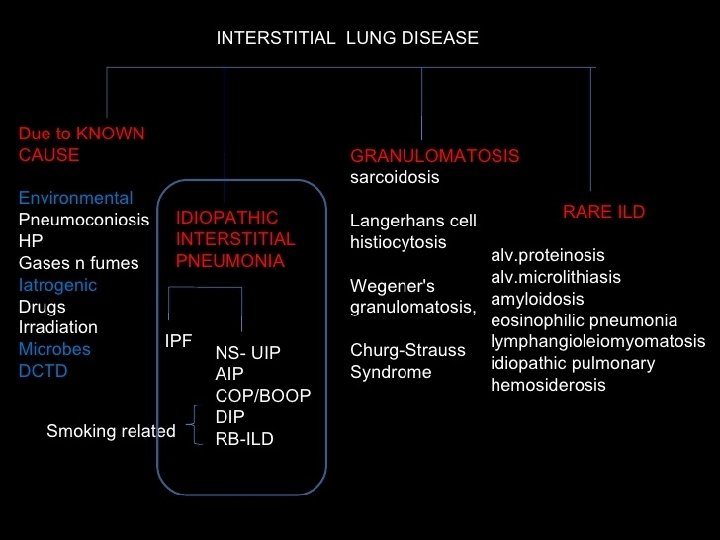
Conclusions • Multiple types of ILD • Consider in older patient with cough or subacute shortness of breath • Evaluation starts with high resolution CT, may need surgical lung biopsy • Important to distinguish IPF from other types of ILD as treatment differs