The Radial Approach for CTO PCI Utility in



 Sometimes TRI with retrograde approach can make possible what seems to")





























 Endeavor 3.")














 First-time PCI attempt")


 Bidirectional approach P<0. 001")
 TFI (n=223) 0 (0%) 6 (2. 7%)")

- Slides: 55
The Radial Approach for CTO PCI Utility in the Retrograde and the Antegrade Approaches Shigeru Saito, MD, FACC, FSCAI, FJCC Shonan Kamakura General Hospital
Shigeru Saito, MD I have no real or apparent conflicts of interest to report.
PCI for a CTO still remains the greatest challenge to the interventional cardiologist • Increased procedural complexity and complications • Low procedural success rate The most important point during PCI for CTO lesions is: To perform PCI successfully without causing the patients to have a worse clinical conditions than before.
Trans-radial intervention (TRI) Sometimes TRI with retrograde approach can make possible what seems to be impossible to treat by PCI.
The Case in which femoral access is limited ü Old CTO ü CRF on hemodialysis ü Leriche syndrome ü Poor LV function (EF 38%) ü Functional Severe Mitral Regurgitation ü Refused surgical treatment by the cardiac surgeons ü Failed at the previous hospital
A 71 -year-old man • Chief complaint: Chest pain on effort • History: December of 2009: Chest pain #2 99%, #3 total, #12 75% PCI for #12 75% (Vision 3. 0 x 12) August of 2010: Chest pain on effort PCI via the rt. radial artery for a #3 CTO (failed) → referred to our hospital • Risk factors: HT, Former smoker (1 P/day for 21 years) • Past history: • 1995~ Hemodialysis for CRF (CGN)
RCA
Occluded lesion Collateral from the LAD RCA
Occluded abdominal aorta Abdominal aorta occlusion
Shunt for hemodialysis 6 F SAL for RCA 6 F EBU for LCA Occluded abd aorta
Angio RCA ostial 90% mid Total
Angio LCA Retrograde Via the Rt. radial 6 F EBU 3. 5
Selection of the Septal Channel
Retrograde Corsair + Fielder FC
Retrograde Corsair + Fielder FC
Retrograde Corsair + Fielder FC
Retrograde Corsair + Fielder FC
Retrograde FINECROSS +ULTIMATE bros 3 ↓ + Wizard 3 Crossed into the Aorta cusp
Retrograde FINECROSS +ULTIMATE bros 3 ↓ + Wizard 3 Crossed into the Aorta cusp
Antegrade Via the Rt. brachial 6 F SAL 1. 0 SH FINECROSS + Runthrough HC ↓ Not cross #2
Antegrade Anchoring at #1 by a Tazuna OTW 3. 0 mm oring h c n A Retrograde We repeated a dilatation at the occlusion site using a Tazuna 1. 25
r Ancho ing
ring o h c An
A or h c n ing
Antegrade Anchoring at #1 by a Tazuna OTW 3. 0 mm + X-treme ↓ Conquest Pro ↓ Wizard 3 Crossed into #4 PL g rin o ch W iz ar d 3 An
Antegrade Tazuna 1. 25 Retrograde Anchoring at #3 by a Tazuna OTW 3. 0 mm Anchoring
Antegrade Tazuna 1. 25 Retrograde Anchoring at #3 by a Tazuna OTW 3. 0 mm Anchoring
Antegrade Tazuna 1. 25 Retrograde Anchoring at #3 by a Tazuna OTW 3. 0 mm Anchoring
Antegrade Tazuna 2. 5 x 15 Retrograde Anchoring at #3 by a Tazuna OTW 3. 0 mm Anchoring
Antegrade Tazuna 2. 5 x 15 Retrograde Anchoring at #3 by a Tazuna OTW 3. 0 mm Anchoring
Antegrade Tazuna 2. 5 x 15 Retrograde Anchoring at #3 by a Tazuna OTW 3. 0 mm Anchoring
Antegrade mother-child technique of 4 -in-6 (4. 5 F ASAHI Co. Katte) Endeavor 3. 0 x 30
Cypher 3. 5 x 13 End eav or 3. 0 x 3 0 18 x 0 3. or v ea d En 0 x 3 3. 0 or av de En 3. 0 x 24 Endeavor
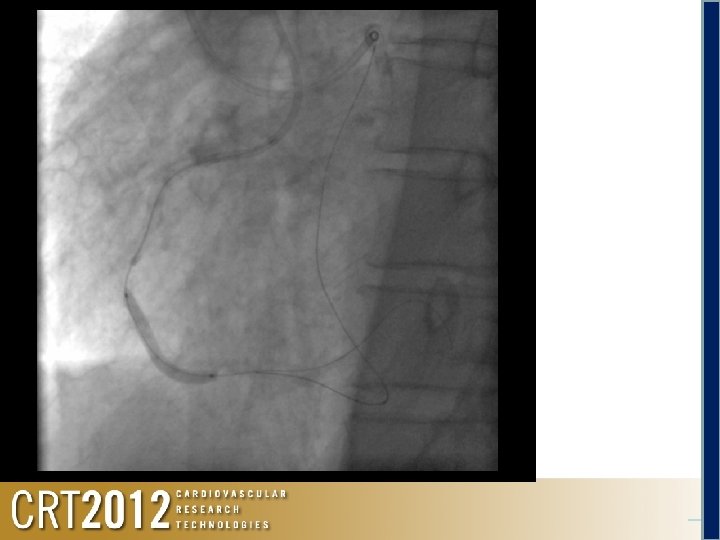
Final angiogram
Final angiogram Procedure time 175 min Fluoro time 72. 8 min Contrast media 300 ml
ü Because of a severe calcified lesion, catheter procedure was difficult, but the CTO lesion was ultimately opened. ü This case was challenging in that no mechanical devices for hemodynamic support were available to use because of bifemoral occlusions and even only one complication could have become very serious and potentially fatal. ü We performed a PCI for the CTO with a bidirectional approach via the ipsilateral radial and brachial arteries due to necessity.
Various Procedure Techniques for CTO Angioplasty • • Double guidewire technique Side branch technique Anchoring balloon technique Use of Tornus device Mother-and-Child catheter technique Retrograde (Bi-directional) approach IVUS-guided technique
Limitation of TRI for CTO – Limited size of guiding catheter (Maximum 7 F ) Decreased backup support →Calcified lesion & Long lesion Limited device & technical selection →IVUS-guided technique not available (Side-branch IVUS & Co-axial IVUS) – Time delay if intra-aortic balloon pump or temporary pacing is needed
Recommendation in TRI for CTO Based on the understanding of the limitation of TRI and various kinds of techniques used in CTO angioplasty, we can perform TRI in various types of CTO lesions such as: • CTO with microchannels • CTO with clear distal anatomy • CTO without calcification or tortuosity • The case in which femoral access is limited
Kamakura experience • Consecutive review of 381 patients (417 CTO lesions) First-time PCI attempt for a CTO via radial or femoral access (January 2005 - August 2011) The patients on hemodialysis were excluded. • • • CTO: coronary obstruction with a TIMI flow grade 0 for 3 months. Indications for PCI for the CTO Viable myocardium by echocardiography and ventriculography. Technical success: TIMI flow grade 3 and a < 50% final residual stenosis on all views.
Results: Baseline clinical characteristics TRI group TFI group p Value Number of patients 175 206 Age, yr 68 ± 10 66 ± 10 0. 10 Male sex, n (%) 143 (81. 7) 167 (81. 1 0. 87 Height, cm 162 ± 8 165 ± 8 0. 017 BMI, kg/m 2 24. 1 ± 3. 5 24. 8 ± 3. 6 0. 19 Current smoking, n (%) 34 (19. 4) 45 (21. 8) 0. 74 Hypertension, n (%) 111 (63. 4) 131 (63. 6) 0. 84 Hyperchoresterolemia, n (%) 117 (66. 9) 139 (67. 5) 0. 84 Diabetes mellitus, n (%) 65 (37. 1) 84 (40. 8) 0. 69 LVEF, % 58 ± 13 57 ± 12 0. 21 Prior MI in other area, n (%) 29 (16. 6) 42 (20. 4) 0. 34 Multi-vessel, n (%) 88 (50. 3) 113 (54. 9) 0. 37 Prior CABG, n (%) 4 (2. 3) 17 (8. 3) 0. 011
Target vessel 120 100 80 60 40 20 0 P<0. 001 118 75 Total Instent occlusion 73 61 58 RCA LAD 32 CX TRI 194 18 223 17 TFI
Sheath size (Antegrade) Bidirectional approach P<0. 001
Procedure complications Bleeding requiring transfusion TRI (n=194) TFI (n=223) 0 (0%) 6 (2. 7%) 4: Access site bleeding 2: Retroperitoneal hematoma Pseudoaneurysm 0 (0%) 2 (0. 9%) Contrast-induced nephropathy 0 (0%) 3 (1. 3%) Cardiac tamponade (all wire perforation) 3 (1. 5%) 2 (0. 9%) Myocardial infarction 2: Pericardiocentesis 1: Surgical + CABG 0 (0%) 1: Pericardiocentesis 1: Surgical procedure 1 (0. 4%) 1: Coronary dissection with retrograde GC Cerebral infarction 0 (0%) Need of IABP 2 (1. 0%) 2 (0. 9%) Death 0 (0%) 1 (0. 4%) 1: Access site bleeding
With an appropriate patient/lesion selection, TRI for CTO lesions may result in more favorable short-term outcomes with acceptably high procedural success and lower complication rates. At least 35% of the total CTO lesions can be successfully recanalized by TRI. Therefore, given the correct circumstances, TRI should be considered as an appropriate first-line intervention for CTO lesions.