CHRONIC KNEE PAIN Shane Cass DO UNM Sports






























- Slides: 33
CHRONIC KNEE PAIN Shane Cass, DO UNM Sports Medicine
OBJECTIVES • Provide a comprehensive case based review of chronic knee pathology • Review clinically relevant anatomy • Synthesize a diagnosis and differential • Appropriately use relevant radiological studies • Provide a rational and useful treatment plan
REFERENCES • To get the most out of this module go to the link below. Here you’ll find great MSK articles by the AAFP. • AAFP MSK Modules • Also please click the link below to review a complete knee exam • Knee exam video
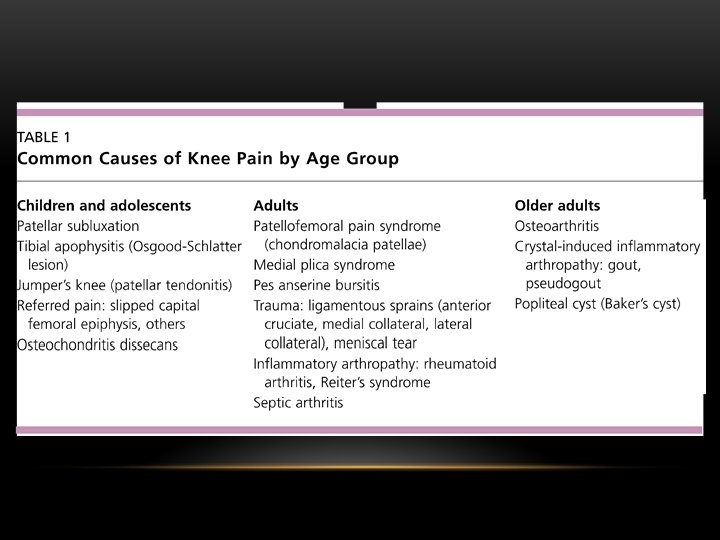
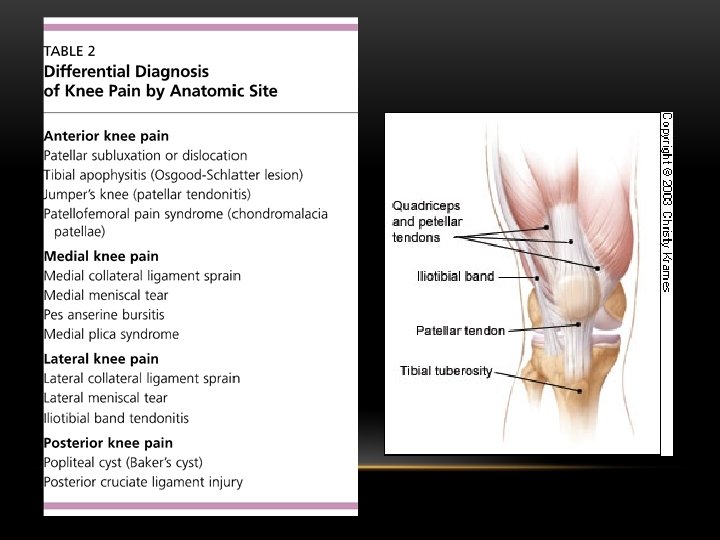
HIGH YIELD ARTICLES FOR THIS MODULE • Evaluation of patients presenting with knee pain • Differential Diagnosis of Knee Pain • Treatment of Knee Osteoarthritis • Non-surgical Management of Knee Pain
ANATOMY
INTERNAL KNEE ANATOMY
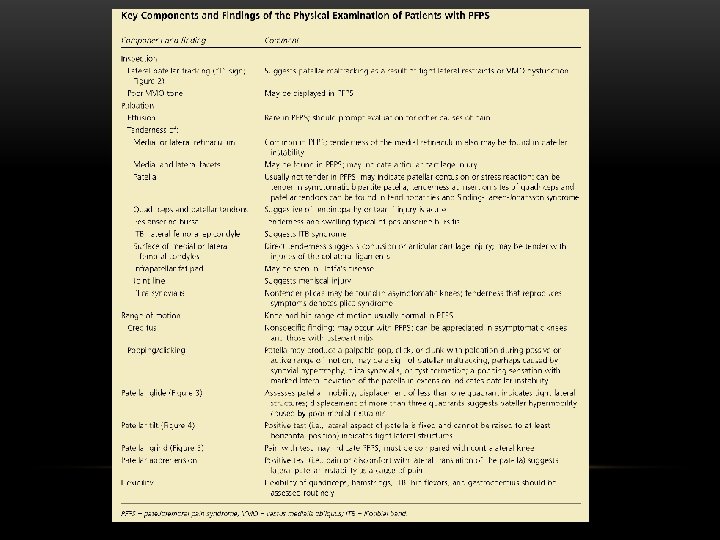
AN 18 YEAR OLD FEMALE VOLLEYBALL PLAYER PRESENTS TO YOUR OFFICE WITH ANTERIOR KNEE PAIN FOR THE LAST 3 MONTHS. SHE DESCRIBES THE PAIN AS PERI-PATELLAR AND “DEEP. ” THERE WAS NO INJURY, BUT THE PAIN STARTED DURING HER SUMMER LEAGUE AFTER DOING NEW HITTING DRILLS. SHE REPORTS NO SWELLING OR MECHANICAL SYMPTOMS, BUT SOMETIMES IT POPS. • True or false: One might find the below exams to be negative. • False: These tests are often positive in Patellofemoral Pain Syndrome Patellar Mobility Testing Patellar Grind Test
PFPS RISK FACTORS
TREATMENT • What treatment has the best level of evidence for PFPS? • 1. Lateral Release Surgery • 2. Corticosteroid Injection • 3. Physical Therapy • 4. Taping Sort Level A SORT Level B Read the whole article here
SUPPOSE OUR IDENTICAL PATIENT HAD A HISTORY OF TRAUMA, AN EFFUSION AND POSITIVE APPREHENSION TEST? WHAT IS HER MOST LIKELY DEFINITION • 1. PFPS • 2. Patellar tendonitis • 3. Tibial apophysitis (Osgood-Schlatter Lesion) • 4. Patellar subluxation or dislocation True or False: The finding in this case making it least likely PFPS is the presence of an effusion. TRUE
OUR PATIENT HAS A 14 YEAR OLD BROTHER WHO PLAYS SOCCER AND IS ALSO HAVING ANTERIOR KNEE PAIN. HE RECALLS NO INJURY AND GETS PAIN WITH STAIRS AND JUMPING. THERE IS TTP OVER THE TIBIAL TUBEROSITY AND NO EFFUSION. WHAT IS HIS MOST LIKELY DIAGNOSIS? • 1. PFPS • 2. Patellar tendonitis • 3. Tibial apophysitis (Osgood-Schlatter Lesion) • 4. Patellar subluxation or dislocation The diagnosis of tibial apophysitis does not require an x-ray for diagnosis. But what if this same patient presented with an acute or subacute injury? Should you get an x-ray then? YES! He has open growth plates and may have an avulsion fracture. The growth plate is the weakest link in the MSK system for the skeletally immature and they are more likely to fracture than undergo ligamentous injury.
Type IIIa Only Type 1 a can be treated without surgery and requires cast
A SIMILAR PRESENTATION WITH PAIN DIRECTLY OVER THE PATELLAR TENDON INSTEAD OF THE TIBIAL TUBERCLE WITH NO INJURY MIGHT INDICATE WHAT? • 1. PFPS • 2. Patellar tendonitis • 3. Tibial apophysitis (Osgood-Schlatter Lesion) • 4. Patellar subluxation or dislocation True or False: Best treatment for this would be Rest, NSAIDS, activity modification and physical therapy. TRUE
WHAT IF OUR 14 YEAR OLD MALE HAD VAGUE AND POORLY LOCALIZED KNEE AND DISTAL THIGH PAIN? THERE WAS NO HISTORY OF TRAUMA. HE WALKS WITH A LIMP. HE HAS A NORMAL KNEE EXAM BUT LIMITED INTERNAL ROTATION OF THE HIP WITH OBLIGATORY EXTERNAL ROTATION WHEN HIP IS BROUGHT INTO 90 DEGREES OF PASSIVE FLEXION. • What should you do next? • 1. Prescribe naprosyn • 2. Prescribe physical therapy • 3. Order a hip x-ray series (AP and frog-leg lateral) • 4. Reassure the parents the knee exam is unremarkable and that this is something he’ll outgrow.
What is the diagnosis from this history and these images? 1. Hip Apophysitis 2. Slipped Capital Femoral Epiphysis 3. Legg-Calve-Perthes Disease 4. Septic Arthritis
SCFE SHOULD ALWAYS BE IN THE DIFFERENTIAL FOR VAGUE KNEE PAIN AND A LIMP IN ADOLESCENTS (SORT LEVEL C)
XRAY FINDINGS CAN BE SUBTLE
DON’T MISS THIS! • Treatment is emergent surgical consultation and complete non-weight bearing • Lesions typically require surgical fixation and possible reduction to reduce risk of osteonecrosis and further bone degradation. Read the full article on SCFE here
THEIR 19 YEAR OLD BROTHER RUNS CROSS COUNTRY AT A DIVISION II SCHOOL AND IS YOUR NEXT PATIENT WITH DIFFUSE LATERAL KNEE PAIN. THE PAIN STARTED WHEN HE WENT FROM 50 MILES A WEEK TO 90 AT COLLEGE. HE WAS ABLE TO MAKE IT THROUGH THE SEASON BUT NOW CAN HARDLY RUN. THERE WAS NO INJURY. • The pain used to come at the end of the run but now happens at the beginning and is noticeably worse with running down hill or when he lengthens his stride. • There is TTP at the lateral femoral condyle and Ober and Noble test are both positive. Hop test is negative. • What is the likely diagnosis? • 1. IT Band Friction Syndrome • 2. Femoral Stress Fracture • 3. Biceps Femoris Tendinopathy • 4. Lateral Meniscal Tear
GIVEN HIS PRESENTATION WHAT SHOULD YOU RULE OUT ALSO • 1. IT Band Friction Syndrome • 2. Femoral Stress Fracture The rapid increase in mileage should • 3. Biceps Femoris Tendinopathy • 4. Lateral Meniscal Tear prompt you to consider stress fracture.
OBER AND NOBLE TEST Noble Test Video Ober Test
TRUE OR FALSE: STRETCHING AND REHAB ARE EFFECTIVE FOR IT BAND SYNDROME. • True. SORT level B indicates stretching and strengthening of hip rotators, especially the gluteus medius, are effective in treating IT Band Syndrome. Read the full article here
YOU SEE THIS SAME PATIENT A YEAR LATER AND HIS IT BAND SYNDROME IS RESOLVED. HOWEVER, OVER THE SUMMER HE DEVELOPED MEDIAL KNEE PAIN THAT STARTED AFTER ADDING INTERVAL TRAINING ON THE TRACK. HE DENIES ANY INJURY. THERE IS NO EFFUSION. HE HAS PAIN JUST DISTAL AND POSTERIOR TO THE MEDIAL JOINT LINE. VALGUS STRESS TESTING ELICITS PAIN. • What is the most likely diagnosis? • 1. Medial Collateral Ligament Sprain • 2. Pes Anserine Bursitis • 3. Medial Meniscal Tear • 4. Medial Plica Syndrome Refer to PT
YOUR PATIENT’S 55 YEAR OLD FATHER COMES IN FOR EVALUATION OF BILATERAL KNEE PAIN. HE DENIES ANY ACUTE INJURY AND NOTES PAIN IS AGGRAVATED BY WEIGHT BEARING ACTIVITIES AND USUALLY RESOLVED BY REST. IN THE MORNING HE IS STIFF BUT IT RESOLVES WITH ACTIVITY WITHIN 10 MINUTES. HE HAS MILD BILATERAL EFFUSIONS AND MEDIAL FEMORAL AS WELL AS TIBIAL PLATEAU PAIN. HE ALSO HAS MEDIAL JOINT LINE PAIN. • You get an x-ray… • Given his joint line pain, should you also consider an MRI? • NO! Treat the obvious osteoarthritis here.
WHAT IF HIS X-RAYS WERE NORMAL? CAN YOU DIAGNOSIS OSTEOARTHRITIS WITH NORMAL XRAYS? • YES! The diagnosis of osteoarthritis is a clinical diagnosis and x-rays are not necessary for all patients. See the American College of Rheumatology Diagnostic Algorithm
YOUR PATIENT IS NOT INTERESTED IN ANY SURGICAL OPTIONS. WHICH OF THE BELOW IS TRUE REGARDING OSTEOARTHRITIS TREATMENT? • 1. NSAIDS and acetaminophen are in-effective for reducing pain. • 2. Opioids should be considered as first line treatment. • 3. Intra-articular corticosteroid injections provide no benefit in studies. • 4. Water or land based exercise, aerobic walking, quad strengthening and resistance exercise are effective for reducing pain and disability from knee osteoarthritis
SORT Level A for CSI injections, NSAIDS and PT/aerobic/resistance training Read the full article for treating osteoarthritis here
INJECTION THERAPY • There are multiple approaches and variations to doing knee injections. See below for an article describing one way. You’ll get more experience with injections during your Sports Medicine Rotation. • Article on knee arthrocentesis
YOUR PATIENT HAS HEARD ABOUT KNEE ARTHROSCOPY, AND THINKS HE WOULD BE MORE INTERESTED IN THAT THAN TOTAL KNEE REPLACEMENT. IS KNEE ARTHROSCOPY EFFECTIVE FOR TREATMENT OF OSTEOARTHRITIS? • No. A 2006 Cochrane review showed high-quality evidence that arthroscopic debridement has NO BENEFIT for typical osteoarthritis of the knee (mechanical or inflammatory causes). • Read the Cochrane Review Here • Knee osteoarthritis is very common in primary care. Get good at managing it and you’ll help many of your patients.
FOR SUGGESTIONS ON IMPROVING THIS EDUCATIONAL MODULE CONTACT ME BELOW BY E-MAIL… • scass@salud. unm. edu