Management of Patient Requiring Breathing Assistance Topic 2
 Dr. S.")
Management of Patient Requiring Breathing Assistance Topic 2 (Q and A session) Dr. S. Nishan Silva (MBBS)

Q : Parts of the Respiratory System?

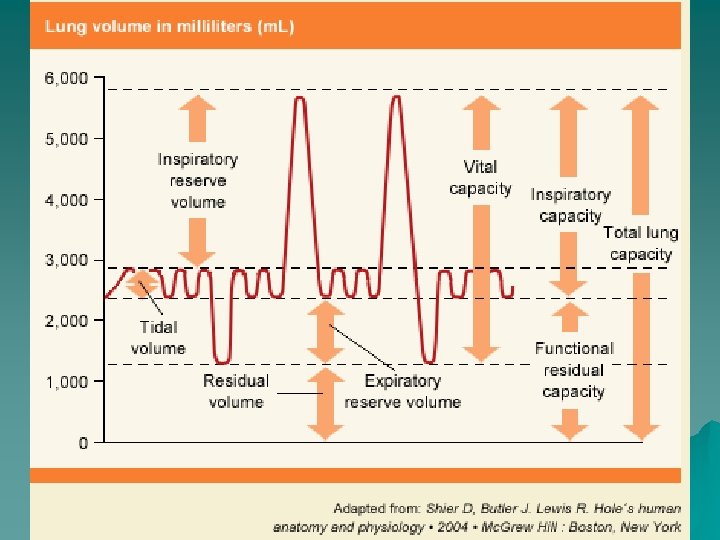
Q : Explain the different “Lung volumes”

Q : Indications for Ventilation?

Initiation of Mechanical Ventilation u Indications – Indications for Ventilatory Support – Acute Respiratory Failure – Prophylactic Ventilatory Support – Hyperventilation Therapy
 u Respiratory activity")
Initiation of Mechanical Ventilation u Indications – Acute Respiratory Failure (ARF) u Respiratory activity is inadequate or is insufficient to maintain adequate oxygen uptake and carbon dioxide clearance. u Inability of a patient to maintain arterial Pa. O 2, Pa. CO 2, and p. H acceptable levels u Pa. O 2 < 70 on on O 2 u Pa. CO 2 > 55 mm Hg and rising u p. H 7. 25 and lower
 u Hypoxic lung")
Initiation of Mechanical Ventilation Indications u – Acute Respiratory Failure (ARF) u Hypoxic lung failure (Type I) – – – Ventilation/perfusion mismatch Diffusion defect Right-to-left shunt Alveolar hypoventilation Decreased inspired oxygen – Acute life-threatening or vital organ -threatening tissue hypoxia
 u Clinical Presentation")
Initiation of Mechanical Ventilation u Indications – Acute Respiratory Failure (ARF) u Clinical Presentation of Severe Hypoxemia – Tachypnea – Dyspnea – Central cyanosis – Tachycardia – Hypertension – Irritability, confusion – Loss of consciousness – Coma
 u Acute Hypercapnic")
Initiation of Mechanical Ventilation Indications u – Acute Respiratory Failure (ARF) u Acute Hypercapnic Respiratory Failure (Type II) – CNS Disorders u Reduced Drive To Breathe: depressant drugs, brain or brainstem lesions (stroke, trauma, tumors), hypothyroidism u Increased Drive to Breathe: increased metabolic rate ( CO 2 production), metabolic acidosis, anxiety associated with dyspnea
 u Acute Hypercapnic")
Initiation of Mechanical Ventilation Indications u – Acute Respiratory Failure (ARF) u Acute Hypercapnic Respiratory Failure (Type II) – Neuromuscular Disorders u Paralytic Disorders: Myasthenia Gravis, Guillain-Barre´, ALS, poliomyelitis, etc. u Paralytic Drugs: Curare, nerve gas, succinylcholine, insecticides u Drugs that affect neuromuscular transmission; calcium channel blockers, long-term adenocorticosteroids, etc. u Impaired Muscle Function: electrolyte imbalance, malnutrition, chronic pulmonary disease, etc.
 u Acute Hypercapnic")
Initiation of Mechanical Ventilation Indications u – Acute Respiratory Failure (ARF) u Acute Hypercapnic Respiratory Failure – Increased Work of Breathing u Pleural Occupying Lesions: pleural effusions, hemothorax, empyema, pneumothorax u Chest Wall Deformities: flail chest, kyphoscoliosis, obesity u Increased Airway Resistance: secretions, mucosal edema, bronchoconstriction, foreign body u Lung Tissue Involvement: interstitial pulmonary fibrotic diseases
 u Acute Hypercapnic")
Initiation of Mechanical Ventilation Indications u – Acute Respiratory Failure (ARF) u Acute Hypercapnic Respiratory Failure – Increased Work of Breathing (cont. ) u Lung Tissue Involvement: interstitial pulmonary fibrotic diseases, aspiration, ARDS, cardiogenic PE, drug induced PE u Pulmonary Vascular Problems: pulmonary thromboembolism, pulmonary vascular damage u Dynamic Hyperinflation (air trapping) u Postoperative Pulmonary Complications
 u Clinical Presentation")
Initiation of Mechanical Ventilation u Indications – Acute Respiratory Failure (ARF) u Clinical Presentation of Hypercapnia – Tachypnea – Dyspnea – Tachycardia – Hypertension – Headache (hallucinations when severe) – Confusion (loss of consciousness, even coma when severe) – Sweating

Initiation of Mechanical Ventilation u Prophylactic Ventilatory Support – Clinical conditions in which there is a high risk of future respiratory failure u Examples: Brain injury, heart muscle injury, major surgery, prolonged shock, smoke injury u Ventilatory support is instituted to: – Decrease the WOB – Minimize O 2 consumption and hypoxemia – Reduce cardiopulmonary stress – Control airway with sedation

Initiation of Mechanical Ventilation u Hyperventilation Therapy – Ventilatory support is instituted to control and manipulate Pa. CO 2 to lower than normal levels u Acute head injury


Initiation of Mechanical Ventilation u Contraindications – Untreated pneumothorax u Relative Contraindications – Patient’s informed consent – Medical futility – Reduction or termination of patient pain and suffering

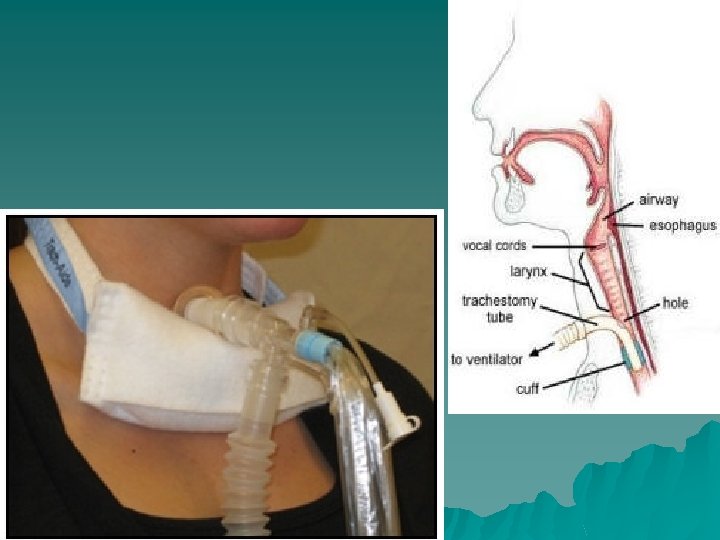
Nomenclature
 – Positive End Expiratory Pressure")
Nomenclature u Airway Pressures – Peak Inspiratory Pressure (PIP) – Positive End Expiratory Pressure (PEEP) – Pressure above PEEP (PAP or ΔP) – Mean airway pressure (MAP) – Continuous Positive Airway Pressure (CPAP) u Inspiratory Time or I: E ratio u Tidal Volume: amount of gas delivered with each breath

Modes u Control Modes: – every breath is fully supported by the ventilator – in classic control modes, patients were unable to breathe except at the controlled set rate – in newer control modes, machines may act in assist-control, with a minimum set rate and all triggered breaths above that rate also fully supported.

Modes u IMV Modes: intermittent mandatory ventilation modes - breaths “above” set rate not supported u SIMV: vent synchronizes IMV “breath” with patient’s effort u Pressure Support: vent supplies pressure support but no set rate; pressure support can be fixed or variable (volume support, volume assured support, etc)
 u. PRVC: Pressure Regulated Volume Control u. PEEP: Positive End")
Ventilator Settings Terminology (con’t) u. PRVC: Pressure Regulated Volume Control u. PEEP: Positive End Expiratory Pressure u. CPAP: Continuous Positive Airway Pressure u. PSV: Pressure Support Ventilation u. NIPPV: Non-Invasive Positive Pressure Ventilation

Modes Whenever a breath is supported by the ventilator, regardless of the mode, the limit of the support is determined by a preset pressure OR volume. – Volume Limited: preset tidal volume – Pressure Limited: preset PIP or PAP

Modes of Ventilation: The Basics u. Assist-Control Ventilation Volume Control u. Assist-Control Ventilation Pressure Control u. Pressure Support Ventilation u. Synchronized Intermittent Mandatory Ventilation Volume Control u. Synchronized Intermittent Mandatory Ventilation Pressure Control

CMV

Control Mode
 or")
Assist Control Ventilation u. A set tidal volume (if set to volume control) or a set pressure and time (if set to pressure control) is delivered at a minimum rate u. Additional ventilator breaths are given if triggered by the patient

A/CV

A/C cont. Negative deflection, triggering assisted breath

Synchronized Intermittent Mandatory Ventilation u Breaths are given at a set minimal rate, however if the patient chooses to breath over the set rate no additional support is given u One advantage of SIMV is that it allows patients to assume a portion of their ventilatory drive u SIMV is usually associated with greater work of breathing than AC ventilation and therefore is less frequently used as the initial ventilator mode u Like AC, SIMV can deliver set tidal volumes (volume control) or a set pressure and time (pressure control)

SIMV

SIMV cont. Machine Breaths Spontaneous Breaths
 Spontaneous inspiratory efforts trigger the ventilator to provide a variable flow")
PSV(pressure support ventilation) Spontaneous inspiratory efforts trigger the ventilator to provide a variable flow of gas in order to attain a preset airway pressure. Can be used in adjunct with SIMV.

Pressure Support Ventilation u The patient controls the respiratory rate and exerts a major influence on the duration of inspiration, inspiratory flow rate and tidal volume u The model provides pressure support to overcome the increased work of breathing imposed by the disease process, the endotracheal tube, the inspiratory valves and other mechanical aspects of ventilatory support.

Tidal Volume or Pressure setting u Maximum volume/pressure to achieve good ventilation and oxygenation without producing alveolar overdistention u Max cc/kg? = 10 cc/kg u Some clinical exceptions

Flow Rate u. The peak flow rate is the maximum flow delivered by the ventilator during inspiration. Peak flow rates of 60 L per minute may be sufficient, although higher rates are frequently necessary. An insufficient peak flow rate is characterized by dyspnea, spuriously low peak inspiratory pressures, and scalloping of the inspiratory pressure tracing

Inspiratory flow u Varies with the Vt, I: E and RR u Normally u Can about 60 l/min be majored to 100 - 120 l/min
 u During spontaneous breathing, the normal")
Inspiratory Time: Expiratory Time Relationship (I: E Ratio) u During spontaneous breathing, the normal I: E ratio is 1: 2, indicating that for normal patients the exhalation time is about twice as long as inhalation time. u If exhalation time is too short “breath stacking” occurs resulting in an increase in end-expiratory pressure also called auto. PEEP. u Depending on the disease process, such as in ARDS, the I: E ratio can be changed to improve ventilation

I: E Ratio u 1: 2 u Prolonged u Inverse at 1: 3, 1: 4, … ratio

Fraction of Inspired Oxygen u. The lowest possible fraction of inspired oxygen (Fi. O 2) necessary to meet oxygenation goals should be used. This will decrease the likelihood that adverse consequences of supplemental oxygen will develop, such as absorption atelectasis, accentuation of hypercapnia, airway injury, and parenchymal injury

FIO 2 u The usual goal is to use the minimum Fio 2 required to have a Pa. O 2 > 60 mmhg or a sat >90% u Start at 100% u Oxygen >40% toxicity normally with Fio 2

Inspiratory Trigger u Normally u 2 set automatically modes: – Airway pressure – Flow triggering
 What is PEEP? What is the goal of PEEP? –")
Positive End-expiratory Pressure (PEEP) What is PEEP? What is the goal of PEEP? – Improve oxygenation – Diminish the work of breathing – Different potential effects
 u. Applied PEEP is generally added to mitigate end-expiratory alveolar")
Positive End-Expiratory Pressure (PEEP) u. Applied PEEP is generally added to mitigate end-expiratory alveolar collapse. A typical initial applied PEEP is 5 cm. H 2 O. However, up to 20 cm. H 2 O may be used in patients undergoing low tidal volume ventilation for acute respiratory distress syndrome (ARDS)

PEEP u What are the secondary effects of PEEP? – Barotrauma – Diminish cardiac output – Regional hypoperfusion – Na. Cl retention – Augmentation of I. C. P. ? – Paradoxal hypoxemia

PEEP u Contraindication: – No absolute CI – Barotrauma – Airway trauma – Hemodynamic instability – I. C. P. ? – Bronchospasm?

PEEP u What PEEP do you want? – Usually, 5 -10 cm. H 2 O

PEEP cont. Pressure above zero PEEP is the amount of pressure remaining in the lung at the END of the expiratory phase.
: • This IS a mode and simply means that")
Continuous Positive Airway Pressure (CPAP): • This IS a mode and simply means that a preset pressure is present in the circuit and lungs throughout both the inspiratory and expiratory phases of the breath. • CPAP serves to keep alveoli from collapsing, resulting in better oxygenation and less WOB. • The CPAP mode is very commonly used as a mode to evaluate the patients readiness for extubation.
 Reduced work of breathing compared")
Advantages of Each Mode Advantages Assist Control Ventilation (AC) Reduced work of breathing compared to spontaneous breathing AC Volume Ventilation Guarantees delivery of set tidal volume AC Pressure Control Ventilation Allows limitation of peak inspiratory pressures Pressure Support Ventilation (PSV) Patient comfort, improved patient ventilator interaction Synchronized Intermittent Mandatory Ventilation (SIMV) Less interference with normal cardiovascular function
 Potential adverse hemodynamic effects, may")
Disadvantages of Each Mode Disadvantages Assist Control Ventilation (AC) Potential adverse hemodynamic effects, may lead to inappropriate hyperventilation AC Volume Ventilation May lead to excessive inspiratory pressures AC Pressure Control Ventilation Potential hyper- or hypoventilation with lung resistance/compliance changes Pressure Support Ventilation (PSV) Apnea alarm is only back-up, variable patient tolerance Synchronized Intermittent Mandatory Ventilation (SIMV) Increased work of breathing compared to AC

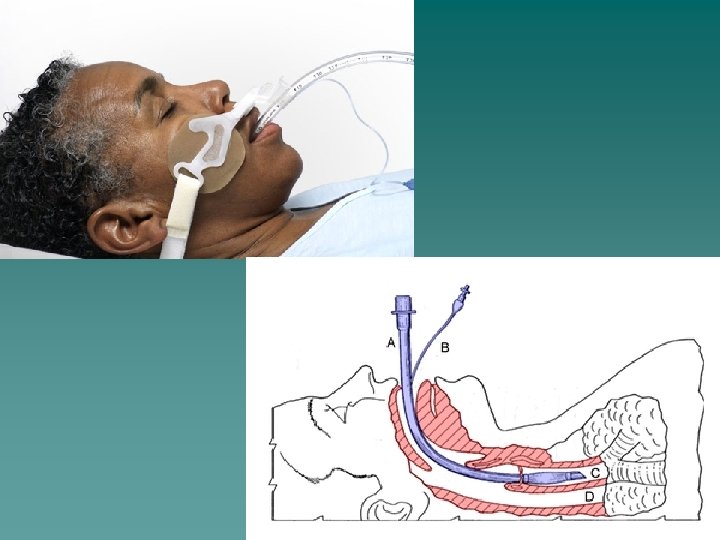
Intubation

Intubation Procedure Check and Assemble Equipment: üOxygen flowmeter and O 2 tubing üSuction apparatus and tubing üSuction catheter or yankauer üAmbu bag and mask üLaryngoscope with assorted blades ü 3 sizes of ET tubes üStylet üStethoscope üTape üSyringe üMagill forceps üTowels for positioning

Intubation Procedure Position your patient into the sniffing position

Intubation Procedure Preoxygenate with 100% oxygen to provide apneic or distressed patient with reserve while attempting to intubate. Do not allow more than 30 seconds to any intubation attempt. If intubation is unsuccessful, ventilate with 100% oxygen for 3 -5 minutes before a reattempt.

Intubation Procedure Insert Laryngoscope

Intubation Procedure

Intubation Procedure After displacing the epiglottis insert the ETT. The depth of the tube for a male patient on average is 21 -23 cm at teeth The depth of the tube on average for a female patient is 19 -21 at teeth.

Intubation Procedure Confirm tube position: üBy auscultation of the chest üBilateral chest rise üTube location at teeth üCO 2 detector – (esophageal detection device)

Intubation Procedure Stabilize the ETT

Q: Describe suction procedure for ventilated patients.

TROUBLESHOOTING

Troubleshooting u Is it working ? –Look at the patient !! –Listen to the patient !! –Pulse Ox, ABG, Et. CO 2 –Chest X ray –Look at the vent (PIP; expired TV; alarms)

TROUBLESHOOTING u Anxious Patient – Can be due to a malfunction of the ventilator – Patient may need to be suctioned – Frequently the patient needs medication for anxiety or sedation to help them relax u. Attempt to fix the problem u. Call your doctor

Low Pressure Alarm u Usually due to a leak in the circuit. – Attempt to quickly find the problem – Bag the patient and call your doctor

High Pressure Alarm u Usually caused by: – A blockage in the circuit (water condensation) – Patient biting his ETT – Mucus plug in the ETT – You can attempt to quickly fix the problem – Bag the patient and call for your doctor
")
Low Minute Volume Alarm u Usually caused by: – Apnea of your patient (CPAP) – Disconnection of the patient from the ventilator – You can attempt to quickly fix the problem – Bag the patient and call for your doctor

Accidental Extubation u Role of the Nurse: – Ensure the Ambu bag is attached to the oxygen flowmeter and it is on! – Attach the face mask to the Ambu bag and after ensuring a good seal on the patient’s face; supply the patient with ventilation. – Bag the patient and call for your doctor

OTHER u Anytime you have concerns, alarms, ventilator changes or any other problem with your ventilated patient. –Call for your doctor –NEVER hit the silence button!

Trouble Shooting

ABG • Goal: • Keep patient’s acid/base balance within normal range: • p. H • PCO 2 • PO 2 7. 35 – 7. 45 35 -45 mm. Hg 80 -100 mm. Hg

Complications u Ventilator Induced Lung Injury –Oxygen toxicity –Barotrauma / Volutrauma u. Peak Pressure u. Plateau Pressure u. Shear Injury (tidal volume) u. PEEP

Complications u Cardiovascular Complications – Impaired venous return to RH – Bowing of the Interventricular Septum – Decreased left sided afterload (good) – Altered right sided afterload u Sum Effect…. . decreased cardiac output (usually, not always and often we don’t even notice)

Complications u Other Complications –Ventilator Associated Pneumonia –Sinusitis –Sedation –Risks from associated devices (CVLs, A-lines) –Unplanned Extubation

Extubation u Weaning – Is the cause of respiratory failure gone or getting better ? – Is the patient well oxygenated and ventilated ? – Can the heart tolerate the increased work of breathing ?
 – decrease the PEEP (4 -5) – decrease the")
Extubation u Weaning (cont. ) – decrease the PEEP (4 -5) – decrease the rate – decrease the PIP (as needed) u What you want to do is decrease what the vent does and see if the patient can make up the difference….

Extubation u Extubation – Control of airway reflexes – Patent upper airway (air leak around tube? ) – Minimal oxygen requirement – Minimal rate – Minimize pressure support (0 -10) – “Awake ” patient

Mechanical Ventilators Different Types of Ventilators Available: Will depend on you place of employment

Mechanical Ventilators

Mechanical Ventilators

Mechanical Ventilators

Mechanical Ventilators

Mechanical Ventilators

High Frequency Mechanical Ventilator


- Slides: 89