Chapter 17 18 Neuroendocrine System Contains the hypothalamus


 FSH:")
: controls plasma osmolality (antidiuretic hormone) § Regulated by")


























 : increased ACTH, decreased cortisol and")


 § Hydrocortisone §")




- Slides: 44
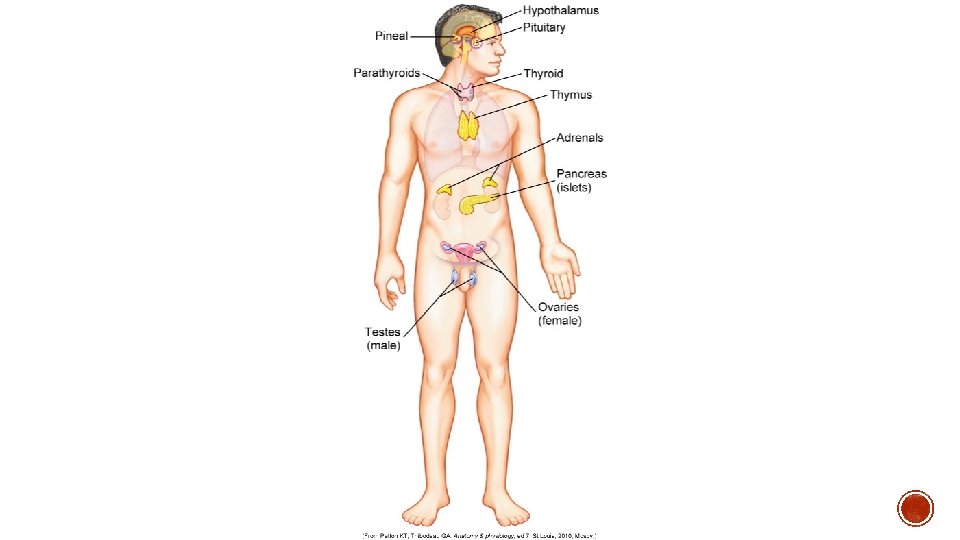
Chapter 17 & 18
§ Neuroendocrine System § Contains the hypothalamus and Pituitary Gland § Controls thyroid, adrenal and reproductive function
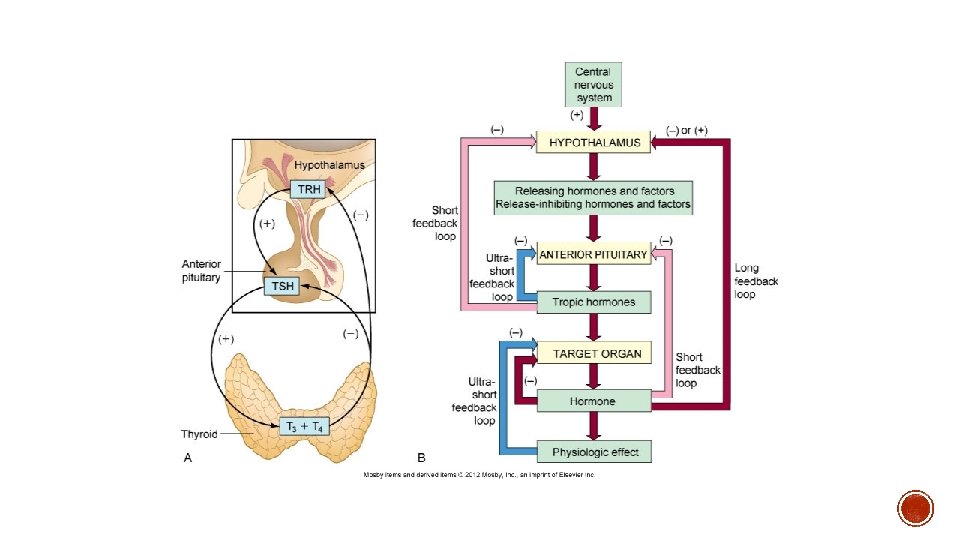
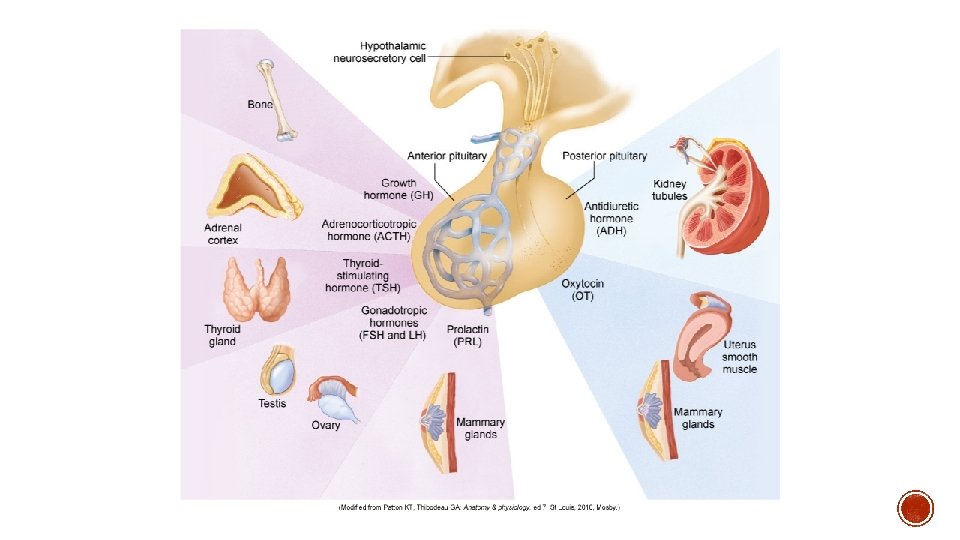
§ TROPIC HORMONES § § § MSH: secretion of melanin (melanocyte stimulating hormone) FSH: estrogen production and spermatogenesis (follicle stimulating hormone) LH: ovulation, progesterone and testosterone production (luteinizing hormone) ACTH: cortisol production and maintenance of adrenal gland (adrenocorticotropic hormone) TSH: thyroid hormone production (thyroid stimulating hormone) GH: skeletal muscle growth, regulates metabolism, necessary for stress adaptation (growth hormone) § Regulated by GHRH and Somatostatin § IGF-1 and IGF-2 (insulin-like growth factor) § Prolactin: milk production (lactation)
§ POLYPEPTIDE HORMONES § ADH (vasopressin): controls plasma osmolality (antidiuretic hormone) § Regulated by glutamate and GABA § Increased release with stress, trauma, decreased intravascular volume § Decreased release with decreased plasma osmolality and increased intravascular volume § Oxytocin: uterine contraction and milk ejection § Also has some antidiuretic effects
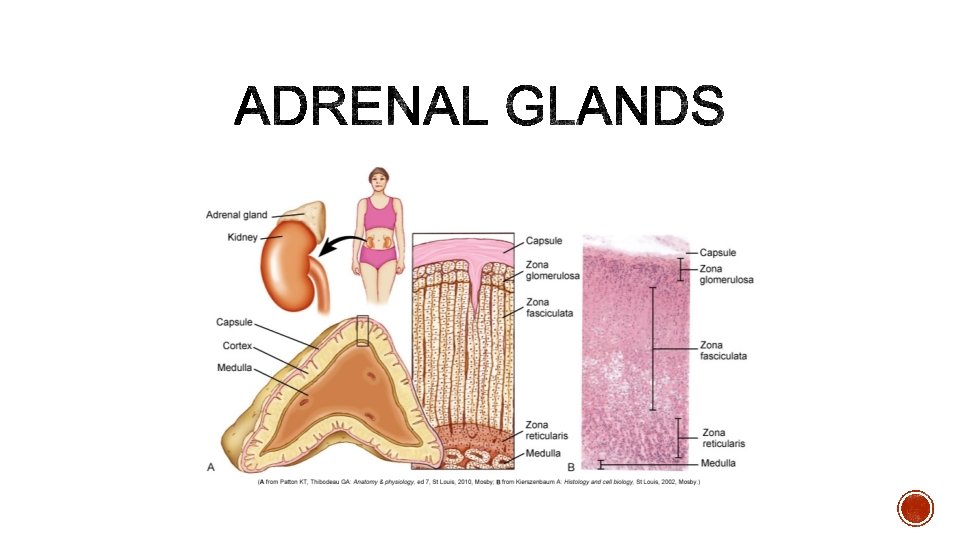
§ Adrenal Medulla § Catecholamine secretion § Epinephrine and norepinephrine
§ Adrenal Cortex § Glucocorticoids § Carbohydrate metabolism, immune suppression, anti-inflammatory effects, suppress bone formation, suppress ADH secretion, stimulate gastric acid secretion § In high levels cause: § Increased appetite, fat deposits in face, abdomen, upper back, hypocalcemia, decreased ACTH synthesis
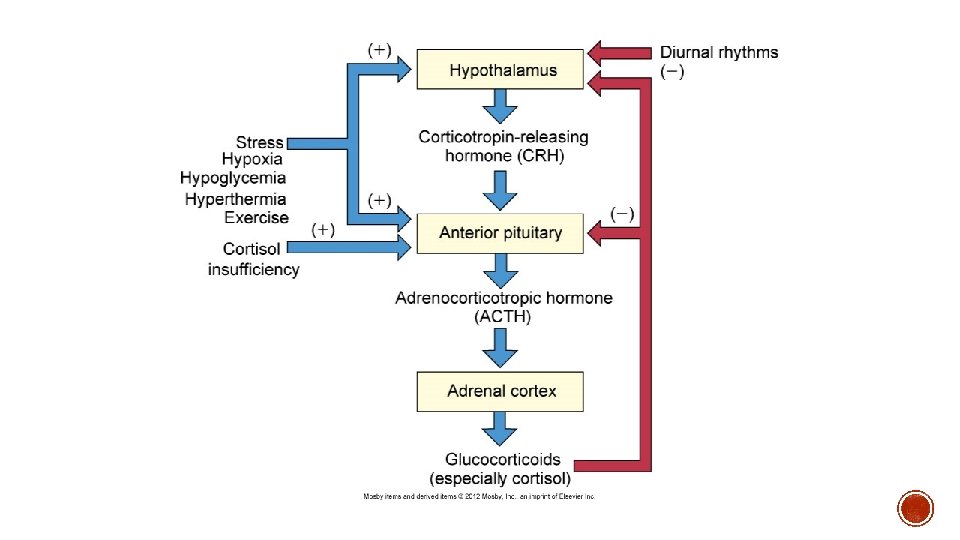
§ Cortisol § CRH ACTH cortisol secretion § Potent naturally occurring glucocorticoid § Necessary for maintenance of life § Diurnal release of ACTH § Negative feedback loop associated with ACTH release § Increased release: low levels of circulating cortisol; stress reactions § Decreased release: high levels of circulating cortisol; synthetic glucocorticoid use
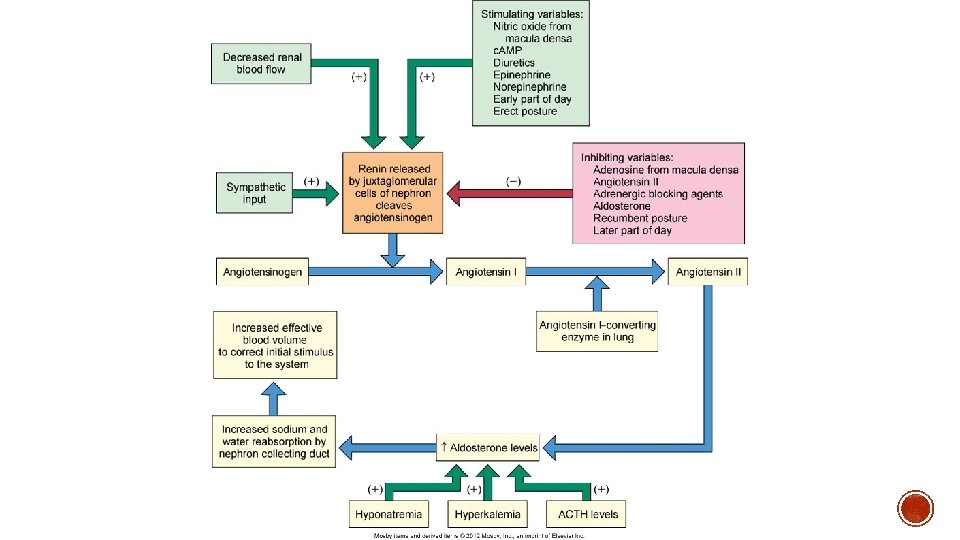
§ Mineralcorticoids § Aldosterone § Natural occurring mineralcorticoid § Promotes sodium retention and potassium excretion § Regulated by the renin-angiotensin system (primarily angiotensin II) § Sodium and water depletion § Hyperkalemia § Decreased blood volume
§ 1. Inadequate Synthesis § Precursor dysfunction § 2. Failure of Feedback Systems § Too much or too little hormone synthesis § 3. Inactive Hormones § Directly inhibited or degraded § 4. Ineffective Hormone Delivery § Decreased blood supply § Inadequate carriers § 5. Decreased Target-Cell Sensitivity § Too little receptors § Presence of antibodies on receptors
§ Increased ADH release regardless of plasma osmolality § Causes: § Neoplasms § Pulmonary disorders § CNS disorders § Medications
§ Manifestations: § HYPONATREMIA § Thirst § Dyspnea § Fatigue § Vomiting § Confusion (late) § Lethargy (late) § Convulsions (late) § Irreversible neurological damage (late)
§ Diagnostics: § Serum hypoosmolality § Serum hyponatremia § Urine hyperosmolality § Normal adrenal, thyroid, and renal function § Resistant hyponatremia § Treatment: § Fluid restriction § Hypertonic solutions § Use of demeclocycline
§ Tetracycline drug class § Has unique side effect of stimulating urine flow § Used for SIADH
§ Decreased ADH release § Causes: § Neurogenic § Insufficient secretion of ADH § Interference of ADH synthesis (brain tumors, aneurysm, infection, thrombosis) § Nephrogenic § Renal tubules do not respond appropriately to ADH § Acquired § Pyelonephritis, polycystic kidney disease, anesthetics, medications § Genetic
§ Manifestations: § Polyuria § Nocturia § Thirst § Polydipsia § Dilute urine § Urine hypoosmolality § Serum hypernatremia § Serum hyperosmolality
§ Treatment: § Desmopressin § Treatment of underlying cause
§ Vasopressin § Antidiuretic hormone § Promotes renal conservation of water, increasing permeability of renal tubules § Used for Diabetes Insipidus § Given intranasally, SQ, IV, or PO § Adverse effects: § Excessive water retention § Limited side effects
§ Causes: § Inadequate Hypothalamic Releasing Hormones § Inadequate anterior pituitary gland § Infarction § Adenoma § Damage to pituitary stalk § Meningitis § Tuberculosis § Autoimmune disorders
§ Manifestations: § Deficient ACTH : anorexia, fatigue, hypoglycemia § Deficient TSH : cold intolerance, lethargy, decreased metabolism § Deficient FSH and LH : amenorrhea, testicular atrophy, decreased libido § Deficient GH : hypopituitary dwarfism (children) Feeling of poor well-being, osteoporosis, fatigue (adult) generalized complaints Panhypopituitarism (all anterior pituitary hormones are deficient)
§ Acromegaly § Prolonged exposure to increased GH and IGF-1 § Middle aged adults § Rare § Slowly progressive § Cause: § Pituitary adenoma
§ Manifestations: § Enlarged tongue § Enlarged sweat glands § Coarse skin § Excessive body hair § Enlargement of facial bones (protrusion of forehead and jaw) § Enlargement of hands and feet
§ Treatment: § Surgical removal of GH secreting adenoma § Radiation § Octreotide § Lanreotide § Pegvisomant
§ Ocreotide § IM injection § Indicated for acromegaly § Adverse effects: § GI symptoms § gallstones § Lanreotide § Prefilled SQ syringe § Adverse effects: § Diarrhea § gallstones
§ Pegvisomant § Most effective drug option for acromegaly § SQ injection § Expensive § Adverse effects: § GI upset § Chest pain § Flu-like symptoms § Monitor hepatic function
§ Prolactinoma § Sustained, elevated release of prolactin § Manifestations: § Galactorrhea § Amenorrhea § Treatment: § Bromocriptine § Cabergoline § Causes: § Pituitary tumor
Ergot derivatives Cabergoline -PO with or without food -can be used to correct amenorrhea, infertility and galactorrhea associated with a prolactinoma -can also cause tumor regression -immediate effects of decreased prolactin secretion -should monitor prolactin monthly until normal, treatment can stop after 6 months of normal levels -adverse effects: nausea, headache, dizziness Bromocriptine Similar, except is not tolerated as well as cabergoline
§ HYPERCORTISOLISM § Cushing Syndrome § Chronic exposure to excessive cortisol § Cushing Disease § Excessive secretion of ACTH § Cushing-Like Syndrome § Administration of synthetic glucocorticoids
§ Manifestations: § Weight gain § Fat deposits in face, trunk and cervical area (moon face, buffalo hump) § Glucose intolerance (hyperglycemia) § Protein wasting (thin extremities) § Osteoporosis § Collagen loss (thin, weak skin, striae, bruising) § Increased catecholamine activity (hypertension) § Increased mineralcorticoid activity (edema, potassium loss) § Cushing Disease in Females (increased androgen levels) § Increased hair growth § Acne § amenorrhea
§ Diagnostics: § Urine cortisol § Dexamethasone suppression test § Measurement of ACTH and cortisol levels
§ Treatment: treat underlying cause tumor removal radiation therapy Ketoconazole antifungal, but also blocks glucocorticoid synthesis 600 -800 mg/day (high doses) must monitor liver enzymes at this high dose
§ HYPOCORTISOLISM § Addison’s Disease (Primary Adrenal Insufficiency) : increased ACTH, decreased cortisol and aldosterone § Secondary Adrenal Insufficiency : decreased ACTH § Causes: § Autoimmune attack of the adrenal cortex (Primary Adrenal Insufficiency) § Prolonged administration of glucocorticoids (Secondary Adrenal Insufficiency) § Pituitary tumors (Secondary Adrenal Insufficiency) § Infections (tuberculosis)
§ Manifestations: § Weakness § Fatigue § Hyperpigmentation of the skin (only in Addison’s disease) § Weight loss § Hypotension § Hypoglycemia § Syncope
§ Diagnostics: § Hyperkalemia § Hyponatremia § Hypoglycemia § Decreased serum and urine cortisol § Increased ACTH (Addison’s Disease)
§ Treatment: § Lifelong glucocorticoid supplementations (higher doses during acute stressors) § Hydrocortisone § Mineralcorticoid supplementation § Fludrocortisone
§ Hydrocortisone § For use in Addison’s Disease § Take entire dose in am or 2/3 in am and remainder in afternoon § Lifelong supplementation § Increased dose at times of stress § Excessive doses can produce symptoms of Cushing’s Syndrome
§ Fludricortisone § Mineralcorticoid replacement § 0. 1 mg PO daily § Used in combination with glucocorticoid § Adverse effects: § With high doses § Hypertension § Hypokalemia § Weight gain § Edema
§ Caused by adrenal adenomas or carcinomas § Feminization: development of female secondary sex characteristics § Gynecomastia, testicular atrophy, decreased libido, early development of sex characteristics § Virilization: development of male secondary sex characteristics § Excessive face/body hair growth, clitoral enlargement, amenorrhea, acne, breast atrophy
§ PHEOCHROMOCYTOMA § Causes continuous, excessive secretion of catecholamines § Rare and can be malignant § Manifestations: § Hypertension, tachycardia, diaphoresis, palpitations, headaches, hypermetabolism § Treatment: § Check for excessive catecholamines in blood and urine § Surgical removal of tumor § Alpha and beta blockers