ANTIANGINAL AGENTS Lector prof Posokhova K A ISCHEMIC




 drugs a group of drugs which by different mechanisms abolish irregularities")
 DRUGS І. Nitrates and sidnonimins ІІ. Beta-adrenoblockers ІІІ. Antagonists of calcium")

 groups (nitrate receptors) inside")

 1 % alcohol or oil solution")














, duration")




")
 2. Derivatives of benzothiazepine (dylthiazem) 3.")



")
")
")











- Slides: 50
ANTIANGINAL AGENTS Lector prof. Posokhova K. A.
ISCHEMIC HEART DISEASE 2, 4 mln. people die from IHD annually
ISCHEMIC HEART DISEASE There are 35 risk factors for development of IHD 3 the most important ones are – “big triple” hypercholesterolemia arterial hypertension smoking 95 % of patients with IHD are observed to have atherosclerotic changes in coronary arteries
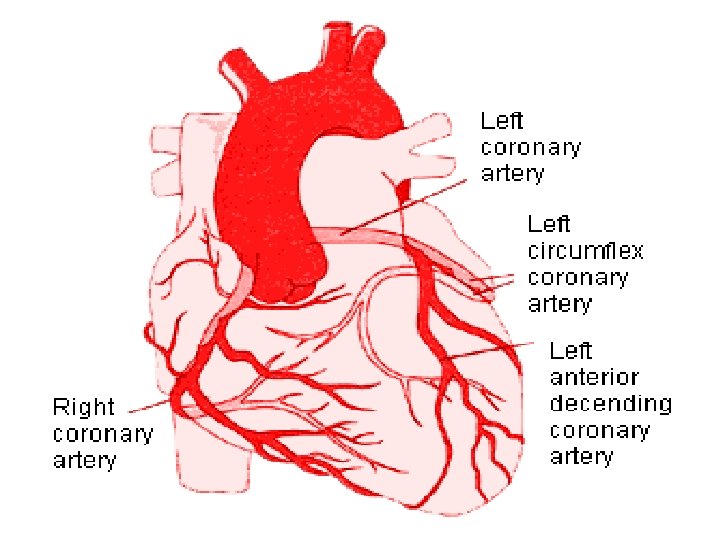
Atherosclerotic changes in coronary arteries
Antianginal (coronary active) drugs a group of drugs which by different mechanisms abolish irregularities (imbalance) between myocardium oxygen demand insufficient coronary blood flow clinically it is manifested by removal or prevention of stenocardia attacks (improvement of disease currency) and increasing of patients’ tolerance to physical load
ANTIANGINAL (CORONARY ACTIVE) DRUGS І. Nitrates and sidnonimins ІІ. Beta-adrenoblockers ІІІ. Antagonists of calcium ions ІУ. Activators of potassium channels • Inhibitors of ACE • Platelet inhibitors and anticoagulants • Drugs with metabolic influence on myocardium
NITRATES nitroglycerin isosorbid dinitrate isosorbid-5 -mononitrate
MECHANISM OF ACTION OF NITRATES • Interaction with sulfhydryl (SH-) groups (nitrate receptors) inside cells of vascular smooth muscles • Stimulation of formation of endothelial factor of relaxation of vessels (ЕRF) – nitric oxide (NO) • Decreasing of ionized Са 2+ content • Relaxation of smooth muscles, dilation of vessels, including coronary vessels
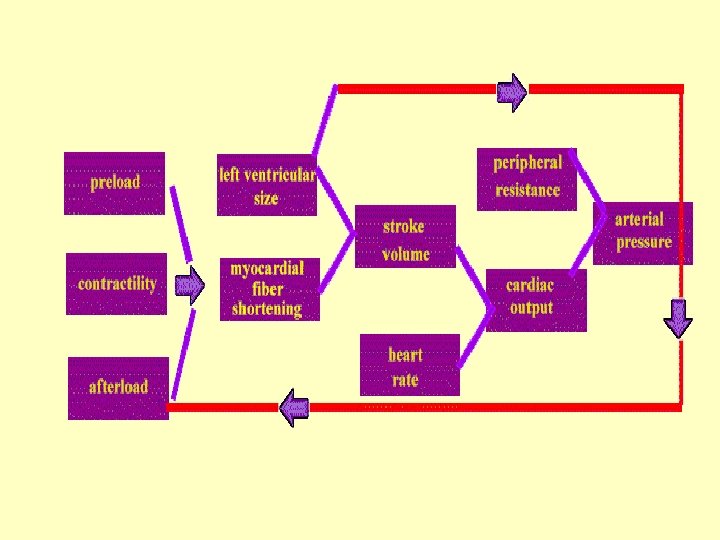
MECHANISM OF ACTION OF NITRATES • a decrease in tone of veins – a decrease of preload (venous return to the heart during diastole) – a decrease of work of left ventricle and heart output • a decrease in tone of arterioles – a decrease of afterload (a decrease of arterial pressure, end diastolic pressure in left ventricle and it’s volume, decreasing of tension of myocardium wall) • a decrease in oxygen demands of heart because of decreased heart work • improvement of blood flow in ischemic zone of myocardium – redistribution of coronary blood flow with increasing of perfusion of subendocardial areas • dilation of large coronary vessels if they are in spasm or narrowed with atherosclerotic mass • development of anastomoses between arteries in myocardium (in case of prolonged administration)
NITROGLYCERINE • • • Tablets (under the tongue) 1 % alcohol or oil solution (under the tongue) aerosol Onset - 2 -3 min Duration of action - 20 -30 min • ampoules 1 % solution – intravenously dropply 0, 01% solution • prolonged forms of nitroglycerine: trinitrolong, sustak, nitrong, ointment, plaster
NITROGLYCERIN pharmaceutical forms
NITROGLYCERIN pill bottles
Nitroglycerine transdermal system in a form of plaster
SIDE EFFECTS OF NITROGLYCERINE bursting, pulsating headache decreasing of arterial pressure (tachycardia, dizziness, collapse – postural hypotension) facial flushing, feeling of fever
Contraindications for nitroglycerine administration • Closed-angle glaucoma • increasing of intracranial pressure, insult • acute myocardium infarction (in case of presence of hypotonia and collapse)
PROLONGED FORMS OF NITROGLYCERINE • Trinitrolong – polymer films (0, 001 g or 0, 002 g of nitroglycerine) action develops immediately, lasts for 3 -5 hours • Sustac - Sustaс-mite (contains 0, 0026 g of nitroglycerine) and Sustac-forte (0, 0064 g of nitroglycerine) onset – after 10 min, maximal action – after 1 hour, duration of action – 4 -5 hours • Nitrong – microcapsule form of nitroglycerine of prolonged action onset – 30 -60 min, maximal effect - after 3 -4 hours, Duration of action - 6 -8 hours
Nitroglycerin and Premature Birth • The five-year, randomized check involved 153 women selected at the time they went into pre-term labor (at 24 to 28 weeks). • Employing nitroglycerin patches for pregnant women prolonged their pregnancy and what's new, the babies were born healthy, with less side effects than those induced by other drugs. • In Canada, about 7. 5 % of all babies are born prematurely (before 37 weeks) and 1 to 2 % are severe cases, before 34 weeks.
Iso Mak Retard 20 mg Iso Mak Retard 40 mg Isomak Retard 60 mg (isosorbid dinitrate)
Isoket Isosorbid dinitrate
SIDE EFFECTS OF NITRATES • bursting, pulsating headache • decreasing of arterial pressure (tachycardia, dizziness, collapse) • skin redness, feeling of fever • development of tolerance • nitrate dependence • withdrawal syndrome
Mechanism of tolerance to nitrates
Other nitrates Nitrosorbid – isosorbid dinitrate onset - 30 -50 min, duration of action – 4 -6 hours and more With sublingual administration of the drug onset decreases to 3 -5 min • buccal form (Dinitrolslrbilong) • tablets of prolonged action (Isoket-retard) • ointment • aerosol • drugs for intravenous introduction Isosorbid-5 -mononitrate - pharmacologically active metabolite of isosorbid dinitrate duration of action - from 6 till 24 hours
SYDNONIMINS Molsydomin – corvaton - sydnopharm • is metabolized by the liver forming a substance – SIN-1 a which contains free NО group (doesn’t need previous interaction with SH-groups) • nitric oxide stimulates guanylatecyclase that activates synthesis of c. GMP • c. GMP causes dilation of vessels 2 mg of molsydomin = 0, 5 mg of nitroglycerine
Molsidomine metabolism
Molsidomine • onset - 20 min (5 -10 min – if administered sublingually), duration of action - 6 hours • can be used for prophylaxis and treatment angina attacks in patients with glaucoma (doesn’t increase intraocular pressure) • indicated for patients which have to discontinue of nitrates administration (“nitrate-free interval”) to restore sensitivity to them • doesn’t lead to development of tolerance (doesn’t require previous conjunction with SH-groups) • absence of withdrawal syndrome
BETA-ADRENOBLOCKERS Mechanism of action during stenocardia • blockade of 1 -adrenoreceptors of heart: decrease of cardiac output and frequency of heart contractions and as follows cardiac need in oxygen • decreasing of platelets aggregation and prevention of plug formation • increasing duration of diastole – improvement of coronary vessels saturation with blood – improvement of perfusion of ischemic areas of myocardium • Decreasing of calcium ions accumulation – releasing of cardiac muscle tension, improvement of metabolic processes, increasing of ATP synthesis • in case of acute myocardium infarction – increasing of blood supply of ischemic areas of heart, decreasing of size of infarction area, prevention of development of cardiac arrhythmias
Beta-adrenoblockers
Anaprilin β 1 - β 2 adrenoblocker
Vasocardin 100 mg Methoprolol tartrate
Nadolol ( β 1, β 2 - adrenoblocker )
CALCIUM IONS ANTAGONISTS 1. Derivatives of difenilalkilamin (verapamil) 2. Derivatives of benzothiazepine (dylthiazem) 3. Derivatives of dyhydropyridine (nifedipin, amlodipin, nimodipin) Drugs of 1 and 2 groups dominantly influence on heart (depress automatism of sinus node, slow cardiac conduction, decrease heart rate and oxygen demand), show antiarrhythmic, antianginal and hypotensive action Derivatives of dyhydropyridine (group of nifedipin) – decrease blood pressure and cause dilation of coronary vessels, cause reflective tachycardia
Nifedipin - corinfar - fenigidin adalate Doesn’t depress cardiac conduction has a weak antiarrhythmic action Maximal concentration of the drug in blood occurs after 45 -60 min after administration orally and after 2 -3 min – if administered sublingually Effect lasts for 4 -6 hours
Antagonists of calcium ions – derivatives of dyhydropyridine of ІІ generation (amlodipin, amlodipin isradipin, nicardipin) • don’t cause tachycardia • are indicated for prolonged treatment of patients with stabile angina • aren’t indicated in case of non stabile angina (long onset)
Usage of calcium ions antagonists Drugs Illness Hypertension Verapamil Dylthiazem Nifedipin Stenocardia Verapamil Dylthiazem Nifedipin Verapamil Dylthiazem Supraventric ular tachyarrhythmia Possible combination with β-blockers -recommended drug Dylthiazem Nifedipin Felodipin Amlodipin Felodipin --should be used carefully Amlodipin
Nifedipin (Са 2+ ions antagonist of dyhydropyrydine group)
Nifedipin (Са 2+ ions antagonist of dyhydropyrydine group)
Nifedipin (Са 2+ ions antagonist of dyhydropyrydine group)
AMLODIPIN
ACTIVATORS OF POTASSIUM CANALS NICORANDIL • activates Са 2+-depending potassium canals • causes relaxation of smooth muscles of vessels – coronary, arteriolar and venous vasodilatation • improves of blood supply of myocardium, decreasing of pre- and afterloads of heart, decreasing of myocardial need in oxygen, of ischemic damage zone
Acetylsalicylic acid • 80 -100 mg per day – against platelets aggregation, decreases risk of development of acute myocardium infarction and decreases mortality of patients with IHD • Throughout the world it is also used as a drug for basic treatment of IHD (can be used for years)
ACUTE MYOCARDIUM INFARCTION • one of the main reasons of disablement and mortality of people of employed age in many world countries, including Ukraine • men suffer from MI almost 5 times more often than women • Mortality of patients with MI during first two hours after beginning of the process makes around 50 % of all mortal cases connected with MI • the most often death causes – acute cardiac-vascular insufficiency (angina pectoris, lung edema, cardiogenic shock), heart rupture, severe cardiac arrhythmias • other complications of MI – thrombosis and emboli, acute and chronic heart aneurisms, Dressler’s syndrome, chronic cardiac insufficiency
ACUTE MYOCARDIUM INFARCTION From a 45 -year-old man who died of an acute myocardial infarction. Postmorten serum Cholesterol 200 mg/d. L.
TREATMENT OF MYOCARDIUM INFARCTION three stages • Immediate treatment – decreasing pain and treatment of cardiac arrest • Early treatment – separation of zone of infarction seat and prevention of early life threatening complications (cardiac arrhythmias, acute cardiac insufficiency) • Further treatment – prevention and therapy of late complications of MI, prophylaxis of recurrent MI and death of the patients
TREATMENT OF ACUTE MYOCARDIUM INFARCTION Releasing of pain and prophylaxis of cardiogenic shock • nitroglycerin (1 tablet under the tongue every 7 -10 min. ) • Neuroleptanalgesia (fentanil with droperidol), morphine, omnopon, promedol (in combination with atropine, dimedrol, aminasine) • Nitrous Oxide in combination with neuroleptics • in case of remaining pain – non narcotic analgesics in combination with antihistamine and neuroleptic drugs • to increase arterial pressure during cardiogenic shock – intravenously dropply dopamine (drugs of choice), noradrenalin, mesaton • sometimes glucocorticosteroids are used
TREATMENT OF ACUTE MYOCARDIUM INFARCTION Size limitation of infarction zone • Intravenous dropply introduction of 0, 01 % nitroglycerin solution • Administration of -adrenoblockers
TREATMENT OF ACUTE MYOCARDIUM INFARCTION Treatment and prophylaxis of cardiac arrhythmias Treatment of ventricular arrhythmias – i. v. slowly 0, 2 % solution of xycain, novocainamid intramuscularly • Prophylaxis of ventricular extrasystolia and tachycardia – magnesium sulfate (intravenous dropping introduction of 4 -5 % solution), -adrenoblockers • Arrhythmias of atrial origin – cardiac glycosides, antagonists of calcium ions • Bradycardia - isadrin, atropine sulfate, alupent (i. v. )
TREATMENT OF ACUTE MYOCARDIUM INFARCTION CORRECTION OF BLOOD CLOTTING • thrombolytic drugs streptokinase (1, 5 mln OD), urokinase (2 mln OD), aktilise – recombinant tissue activator of plasminogen (100 mg) intravenously • after performing of thrombolytic therapy – intravenous introduction of heparin, at first 10 000 OD, after 1000 OD per hour during 24 -48 hours • anticoagulants of indirect action • acetylsalicylic acid (80 -100 -300 mg per day)
TREATMENT OF ACUTE MYOCARDIUM INFARCTION Treatment of cardiac insufficiency • i. v. furosemid (40 -120 mg); i. v. dropply nitroglycerine (12 -20 hours), morphine • i. v. dropply dopamin and dobutamin • heart glycosides – in tachysystolic form of scintillating arrhythmia or fluttering of atria with moderate leftventricular insufficiency General measures • oxygen inhalation • correction of acid-base balance