2 Fluid Management in Dengue Hemorrhagic Fever Dengue





")









+ 9/2 • 1 -7 years :")















- Slides: 39
2. Fluid Management in Dengue Hemorrhagic Fever Dengue Expert Advisory Group
Dengue Virus Infection • Asymptomatic • Symptomatic – Undifferentiated Febrile Illness – Dengue Fever – Dengue Hemorrhagic Fever Non Shock
Dengue Hemorrhagic Fever • Febrile Phase • Critical phase characterized by plasma leak • Convalescent Phase
Dengue “Leak” Fever • Plasma leak during critical phase is the hall mark • Leading to 3 rd space losses – peritoneal cavity – pleural cavity • Variable in magnitude and exact timing
Pathogenesis of leak • Infection with a virulent dengue virus • Presence of antibodies that enhance dengue virus infection (ADE) • Intense immune activation
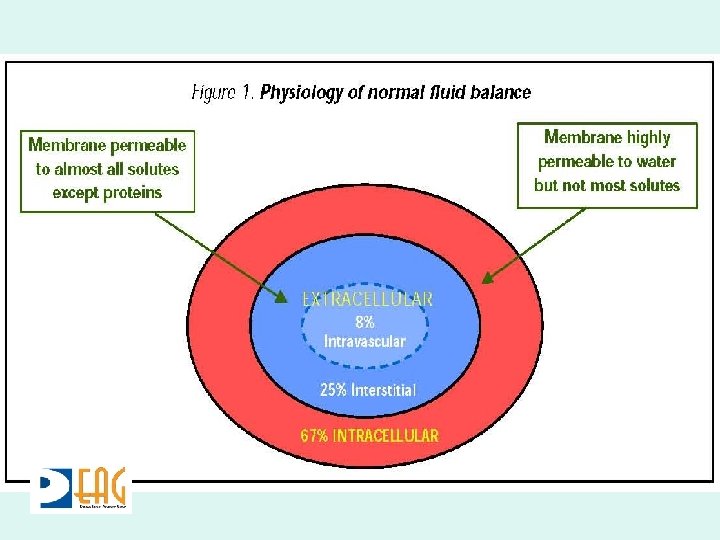
Pathogenesis • Rapidly elevated cytokines (TNF-a, IL-2, IL -6, IL-8, IL-10, IL-12, and IFN-g) • Malfunction of vascular endothelial cells • Plasma leakage from intra to extravascular space
Pathogenesis • In severe DHF the loss of plasma is critical • Patient becomes hypovolaemic • Signs of circulatory compromise • Progress to shock, organ failure, death
Pathogenesis • Cytokine Storm • Self limited • Ends after 48 hours
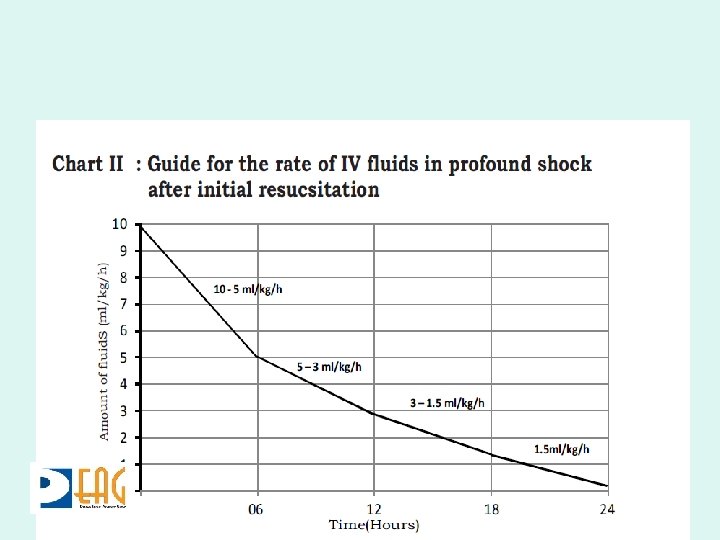
Clinical Implications • Extravascular fluid loss at variable rate that has to be matched ml for ml • Lasting 48 hours • Resorption of fluid during convalescent phase
Key Points • Manage critical phase with appropriate volume – Don’t under transfuse – Don’t over transfuse • Meticulous monitoring during critical phase to match rate of fluid infusion with rate of leak
Monitoring Parameters • Clinical – Pulse Rate – Blood and Pulse Pressure – Capillary Refill Time – Urinary Output • Lab – Hematocrit
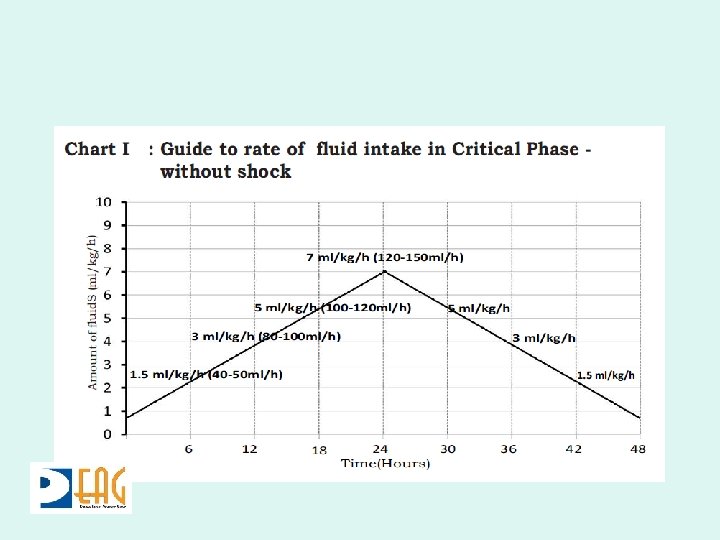
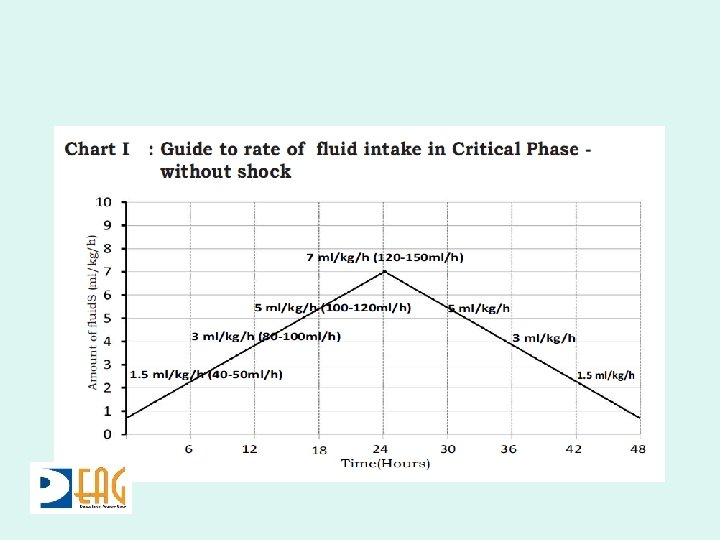
Fluid Management Critical Phase
Amount of Fluid? • Based on weight • Adults – If less than 50 kg use actual weight – If more take weight as 50 kg • Paediatrics – Current OR Ideal body weight whichever is lower
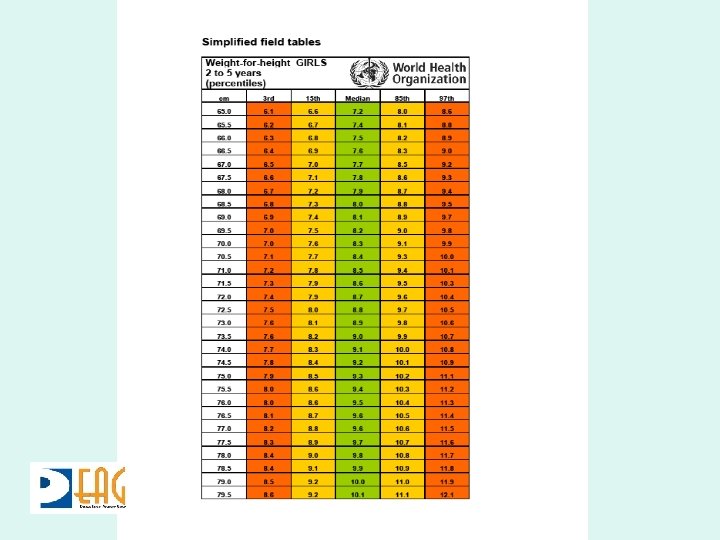
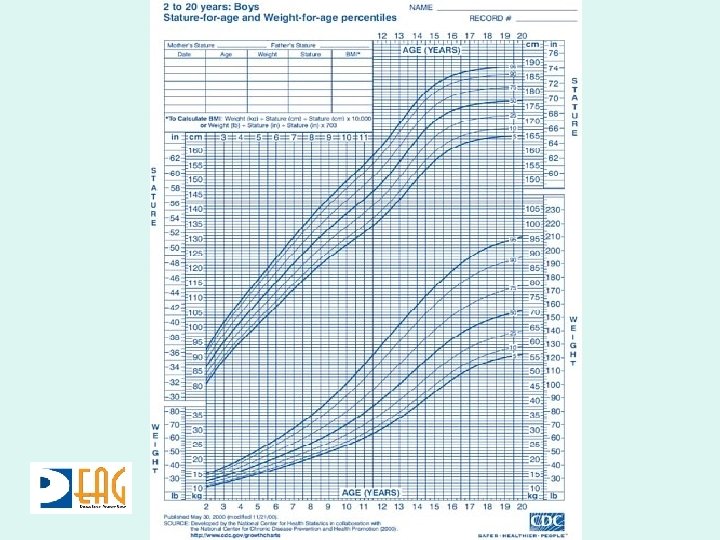
Ideal Body Weight • Weight for height using a growth chart • Weight for age • Formulae in emergency
Growth Charts
Formulae • <1 year : Age (in Months)+ 9/2 • 1 -7 years : (Age x 2)+ 8 • >7 years : • APLS : (Age in years + 4) x 2 Age x 3
Fluid Quota • M + 5% = Maintenance + 5% of body weight • Over 48 hours if patient presents in the beginning of critical phase (without shock) • Over 24 hours for patients coming in shock
M + 5% - Adults • Maintenance – 1 st 10 kg – 1000 mls – 2 nd 10 kg – 500 mls – Remaining 30 kgs – 600 mls – Sum = 2100 mls • 5% deficit – 50 x 50 = 2500 mls • Total = 4600 mls
Child 22 kg • Maintenance – 1000 + 500 + 40 = 1540 mls • 5% Deficit – 50 x 22 = 1100 mls • Total 2640 mls
Types of Fluid • Crystalloids – 0. 9% Saline – 5%Dextrose 0. 9% Saline – 5% Dextrose ½ saline
Monitoring – Critical Phase • Vital parameters - hourly • Fluid balance chart - assess three hourly • HCT - six hourly
Fluid Management in Dengue Shock Syndrome
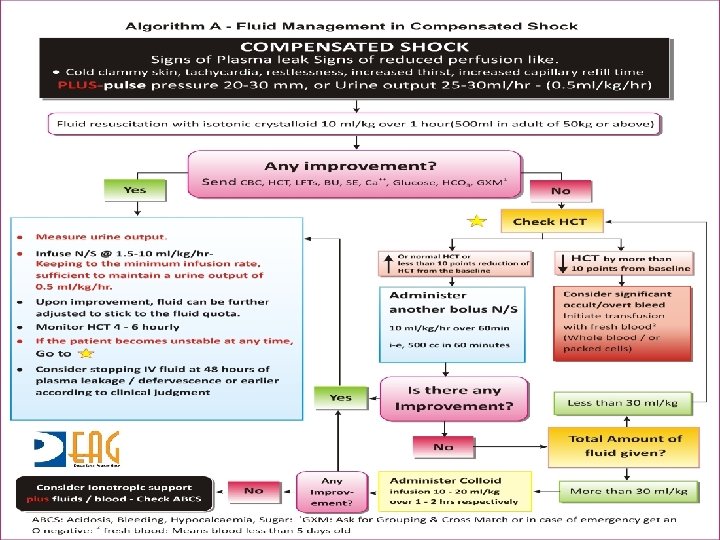
Compensated • Body compensates for fluid loss • • Tachycardia Pulse Pressure narrows Prolonged CRT Fall in urine output to 0. 5 mls/kg/hr
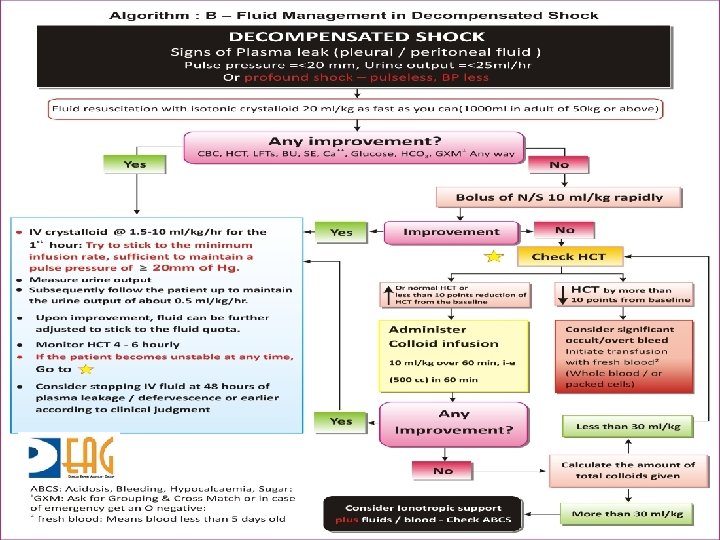
Decompensated • Pulse pressure narrows further leading to unrecordable pulse and BP • Urine output falls less than 0. 5 mls/kg/hour • Supply to myocardium and brain compromised
Fluid Resuscitation • Crystalloids – N Saline • Colloids – Dextran 40 in saline – 6% Starch • All boluses part of fluid quota
Indications for Colloid • Failure of crystalloid boluses to normalize pulse /BP • Development of shock – with fluid overload – amount of fluid exceeding M + 5% deficit • 10 ml/kg over 1 hour
Colloids • Dextran may sometimes interfere with grouping and cross matching • 3 doses of Dextran 40 during a 24 hour • 5 doses of 6% Starch during 24 hour • Remain in circulation for much longer
Refractory Shock - ABCS • Blood – packed cells – whole blood • Bicarbonate • Glucose • Calcium
Monitoring During Shock • 15 minute monitoring of vital signs • HCT immediately before and after each fluid bolus and then at least two to four hourly
Key Points – Managing DHF • Recognizing the start of critical phase of DHF • Predicting the rate of leak which may vary from patient to patient and within the same patient • Matching the rate of infusion to rate of leak • Being cognizant of the end of critical
Key Points – Managing DSS • Meticulous monitoring • Switching appropriately from crystalloids to colloids • Recognizing need for blood transfusion