Surgical treatment of shoulder sports injuries Mr Lee












 Questionaire -")





















")
 20, 326 -332")

 8 -11% – Open (Bankart) 0")


 • Initially Tibia • Now iliac")









- Slides: 51
Surgical treatment of shoulder sports injuries Mr Lee Van Rensburg United Kingdom
Objectives • Surgical options for shoulder instability – Glenohumeral • Acute traumatic • Recurrent traumatic
30 YO male, Professional Rugby payer,
Surgical options
Shoulder Instability Hippocrates 400 BC • method of reduction • cauterisation of inferior capsule
Bankart Lesion • Perthes 1906 • Bankart 1938 – “essential lesion” of the capsulolabral complex Uber operation bei habitueller schulterluxation. Perthes G. Dtsch Z Chir 1906 The pathology and treatment of recurrent dislocation of the shoulder joint. Bankart B Br J Surg 1938
Bankart Repair • Bankart 1938 • 1 st procedure 1923 on his former House Surgeon • re-attaching capsule to the glenoid with transosseous sutures • repairing subscapularis with NO overlap or shortening The pathology and treatment of recurrent dislocation of the shoulder joint. Bankart A. Br J Surg 1938
Modified Open Bankart Repair • Numerous modifications - capsular imbrication - suture anchors • Multiple series published • Accepted recurrence rate Open Bankart Repair 8 – 12% • Loss of ER
Arthroscopic Stabilisation • Johnson 1982 - Arthroscopic Staple Capsulorrhaphy - Metal Staple - 106 patients - > 18 mth F/U - 21% recurrence Early complications of acute anterior dislocation of the shoulder in middle-aged and elderly patients. Johnson JR et al. Injury 1982
Staple Capsulorrhaphy Lane et al 1993 - 54 patients Staple Capsulorrhaphy - >39 month F/U - 18 (33%) re-dislocated - 36 stable – 15 % loose staple + articular injury - < 50 loss of ER - Caution in considering Staple Capsulorrhaphy - ROM & functional level well maintained Arthroscopic staple capsulorrhaphy: A long term followup. Lane JG et al. Arthroscopy 1993
Transglenoid Stabilisation • Caspari 1988 - Transglenoid arthroscopic stabilisation - multiple sutures passed through AI capsule - transglenoid drill hole - passed A to P through glenoid - sutures tied onto infraspinatus fascia Arthroscopic reconstruction for anterior shoulder instability. Caspari. Tech Orthop 1988
Transglenoid Stabilisation • Torchia 1997 - 150 transglenoid stabilisation - F/U > 2 yrs - av age 29 yrs (14 – 67) - 11 dislocations (7. 3%) - areas of risk - P fixation - < 25 yrs Arthroscopic transglenoid multiple suture repair: 2 - 8 year results in 150 patients. Torchia et al. Arthroscopy 1997
Transglenoid Stabilisation • Soderlund 2008 - 455 army recruits (1992 – 2000) Questionaire - 312 (68. 5%) responded av 20 yr (18 -28) - Av time from surg 6. 4 yrs (1 -14) - 177 (56%) re-dislocations Long-term outcome of a transglenoid suture technique for anterior shoulder instability in young adults. Soderlund et al JBJS Br 2008
Bioabsorbable Tack Stabilisation • Bioabsorbable Tack Stabilisation Speer 1996 - 52 recurrent dislocators - Suretac stabilisation - > 2 yr F/U (24 – 60 mth) - 11 dislocations (21%) - 7 of 8 open revision Bankart healed with ‘patulous capsule’ An arthroscopic technique for anterior shoulder stabilisation of the shoulder using a bio-absorbable tack. Speer et al. J BJS Am. 1996
Arthroscopic Stabilisation • Suture Anchor Stabilisation - problems staple & transglenoid fixation - difficulty in capsule plication with tacks - improvements in suture anchor design - improvements in instrumentation
Arthroscopic washout Arthroscopic Stabilisation v Arthroscopic Lavage • 2 yr f/u (1 lavage & 3 stabilisation – lost) - Re-dislocation - stab - lavage 3/42 ( 7%) 16/42 (38%) - Reduction in risk - 76% re-disc & 82% instab Primary arthroscopic stabilisation for a first-time anterior dislocation of the shoulder. Robinson JBJS Am 2008
Suture Anchor Stabilisation • Metanalysis Hobby 2007 - 20 suture anchor stabilisation studies - 1030 patients - recurrence as end point - failure rates ranged from 0 – 30% - most < 10% Is arthroscopic surgery for chronic shoulder instability as effective as open surgery? A systematic review and metaanalysis of 62 studies including 3044 arthroscopic operations. Hobby et al. JBJS Br. 2007
Surgical options summary • Hot Poker in axilla • Open Bankart • Arthroscopic – Staple – Transglenoid suture – Suture tacks – Arthroscopic washout – Suture anchors
Again? • Age 30 continues to play what are chances it will happen again
Non-Operative Treatment Prognosis: age at time of dislocation 12 -22 yrs 23 -29 yrs 30 -40 yrs Re dislocated 73% 56% 25% x 1 disloc 20% 18% 10% no surgery 12% 10% 5% surgery 40% 28% 10% Recurrence ( > x 2) Non-operative treatment of primary anterior shoulder dislocation in patients forty years and younger. A prospective twenty-five-year followup. Hovelius et al JBJS Am 2008
Open Access Journal of Sports Medicine 2011: 2 19– 24
Diagnostic arthroscopy • Anaesthetic – GA – Regional block – www. nerveblocks. co. uk • Interscalene block • Supraclavicular +- Axillary nerve block • Setup – Beach position – Lateral position • Skin preparation – Alcohol/ chlorhexidine preparation • Propriono bacterium acnes • Prophylactic antibiotics – Implant surgery – P acnes • Flucloxacillin _+- Gentamycin
• Alcohol and chlorhexidine, superior to povidone iodine J Bone Joint Surg Am. 2009; 91: 1949 -53
Diagnostic arthroscopy • Equipment – Arthroscopy stack • 30 degree scope – Fluid management system – High flow arthroscopy trocars – Radiofrequency probe – Arthroscopic shaver – Suture passers – Anchors
Diagnostic arthroscopy • Portals – Posterior – viewing portal – Anterior- working portal (inside out, spinal needle) • Procedure – – – – – Biceps anchor Anterior labrum MGHL Subscapularis SGHL (Pulley) Biceps (tunnel) Supraspinatus Inferior recess Articular surfaces • • • Glenoid Humeral head Closure – Subcuticular prolene
Portal Placement • Anterior Portal – 2 nd 2 1 ‘working’ gleno-humeral portal
Arthroscopic Bankart
Diagnostic Arthroscopy
Suture Anchor Insertion
Knott Tying
Second Anchor
Arthroscopic stabilisation
Arthroscopic stabilisation
SLAP tears 1 Frayed 6 2 with A or P labral flap 2 Superior A and P 7 Tear into MGHL 3 2 + bucket handle 8 2 + P labrum 4 Bucket into biceps 5 Assoc dislocation 9 10 2 + Circumferential labrum 2 + P + Inf labrum
SLAP tears • Options – Debridement • Type 1 – Re attachment (SLAP repair) – Biceps tenotomy/ tenodesis
J Shoulder Elbow Surg (2011) 20, 326 -332
Again?
• Recurrence rates – Arthroscopic (suture anchor) 8 -11% – Open (Bankart) 0 -11% • Arthroscopic slightly better ROM Sports Health. 2011 Jul; 3(4): 396 -404.
Glenoid Bone Loss • Re-Dislocation - 194 arthroscopic stabilisations - 21 significant bone loss - no bone loss - inverted pear 4% recurrence 61% recurrence - “Inverted Pear” 25% of glenoid surface area Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the glenoid’s “inverted pear” and the humeral “engaging Hills-Sachs lesion”. Burkhart & De Beer Arthroscopy 2000
• Glenoid • Concavity depression • De Beer – Inverted pear • Deficiency antero inferior diameter >25% – Augment glenoid • Humeral • Hills sachs lesion • Engaging Hill Sachs lesion – Dx Arthroscopy – Address humerus J Shoulder Elbow Surg (2009) 18, 317 -328
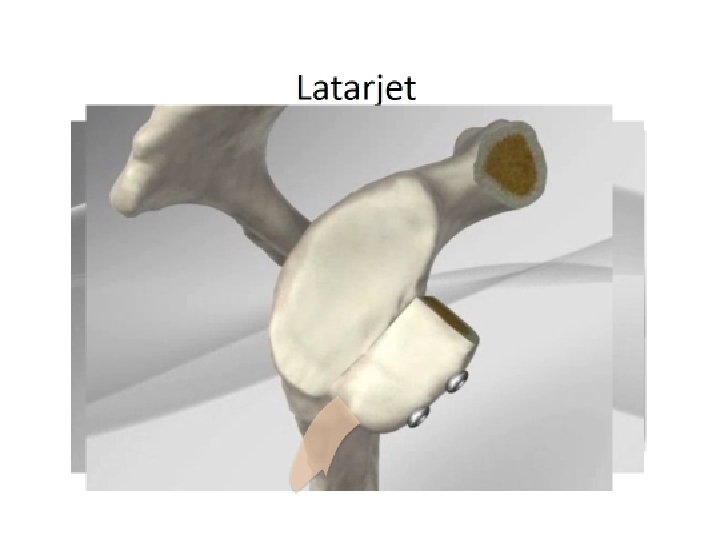
Glenoid defects • Eden Hybbinette ( 1918/ 1932) • Initially Tibia • Now iliac crest • Bristow (Helfett 1958) • 1 -2 cm Coracoid transfer distal to pectoralis minor • Single screw • Latarjet (1954) • Larger 2 -3 cm • Length ways 2 screws • Arthroscopic
Latarjet
Humeral defects • Massive Hill-Sachs lesion • >25% volume of the humeral head • Management - rotational osteotomy - hemiarthroplasty - infraspinatus transfer - osteo-articular allograft - arthroscopic remplissage
Humeral Bone Loss • Osteoarticular humeral head allograft - 18 patients failed surgery with >25% Hill-Sachs - osteoarticular allograft - 0 recurrence at 2 yrs - early x-ray evidence of allograft collapse Recurrent anterior instability following failed surgical repair: Allograft reconstruction of large humeral defects. Miniaci, Tytherleigh-Strong. JBJS 2001
Arthroscopic Remplissage • arthroscopic Bankart • capsulodesis and infraspinatus tenodesis
Summary Young sports dislocation 1 week
Bone loss - Plain x-ray - CT recon
Practically • Arthroscopic Bankart with anchors – 1 st time dislocator – Recurrent with no bony defect • Open Latarjet – Failed arthroscopic Bankart – Bony defects (glenoid) – Chronic dislocation
J Bone Joint Surg Am. 2009; 91: 966 -78
The End