ALK e meccanismi di resistenza Lucio Crin S




![[TITLE] Presented By Fabrice Barlesi, MD, Ph. D at 2013 ASCO Annual Meeting](https://slidetodoc.com/presentation_image_h2/c56622bdf8ca15c11ab6d870be73b923/image-5.jpg "[TITLE] Presented By Fabrice Barlesi, MD, Ph. D at 2013 ASCO Annual Meeting")




")

 • • 65% (22/34) objective response rate (95%")


 patients")
 at baseline Previously")

 by presence or absence of brain metastases (BM) at baseline")







 Felip, et al. ESMO")







- Slides: 35
ALK e meccanismi di resistenza Lucio Crinò S. C. di Oncologia Medica Azienda Ospedaliera di Perugia
Outline • Current evidence with ALK-TKIs in naïve patients • ALK-TKIs in crizotinib-refractory disease • Challenging brain mets in ALK+ disease • Resistance to crizotinib: focus on ‘unknown’ mechanisms
Outline • Current evidence with ALK-TKIs in naïve patients • ALK-TKIs in crizotinib-refractory disease • Challenging brain mets in ALK+ disease • Resistance to crizotinib: focus on ‘unknown’ mechanisms
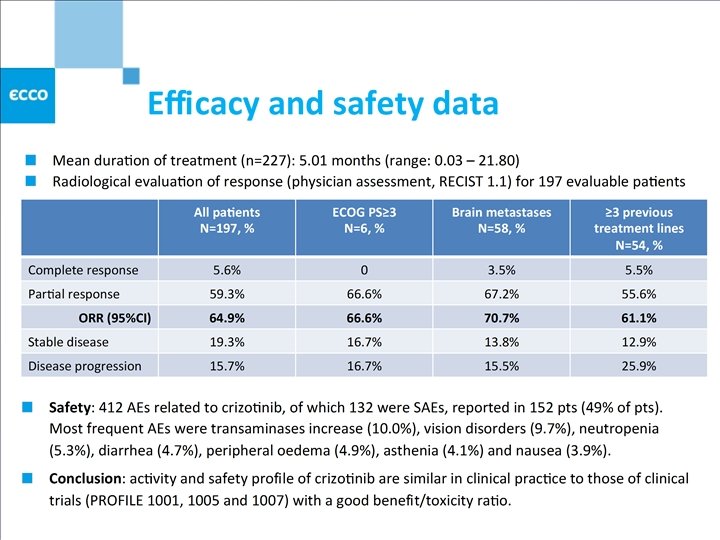
Crizotinib for ALK+ advanced NSCLC: RR appr. 60%, PFS 7. 7 -9. 7 mos Study No. of patients RR (%) PFS (mos. ) A 8081001 143 60. 8 9. 7 A 8081005 261 59. 8∞ 8. 1 A 8081007 173 65* 7. 7 French Temporary Authorization for use of Crizotinib 230 56. 5 Not reported ∞ 259 pts evaluable for response *Independent radiologic review Camidge, et al. Lancet Oncol 2012 Kim, et al. ASCO 2012 Shaw, et al. NEJM 2013 Perol, et al. ECCO 2013
[TITLE] Presented By Fabrice Barlesi, MD, Ph. D at 2013 ASCO Annual Meeting
2 nd generation ALK-inhibitors in clinical development Drug Inhibition of secondary L 1196 M ‘gatekeeper’ mutation Company Clinical stage AP-26113 Yes Ariad Pharmaceuticals Phase I/II LDK 378 Yes Novartis Phase II/III Alectinib Yes Chugai Pharmaceuticals Phase I/II TSR-011 Yes Tesaro Phase I NMS-E 628 Yes Nerviano Medical Phase I ASP-3026 Yes Astellas Phase I X-376 and -396 Yes Xcovery Phase I CEP-28122 Yes Cephalon Preclinical
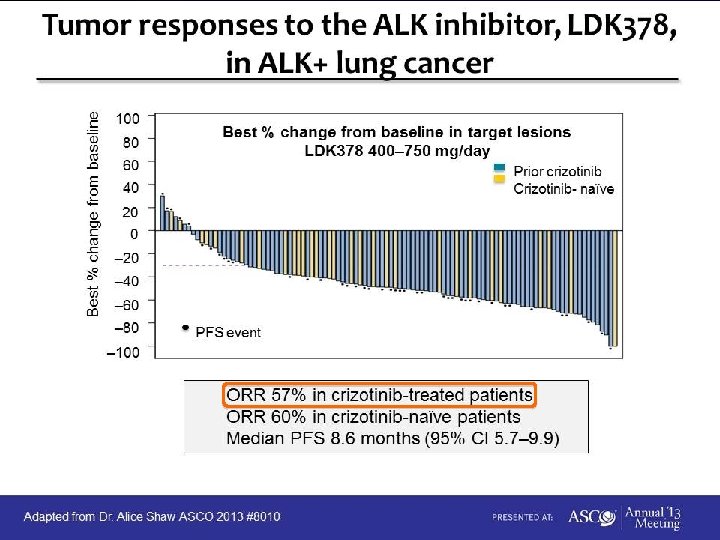
RR with 2 nd generation ALK-inhibitors in Crizotinib-naïve patients Author Drug No. of pts RR (%) Camidge (ECCO 2013) AP 26113* 3 100 Shaw (ASCO 2013) LDK 378** 35 60 Seto (Lancet Oncol 2013) Alectinib*** 46 93. 5 *60 -300 mg/d **400 -750 mg/d ***300 mg x 2/d; Asiatic (Japanese) patients
Outline • Current evidence with ALK-TKIs in naïve patients • ALK-TKIs in crizotinib-refractory disease • Challenging brain mets in ALK+ disease • Resistance to crizotinib: focus on ‘unknown’ mechanisms
CHEMOTHERAPY TKI beyond PD or 2 nd generation TKI ± local therapy TKI beyond PD + brain RT
Chemotherapy +/- ongoing crizotinib for acquired resistance in ALK-positive NSCLC SWOG 1300 (in development) PI: Ross Camidge ALK rearrangement Progression on Crizotinib after response or SD > 3 mo No prior pemetrexed N=114 Co-primary endpoint: progression-free survival Respnse rate, pemetrexed alone R A N D O M I Z E Pemetrexed alone Pemetrexed + ongoing Crizotinib
Crizotinib beyond progression Ou, et al. IASLC 2013
AP 26113 in ALK+ NSCLCs (N=34) • • 65% (22/34) objective response rate (95% CI: 47 -80%) • 61% (19/31) post-crizotinib (incl. 1 criz intolerant) • 100% (3/3) in TKI-naïve (incl. 1 CR) Response duration 8+ to 40+ weeks • 14 confirmed, 4 awaiting confirmation, 4 not confirmed 13 All patients received prior crizotinib unless otherwise indicated; Doses ranged from 60 -240 mg/d (23 pts ≥ 180 mg/d); a. TKI-naïve; b. Received prior crizotinib and LDK 378; c. PD by RECIST 1. 1 due to 2 nd primary tumor of melanoma; d. Crizotinib-intolerant of 6 Sept 2013 Camidge, et. Data al. as IASLC
Alectinib in crizotinib-refractory patients Overall RR 54. 5% across all cohorts for all patients Waterfall plot % tumor shrinkage Duration on study Days on study (*: off study, data cut-off Sept. 12, 2013) ** * * ** ** * * Overall RR 59. 5% for cohorts of 460 mg dose or higher 24 of the 47 patients received the drug for 120 days or longer Gadgeel, et al. IASLC 2013
Outline • Current evidence with ALK-TKIs in naïve patients • ALK-TKIs in crizotinib-refractory disease • Challenging brain mets in ALK+ disease • Resistance to crizotinib: focus on ‘unknown’ mechanisms
The problem of CNS progression to Crizotinib in ALK+ patients • 13/28 (46%) patients at U. of Colorado with first progression in CNS - 2/13 had synchronous systemic progression Weickardt et al. JTO 2013 • Decreased CSF: plasma (0. 0026) ratio suggestive of pharmacological failure of Crizotinib Costa et al. JCO 2011
Crizotinib antitumour activity in patients with or without brain metastasis (BM) at baseline Previously untreated for BM (n=109) n Outcome Previously treated for BM (n=166) n Outcome No BM detected (n=613) n Outcome DCR at 12 weeks, % (95%CI) IC 109 56 (46− 66) 166 62 (54− 70) NA Systemic 109 63 (54− 72) 166 65 (57− 72) 109 7 (3− 14) 166 7 (4− 12) NA 22 18 (5− 40) 18 33 (13− 59) NA 109 53 (43− 63) 166 46 (39− 54) 613 71 (68− 75) ORR, % (95% CI) IC Target-lesion BM Systemic 613 55 (51− 59) Median time to tumor response (range), a weeks IC Systemic 8 6. 0 (4. 9− 12. 4) 12 6. 4 (5. 9− 17. 7) NA 58 6. 1 (2. 0− 31. 4) 77 6. 1 (3. 1− 35. 3) 8 26. 4 (6. 1− 59. 3) 12 NR (6. 0− 59. 9) 58 47. 9 (5. 3− 55. 0) 77 55. 6 (4. 4− 95. 3) 336 49. 0 (4. 1− 96. 1) 109 8. 3 (6. 7− 14. 0) 166 13. 5 (6. 2− 16. 5) 613 9. 9 (8. 8− 12. 2) 336 6. 1 (3. 0− 49. 1) Median duration of response b (range), a weeks IC Systemic Median systemic PFS, b (95% CI), c mo NR, not reached a. In patients with confirmed objective response; b. Kaplan−Meier method; c. Brookmeyer−Crowley method NA Costa, et al. IASLC 2013
Example of a complete response of a brain lesion in response to crizotinib treatment Before initiation of crizotinib 6 weeks after crizotinib 250 mg BID This patient presented with a brain lesion previously treated with chemotherapy and palliative IC radiation, which was classified as a target lesion. A CR in this lesion was observed after 6 weeks of treatment and had persisted for 54 weeks by data cutoff (courtesy of J-Y Han, National Cancer Center, Goyang, South Korea)
Systemic progression-free survival (PFS) by presence or absence of brain metastases (BM) at baseline (BL) The presence of BM at BL does not significantly affect systemic PFS to crizotinib Costa, et al. IASLC 2013
CNS activity of alectinib • ORR of the 21 patients as determined by central image review CR PR SD PD Total N=21 6 5 8 2 % 29% 24% 38% 10% • 9/21 patients with baseline CNS metastasis had measurable CNS lesions and received no prior radiation within 4 weeks from first dose of alectinib – No CR. 5/9 achieved CNS PR (≥ 30% reduction in sum of largest dimension). 2/9 had CNS stable disease and 2/9 had CNS progression. 0, 60 PR 0, 40 0, 20 0, 00 Brain RT > 4 wks 91+ 203+ No brain RT 42 -0, 20 -0, 40 224+ 287+ 224+ -0, 60 98+ 196+ 294+ -0, 80 Progressing CNS mets Days on study Ou, et al. IASLC 2013
Outline • Current evidence with ALK-TKIs in naïve patients • ALK-TKIs in crizotinib-refractory disease • Challenging brain mets in ALK+ disease • Resistance to crizotinib: focus on ‘unknown’ mechanisms
Unraveling the mechanisms of resistance to EGFR-TKIs and Crizotinib Amp lified Unknown ALK amp ALK+ No ALK amp or mut ALK mut M 96 1 L 1 G 1269 A S 1206 Y G 1202 R 115 L 11 1 Tins C 1 52 R 15 6 Y Bypass tracks EGFR MT KRAS MT Katayama, et al. Sci Trans Med. 2012 Doebele, et al. Clin Cancer Res. 2012
IGF-1 R and IRS-1 are up-regulated in ALK TKI resistant cells p. ALK Y 1604 ALK p. IGF-1 R Y 1131 IGF-1 R p. AKT S 473 AKT p. S 6 p. ERK IRS-1 p. Y 941 References: Lovly, C et al 2011 Cancer Research and Lovly, C et al submitted IRS-1 00 50 M SO TKI resistant D 00 50 ALK TKI [n. M] M SO TKI sensitive D Generation of isogenic pairs of ALK TKI sensitive and ALK TKI resistant cells
p. IGF-1 Rand and. IRS-1 are areup-regulatedininpatientbiopsysamplesatat thetimeof ofacquiredresistanceto tocrizotinib Reference: Lovly, C et al submitted
IGF-1 R inhibitors sensitize H 3122 ALK TKI resistant cells to the anti-proliferative effects of ALK inhibitors Key: - X-376: ALK TKI - MAb 391: IGF-1 R MAb - Soft agar assay in H 3122 X-376 resistant cells Similar results seen in H 3122 crizotinib resistant cells Analogous results seen with IGF-1 R TKIs in addition to IGF-1 R MAbs Reference: Lovly, C et al submitted
Rationale for double ALK/HSP 90 inhibition in ALK+ advanced NSCLC From Crystal and Shaw, Clin Cancer Res 2012
Hsp 90 inhibitor AUY 922: activity in ALK+ patients (n=19/22) Felip, et al. ESMO 2012
The Hsp 90 i AT 13387 overcomes acquired resistance to crizotinib H 2228 R tumor xenografts treated with AT 13387 Tumor #6 transplanted • AT 13387 treatment inhibits the growth of an ALK-dependent tumor xenograft with acquired resistance to crizotinib Wallis, IASLC 2013
Rationale for the upfront use of combination regimens Therapy Resistance Selection for resistance Selection for genetic instability ALK: (e. g. ALK-TKI + Hsp 90 inhibitor; ALK-TKI + IGFR-1 R inhibitors )
Preclinical evidence for UPFRONT dual ALK/Hsp 90 inhibition: ALK-TKI + Ganetespib Sang et al. Cancer Discov 2013
Preclinical evidence for UPFRONT dual ALK/Hsp 90 inhibition: ALK-TKI + AT 13387 • • Combination of AT 13387 and crizotinib shows improved inhibition of tumor growth over monotherapies Combining crizotinib upfront with AT 13387 delays the emergence of resistance in vivo Wallis, IASLC 2013
Clinical attempt to better Crizotinib: trials of ALK/HSP 90 inhibition Regimen Phase Clinical. Trials. gov Identifier Crizotinib + AT 13387 I/II NCT 01712217 Crizotinib + Ganetespib I/II NCT 01579994 LDK 378 + AUY 922 Ib NCT 01772797
ALK-inhibition in ALK+ NSCLC • Platform networks required tools for optimization of NSCLC treatment • 2 nd generation ALK-TKIs may break the boundary of 60% response rate observed with Crizotinib • Appr. 60% of RR with 2 nd generation ALK-TKIs in Crizotinibrefractory patients • 2 nd generation ALK-TKIs may prevent CNS pharmacological failure • Hsp 90 activity and IGF-1 R upregulation may be partly responsible for the non-ALK dominant mechanisms of resistance to crizotinib • Robust preclinical evidence of anticancer efficacy with ALKTKIs + HSP 90 or IGF-1 R inhibitors in ALK+ advanced NSCLC
Thanks for your attention lucio. crino@ospedale. perugia. it