ACUTE SHOULDER INJURIES Shane Cass DO UNM Sports







 •")


































- Slides: 45
ACUTE SHOULDER INJURIES Shane Cass, DO UNM Sports Medicine
OBJECTIVES • Provide a comprehensive case based review of shoulder pathology • Review clinically relevant anatomy • Synthesize a diagnosis and differential • Appropriately use relevant radiological studies • Provide a rational and useful treatment plan including
REFERENCES • To get the most out of this module go to the link below. Here you’ll find great MSK articles by the AAFP. • AAFP MSK Modules • Also please click the link below to review a complete shoulder exam • Shoulder exam video
HIGH YIELD ARTICLES FOR THIS MODULE • Acute Shoulder Injuries • The Painfull Shoulder Part I: Clinical Evaluation • The Painfull Shoulder Part II: Acute and Chronic Disorders • Diagnosing Rotator Cuff Tears: Point of Care
A 25 YEAR OLD WITH ACUTE SHOULDER PAIN • A 25 year old male cyclist comes into the office after being ran off the rode on Tramway. He fell directly on his right shoulder and felt a popping sensation followed by extreme pain. • What is on your differential?
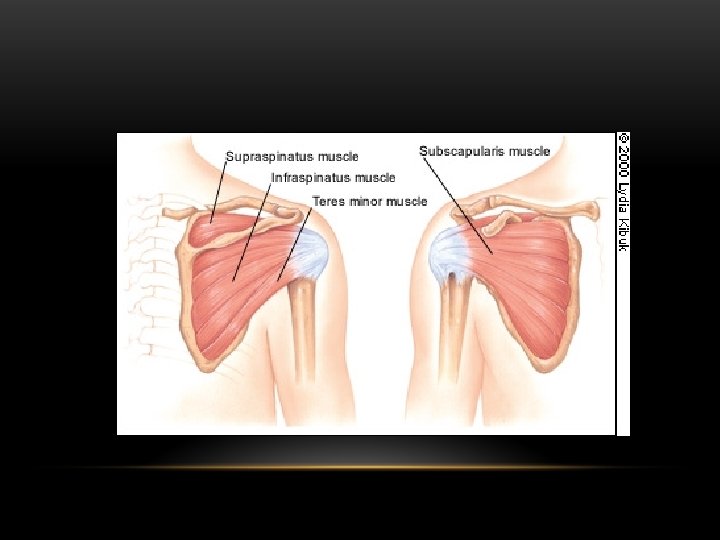
ANATOMY
KEY HISTORY ITEMS • Mechanism of injury • Sport/activity, work • Handedness • Duration of pain • Activities and motions causing pain
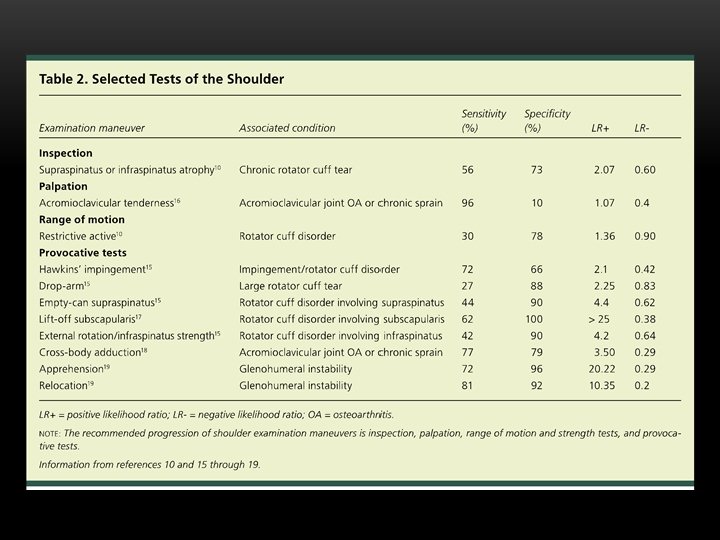
EXAMINATION • General Inspection • Palpation • Range of motion (passive and active) • Strength testing (rotator cuffs, deltoid, pectorals) • Impingement Testing (Neer’s and Hawkins) • Biceps testing (Speed’s and Yergusons) • Labral Assessment (Obrien’s, Crank) • Stability Testing (Apprehension testing, Shift and Load, Sulcus Sign)
STRENGTH TESTING ROTATOR CUFF
IMPINGEMENT Neer’s Test Hawkin’s Test
GENERAL INSPECTION • He has an obvious deformity and won’t let you palpate his clavicle • You get an x-ray
RADIOGRAPH
CLAVICLE FRACTURES
WHAT IS THE BEST TREATMENT? • A. Figure of Eight Sling • B. Normal sling with RICE treatment and early range of motion • C. Orthopedic Surgical Evaluation
TREATMENT • SORT Level A evidence for not using figure of eight sling • Group 1 represents 80% of all clavicle fractures. Treat with regular sling for comfort, Ice, NSAIDS, early range of motion. • Group 2 may need surgical consultation if into AC joint • Group 3 can be treated conservatively if no thoracic trauma and nondisplaced, otherwise referral to orthopedics is appropriate Group 2 SC Dislocation
WHAT IF THE PATIENT IS 85… • He fell off his bike at a stop light and reached out his arm to stop the fall • He is diffusely tender over the humeral head and point tender at the greater tuberosity; there is noted ecchymosis. • You get a radiograph
Humeral Head Fracture
Refer displaced fractures, fractures with >45 degree angulation, open fractures, neurovascular or neurological deficits, fracture dislocations, and fractures of the anatomic neck
WHAT IS MISSING FROM OUR RADIOGRAPHS? • All shoulder x-rays should include a true AP (Grashey), Axillary View, and Scapular Y
Axillary View Scapular Y View Anterior Shoulder Dislocation
SHOULDER DISLOCATIONS • 90% Anterior • Obvious deformity and guarding, patient will cradle their arm • Bulge where humeral head rests, empty space beneath acromion • Evaluate for neurovascular compromise (think axillary nerve) • Get x-rays to rule out fracture • Early reduction prior to muscle spasms if possible • Late reduction generally requires anesthesia
REDUCTION TECHNIQUES • Learn two to keep at your disposal • I prefer Fares, Spaso and Stinson • https: //www. youtube. com/watch? v=8 xibz. OM 7 Hp 0
POST REDUCTION TREATMENT • “Relative” immobilization in a sling for 3 -4 weeks. • Rehabilitation • High rate of recurrent dislocation in those < 25 years old • 67 -97% likelihood of repeat dislocation within the year • Better outcomes with early surgical intervention in young athletic populations • Don’t forget to always check your axillary nerve function pre and post reduction and document it!
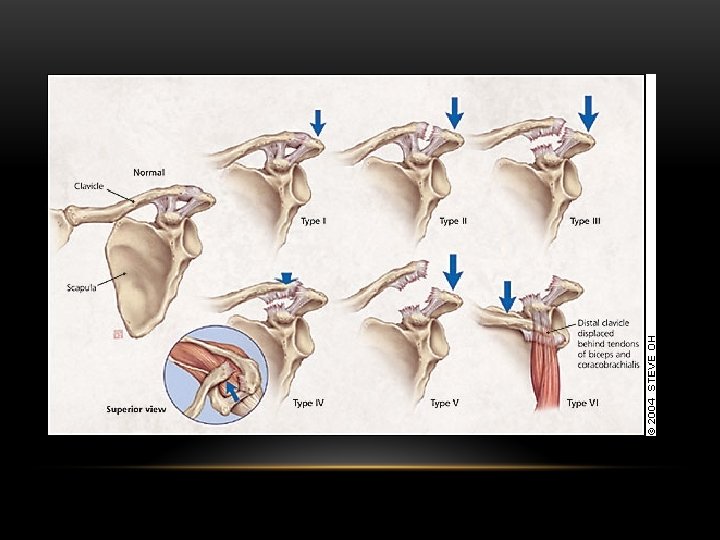
WHAT IF GROSS EXAM SHOWED THIS? Acromioclavicular Sprain
AC JOINT SPRAINS • Direct blow to acromion with humerus adducted or sometimes FOOSH or fall on elbow • AC Ligament first damaged • Enough force damages coracoclavicular ligament and delto pectoral fascia causing it to rise superiorly • Type 1 injuries with no gross deformity and pain over AC joint with pain with cross over • Cross Stress x-rays are debatable. Zanca view is a dedicated AC view. Arm Abduction Test
AC JOINT SPRAIN TREATMENT • Consider referral to orthopedics for types IV-VI • Treat type I and II nonoperatively with a sling for 1 -3 weeks, NSAIDS and RICE treatment. • Once acute pain resolved, ROM followed by strengthening. • Return to activities when pain free function is restored • Type III is controversial, if non-operative decided treat same as I and II injuries, with longer immobilization (2 -4 weeks) • Type IV-VI require internal fixation
BACK TO OUR CASE… • Another 50 year old mountain biker finished his ride in the foothills. While lifting his heavy mountain bike onto the rooftop rack of his Land Rover he felt a sharp pain and tearing sensation in his shoulder.
WHICH PHYSICAL EXAM FINDINGS ARE MOST CONSISTENT WITH ROTATOR CUFF TEAR • A. Subscapularis Weakness • B. Impingement Signs (Neer’s Test) • C. Painful Arc • D. Internal rotation weakness • E. B and C • F. All of the above
2 CLINICAL DECISION RULES FOR PREDICTING ROTATOR CUFF TEARS • Supraspinatus Weakness, External Rotation Weakness and Impingement signs 98% probability of cuff tear with all 3 signs, or age > 60 with 2 signs • Painful arc sign is 97% sensitive for rotator cuff tear. Good negative predictive value Read the article here
PAINFUL ARC SIGN
IMAGING? • Suspecting a rotator cuff tear you decide to get imaging. Can we see anything on plain film, or should we just go to the MRI? • Always get plain films! • Rotator cuff tears on plain films may present with superior migration of the humeral head due to the force of the deltoids, especially on large new tears
RADIOGRAPH
ROTATOR CUFF TEARS • Common in patient’s > 40 • Full thickness tears in younger patients present usually with significant trauma • In older or middle age may present as chronic impingement • MRI is the gold standard , 95% sensitive and specific for diagnosing full thickness cuff tear (Big problem is diagnosing asymptomatic cuff tears)
WHO SHOULD GET SURGERY? • A. All full thickness rotator cuff tears • B. Younger patients with full thickness rotator cuff tears • C. Younger patients with any rotator cuff tear (full thickness or partial thickness) • D. All of the above
TREATMENT • Young active patients with acute full thickness tears and severe functional deficiet are most likely to respond to surgical treatment and should be referred to arthroscopy within 3 weeks of injury to decrease risk of retraction and atrophy • Competitive athletes tend to do better with surgery, despite their age • Studies show many older patient’s achieve functional improvement and pain reduction with conservative treatment • Conservative treatment starts with relative rest and restriction of movement for 1 -2 weeks with RICE and NSAIDS. PT for ROM followed by strengthening. Sometimes subacromial bursal injections can help.
WHAT IF THE CUFF TEAR INCREASES? • See the natural history of rotator cuff tears at this link (need to be logged into HSC Library)… • Natural History Cuff tears; systematic review
MOVING INTO A GREY AREA… • A 55 year old former police officer comes in with acute on chronic pain for the past 3 weeks. He reports a remote injury 5 years ago restraining someone in the line of duty. His pain has been off and on since, managed with rest and activity modification, until a recent injury lifting a large box in his garage. He now has pain with overhead activity and he can’t lie on his shoulder at night. Pain is anterolateral. • What exam finding is most likely to be positive in this patient? • A. Spurling’s Test • B. Hawkins Sign • C. Speed’s Test • D. O’Brien’s Test
IMPINGEMENT SYNDROME • A series of pathological changes that leads to soft tissue structures impinged on the acromion with arm abduction. 4 stages described by Neer… • 1. Injury causing hemorrhage and edema • 2. Tendonitis and fibrosis • 3. Tendon degeneration of rotator cuff and biceps tendon • 4. Bony changes and tendon rupture
EXAM • Positive Impingement Signs Neer’s and Hawkin’s
TREATMENT • Initial treatment is conservative; rest, activity modification, ice and NSAIDS. ROM should be instituted early and strengthening programs with home exercise or PT when pain free. • True or False: A subacromial injection has no benefit for acute impingement syndrome? • FALSE • Subacromial injections in the acute phase of impingement have significant pain relieving benefits in the first 4 -6 weeks. Long term effects are less convincing from the literature • Blair B, Rokito AS, Cuomo F, Jarolem K, Zuckerman JD. Efficacy of injections of corticosteroids for sub-acromial impingement syndrome. J Bone Joint Surg [Am]. 1996; 78: 1685– 9.
WHAT ABOUT IMAGING? • Plain films may be considered initially to determine bony deformities such as a curved or hooked acromion or AC joint spurs. • Imaging should be considered if no improvement with conservative treatment in 4 -6 weeks • MRI should be considered to evaluate rotator cuff integrity if surgery is desired. • Subacromial decompression with bursectomy and acromioplasty may be considered if no improvement with conservative treatment Down sloping acromion
FOR SUGGESTIONS ON IMPROVING THIS EDUCATIONAL MODULE CONTACT ME BELOW BY E-MAIL… • scass@salud. unm. edu