Social Determinants of Health Impacts on Health Outcomes


 of any commercial product(s)")








 County Health Rankings Components Source: http: //www. countyhealthrankin gs.")














 • Routinely assess for trauma exposure and related")






 • Child •")






 • Section 2")






 • Educate staff regarding")
















 https: //picc. jhu. edu/the-toolkit. html")

 Center www. aap. org/screening")
- Slides: 70
Social Determinants of Health: Impacts on Health Outcomes, Engaging Families and Clinicians in Addressing Social Determinants & Promoting Resilience, and Creating System Level Changes to Accelerate Action
Practice Implementation and System Building for Two-Generational Care Screening for, and Addressing Social Determinants of Health and Perinatal Depression Marian F Earls, MD, MTS, FAAP Pediatric Population Health Forum Seattle, Washington June 8, 2019
Disclosures I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in this CME activity. We do not intend to discuss unapproved or investigative uses of a commercial product or device. Marian F. Earls, MD, MTS, FAAP
Today’s Objectives At the completion of this activity the learner will be able to: • Understand the impact of Social Determinants of Health, ACEs and perinatal depression on the health of the child and family. • Engage families with screening as conversation, and as partners in care. • Implement screening, primary care intervention, and processes for linking families with resources. • Implement outreach to build collaborative relationships with community partners.
What We Know • Impact of experience on brain development. • Growth, development, and behavior are inextricably linked. • Emotional development occurs in the context of a relationship (bonding, attachment, reading cues).
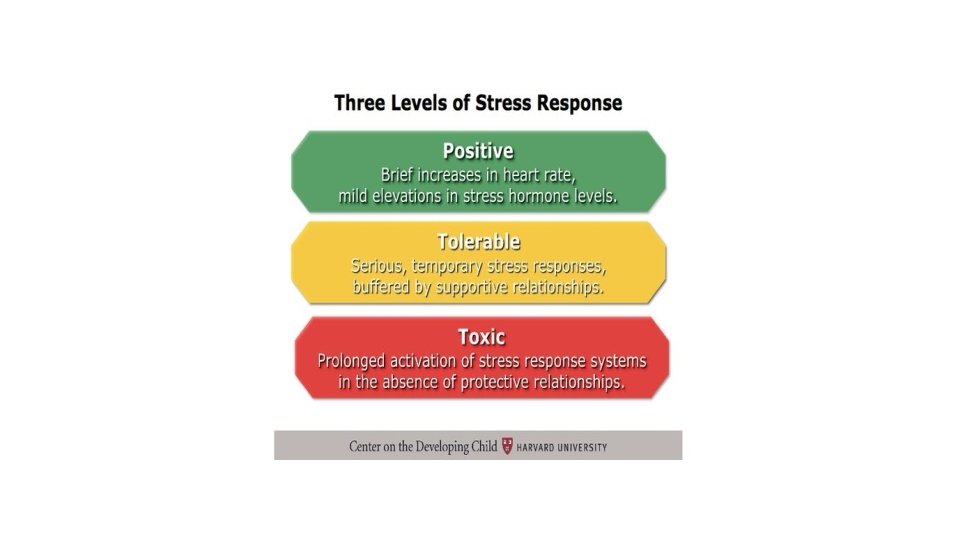
Childhood Adversity • Childhood adversity – wide range of circumstances that pose a threat to health and well-being • ACEs – a subset of Childhood Adversities • Social disadvantage, including homelessness, discrimination, community violence, historical trauma • Trauma – one possible outcome of exposure to adversity • Toxic Stress – occurs when adversity is extreme, long-lasting and severe (such as chronic neglect, domestic violence, severe economic hardship, ACEs) without the buffer of a caring adult.
Effects of Toxic Stress • The activation of the physiologic stress response system results in increased levels of stress hormones. • Persistent elevation of cortisol, can disrupt the developing brain’s architecture in the areas of the amygdala, hippocampus, and prefrontal cortex (PFC), and therefore ultimately can impact learning, memory, and behavioral and emotional adaptation. • Suppresses the immune response, affects other organ systems and makes an infant, child or adult more vulnerable to infections and chronic health problems. • Different exposures to stressors at critical times can affect how a gene is expressed (epigenetics) or how a pathway develops and subsequently the behaviors and health conditions that are manifested over the life of that person.
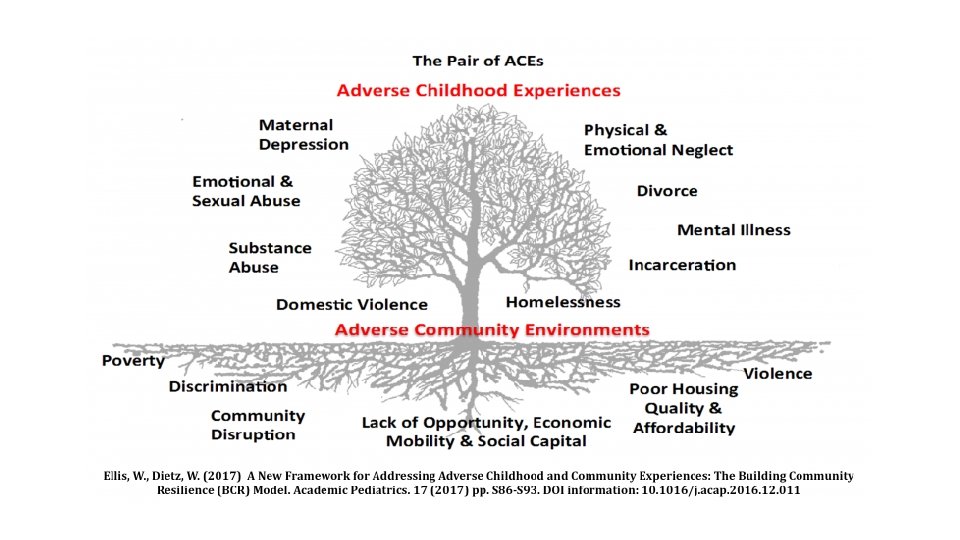
Adverse Childhood Experiences • Recurrent and severe physical abuse • Recurrent and severe emotional abuse • Sexual abuse • Neglect (physical and/or emotional) • Alcoholic or substance abuse in household family member • Imprisoned household family member • Mentally ill, depressed, or institutionalized household family member • Mother treated violently • Parental separation or divorce
ACEs Dose-Response • Children with 3 or more ACEs • 3 X academic failure • 6 X behavior problems • 5 X attendance problems • Adults with 4 or more ACEs • 7 X alcoholism • 2 X cancer • 4 X emphysema • 6 or more ACEs • 30 X suicide
Parental ACEs and Child Development • Perinatal depression • Maternal depression in infancy is predictive of cortisol levels in preschoolers, which is linked with anxiety, social wariness and withdrawal. • When mothers experienced major depression, then attachment disorders, behavior problems, and depression and other mood disorders can occur in childhood and adolescence. • In Israel, cohort 125 mother-child pairs, mothers with depression, followed from birth to age 10; at age 10 mothers had increased cortisol and s-Ig. A and showed more negative parenting; children had more Axis I disorders, higher s-Ig. A, and social withdrawal. Ulmer-Yaniv et al, DEPRESSION AND ANXIETY, August 2018. • Parental ACEs and infant toddler development • Pediatric practice in Oregon – 3 or more maternal ACEs associated with increased risk for developmental delay in multiple domains. Folger et al, PEDIATRICS, Vol 141, Number 4, April 2018 • Canada, women recruited during pregnancy – psychosocial and health risks in pregnancy confer risk through maternal ACEs to developmental outcomes. Racine et al, PEDIATRICS, Vol 141, Number 2, April 2018.
Historical Trauma “A constellation of characteristics associated with massive cumulative group trauma across generations” (Brave Heart, 1999). • cumulative emotional and psychological wounding, over individual lifespans and across generations, • emotional, physical, and political violence directed toward particular peoples or communities • experienced by any individual or group whose past includes persecution, discrimination, and attempts to deny or destroy their language or culture
Robert Wood Johnson Foundation (RWJF) County Health Rankings Components Source: http: //www. countyhealthrankin gs. org/app/northcarolina/2016/ rankings/ 13
Social Determinants of Health Exposu re to hazards Safety/ violence Employm ent Income/ Poverty WHO defines SDOH as the circumstances in which people are born, live, and work, and the systems in place to deal with illness. Circumstances shaped by larger forces such as economics, public policies, and politics. Stress, trauma, ACE Using a Health Equity Lens. IM Co. IIN Learning Session 5 Racism Educatio n Housing Neighbor hood Social support From Kay Johnson
WHO: Social Determinants of Health Social gradients Stress Early childhood development Social exclusion (racism, discrimination) • Unemployment (opportunities for education and jobs) • • • Social support networks • Availability of healthy food (air, housing and water) • Availability of health transportation • Addiction
CAHMI Technical Working Group on SDo. H Screening From Charles Bruner
Perinatal Depression Policy Statement and Technical Report: January 2019 Background • Builds on 2010 Clinical Report • Screening recommended by USPSTF and CMS (2016) • Risk factors – hx of depression, substance use, marital discord, domestic violence, isolation, poverty, young maternal age, difficult infant temperament, multiple birth, preterm birth, congenital conditions, minority/immigrant • Prevalence – 12% of women pregnant or postpartum in a given year; 11 -18% report postpartum depressive symptoms; increased – low income, adolescent • Peak occurrence: 6 weeks postpartum major depression; 2 -3 months postpartum minor depression; postpartum psychosis in first 4 weeks postpartum • Also fathers: 2 -25% (increased if mother has PPD) • Spectrum – postpartum blues, postpartum depression, postpartum psychosis • 2 – generational issue • Earls MF, Yogman MW, Mattson G, Rafferty J, “Incorporating Recognition and Management of Perinatal Depression into Pediatric Practice, ” PEDIATRICS, Volume 143, Number 1, January 2019, pp 73 -81.
Perinatal Depression Impact on the Infant, Dyad, and Family • Potential for toxic stress • Impact on parenting; may: • Hinder bonding, reciprocal interaction, and healthy attachment • Distort perception of the infant’s behavior • Cause the mother to be less sensitive and attuned, indifferent or more controlling • Impair the mother’s attention to, and judgement for, health and safety. • Discontinuation of breastfeeding • Neglect, abuse • Family dysfunction
Examples of Social Determinants That Protect Health • Parental knowledge and skills about child development and caretaking • Good parental or caregiver physical and mental health • Positive father involvement • Strong emotional bond or attachment between infant/child and parent/caregiver • Social supports (ie. , friends, neighbors, relatives, faith-based groups, and other agencies) • Safe and good housing • Stable/secure home life • High school education level or higher for parents/caregivers • Opportunities for stable income/employment for household • Food security for household • Safe neighborhood with no violence • Community resources for fresh produce, exercise, social interactions
Strengthening Families’ Five Protective Factors Framework 1. Parental resilience 2. Social connections 3. Knowledge of parenting and child development 4. Concrete support in times of need 5. Social and emotional competence of children Source: http: //www. cssp. org/reform/strengtheningfamilies
Protective Factors: CSSP & AAP Guidance for PCCs https: //www. cssp. org/reform/strengthening-families/messaging-atthe-intersection/Messaging-at-the-Intersections_Primary. Health. pdf
Promotion of Protective Factors Examples: Reach Out and Read Learn the Signs, Act Early
Two Generational Approach to Health • The individual and interpersonal development, health and well-being of children and their parents are linked • Parents and children can learn together skills to adapt positively to risk and adversity and thrive (i. e. , executive functioning and mindfulness) • Additional components are needed to support a two generation approach which include early childhood through postsecondary education, employment pathways, economic assets, and social capital See Two Generation Approach from the Aspen Institute: www. ascend. aspeninstitute. org/pages/the-two-generation-approach
Resilience is the process by which a person moves through a traumatic event, utilizing various protective factors for support, and returning to “baseline” in terms of an emotional and physiologic response to the stressor. It is the process of utilizing one’s protective factors to navigate successfully through a stressful situation. Resilience provides a buffer between the child and the traumatic event, mitigating the negative effects that could result, such as physical, emotional, and behavioral health issues that can last even into adulthood. (excerpted from AAP Resilience Project) www. aap. org/resilience (>Children Exposed to Violence & Toxic Stress > Promoting Resilience)
Trauma-Informed Primary Care • Integrates an understanding of the prevalence of adverse childhood experiences and their impact on lifelong health • Science reveals that the environment in which children develop – family, community, and culture – impacts brain development, health and genetics • In the medical home, being trauma-informed is essential for prevention and amelioration of this impact
What is Trauma- and Resilience-Informed Care? AWARENESS DETECTION INTEGRATION • Realizes the widespread impact of trauma and understands potential paths for recovery • Recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system • Responds by fully integrating knowledge about trauma into policies, procedures, and practices, and seeks to actively resist retraumatization
Trauma- and Resilience-Informed Care • Recognizes the importance of patient/family involvement in service design • Recognizes the importance of multi-generational care • Integration has to include community services that address “social determinants of health” – truly integrated into diagnosis and treatment planning • Services and treatment have to address historical trauma and ongoing discrimination, institutional racism
NCTSN (National Child Traumatic Stress Network) • Routinely assess for trauma exposure and related symptoms • Use evidence-based, culturally responsive assessment & treatment • Make resources available to children, families and providers on trauma, its impact, and treatment • Engage in efforts to strengthen the resilience and protective factors • Address parent and caregiver trauma and its impact on the family • Emphasize continuity of care and collaboration across systems
The Conversation • Screening is an opportunity to engage the patient/family and to build trust • Screening always involves a conversation • Inquire about social determinants that are protective as well as those that confer risk • The purpose is not to “solve” every issue immediately • The question is “where should we start together? ”
Recommendations: Children & Families • Recommendations: • Bright Futures • Screenings • Ask about parental strengths and Social Determinants of Health (SDo. H) at every well-visit • AAP Screening in Practices Project • National Advisory Board and Project I-SCRN • Developmental and behavioral (including social emotional), autism, perinatal depression, social determinants of health • AAP Mental Health • Psychosocial assessment (social-emotional, SDo. H, ACEs) at every well visit • Brief mental health update at acute visits
The Role of the Medical Home • Support of the dyad and family • Promote healthy social-emotional development • Implement screening • Identify and use community resources • Coordinate access to treatment • All of the above are consistent with: • Bright Futures – elicit parental strengths and assess social determinants of health • AAP Mental Health Competencies for pediatric practice
Implementation • Practice Implementation aligns with recognition of toxic stress, ACEs, and importance of trauma/resilience-informed care • Intervention and referral optimized by collaborative relationships with community resources and integrated mental health in primary care.
Tools with Multiple SDo. H Areas • Health Leads Toolkit https: //healthleadsusa. org/wp-content/uploads/2016/07/Health-Leads-Screening-Toolkit-July-2016. pdf • PRAPARE (Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences) FQHCs • WE CARE (Well Child Care, Evaluation, Community Resources, Advocacy, Referral, Education Survey Instrument) • SEEK (Safe Environment for Every Kid) • SWYC (Survey of Well-being of Young Children) • Family Psychosocial Screen (Pediatric Intake Form)
Tools for Specific SDo. H • Hunger Vital Sign • Addressing Food Insecurity: A Toolkit for Pediatricians • http: //ww. frac. org/aaptoolkit • Housing Stability Vital Sign
Tools for ACEs • Center for Youth Wellness (Nadine Burke, MD) • Child • Teen self report • The Children’s Clinic (RJ Gillespie, MD) • ACE Score (parent) • Resilience Score (parent)
Health Leads Toolkit • Essential • Food insecurity* • Housing instability* • Utility needs* • Financial resource strain* • Transportation* • Exposure to violence* • Optional • Child care* • Education* • Employment • Health behaviors • Social isolation and supports • Behavioral/mental health Recommended tool* has 10 questions Additional validated questions by category to expand or customize
PRAPARE • Items: 17 -21 • Areas • • • Domestic violence Education Employment Family Member Incarceration Financial security/stress Housing Safety Stress Transportation
WE CARE • Items: 6 • Areas: • • • Childcare Education Employment Food insecurity Housing
SEEK • Poison control • Smoking • Food insecurity • Discipline/behavior • Depression • Domestic violence • Substance use
SWYC Family Questions • Smoking • Substance use • Food insecurity • Depression • Domestic violence
Family Psychosocial Screen • Items: ~56 • Areas: • • Caregiver education Family history Health habits – safety, domestic violence, guns, smoking Substance use Parental childhood experiences – discipline, abuse, neglect Depression Support system
CYW: 3 Forms • Section 1 – 10 questions (original ACEs) • Section 2 - 7 -9 questions (additional early life stressors) • Scoring: Section 1 plus Section 2 • If 0 -3 without symptomatology – anticipatory guidance • If 1 -3 with symptomatology OR > 4 – refer for treatment
The Children’s Clinic • ACE Score • Resilience Score • Comments, Questions and Concerns • Interest in Resources
The “New Mexico Three” • has anything major (traumatic, etc - use your own terms) happened since the last time we've met • if so, how has it had an impact on you and your family (again, whatever scope is appropriate) • despite that, what's been going well for you
Coding and Billing - SDo. H • CPT • 96160 – health risk screening • ICD-10 • Z-codes – array of Z-codes that align with social determinants categories and ACEs
Tools for Perinatal Depression Screening • Edinburgh Postpartum Depression Scale or PHQ-2 followed by the Edinburgh or PHQ-9 • Routine screening with Edinburgh Postpartum Depression Screen, PHQ-9, or SWYC (includes Edinburgh) at 1, 2, 4, and 6 month well-visits. Also appropriate for the prenatal visit. • EPDS • • Completed by the mother/parent At 1 month, 2 month, 4 month, 6 month visits Simple 10 multiple choice questions Score of 10 or greater indicates possible depression English and Spanish Sensitivity – 86%; Specificity – 78% Available on line
Coding and Billing – Perinatal Depression CPT • 96161 – health risk screening of caregiver for benefit of the patient • 96127 – social-emotional screening for infant (as part of follow-up) ICD-10 • If there are concerns about the dyad relationship, the code Z 62. 820, Relationship Specific Disorder or Infancy/Early Childhood, (published in the DC: 0 -5 - Diagnostic Classification for 0 -5 year olds, 2016) can be used as secondary to the well-visit code. • If attachment problems meet the DC: 0 -5 criteria for Reactive Attachment Disorder, the code is F 94. 2.
Readying the Practice • Develop and foster a trauma and resilience-informed environment • Build relationships with the community to support patients and families • Engage with families in their own care • Assess whole family health and resilience • Address whole family health and resilience • Coordinate services and supports for families
Environment • Involve families at organizational level (planning, implementation, evaluation) • Educate staff regarding trauma, resilience, SDo. H, and traumainformed care • Create & support healthy office environment
Build Relationships • Understand the community’s strengths and needs • Develop relationships with community partners (e. g. housing food security, employment assistance, Child welfare, transportation…) • Develop partnerships medical and mental health specialists
Engage Patients/Families in their Own Care • Plan and make decisions collaboratively with patients/families, asking about their goals and preferences • Engage parents as experts on their child
Assess Whole Family Health and Resilience • Ask about risks and protective factors • Choose a screening tool/validated questions • Develop and utilize a standardized, respectful, culturally appropriate message about the reason for screening • Always acknowledge completion of the screen and discuss
Primary Care Intervention • Transdiagnostic Approaches • Common Factors communication skills • Components of interventions common to diverse therapies; coming from family therapy, cognitive therapy, motivational interviewing • See HELP mnemonic • Common Elements • Components of therapies that apply to a group of related conditions (such as anxiety, low mood, ADHD)
Skills to Engage the Child and Family: the “Common Factors” Approach HELP build a therapeutic alliance: • • H = Hope E = Empathy L 2 = Language, Loyalty P 3 = Permission, Partnership, Plan Wissow LS, Gadomski A, et al. Improving Child and Parent Mental Health in Primary Care: A Cluster. Randomized Trial of Communication Skills Training. Pediatrics. 2008; 121(2): 266 -275
Primary Care Intervention: Perinatal Depression • For pediatrics, the focus is on the dyad • Primary care intervention Promote the strength of the mother-infant relationship Encouragement and reassurance re breastfeeding (may be protective) Encouragement of understanding and responding to the infant’s cues Encouragement of routines for predictability, sleep, diet, exercise, and stress relief • Promote realistic expectations and prioritizing • Encouragement of social connections • •
Address Whole Family Health and Resilience • Raise awareness of links between trauma/stress and health • Provide support at the visit • Link patient/family to services and supports
Perinatal Depression Screening: Immediate Action If the Edinburgh Score is 20 or greater or the answer to question 10 is yes, or If the mother expresses concern about her or her baby’s safety, or If the PCC suspects the mother is suicidal, homicidal, severely depressed/manic or psychotic… üRefer for emergency mental health services üBe sure she leaves with a support person (not alone) and has a safety plan
Perinatal Depression Referrals and Linkages • Referral - for mom, the dyad, the infant • Mom • Mental health professional • PCC or OB • Lactation support • Infant • EI for targeted promotion of social-emotional development • Dyad • CPP, ABC, COS • Follow-up – includes social-emotional screening of the infant (e. g. ASQ: SE-2, Baby PSC)
Referral for the Dyad • The mother and child need to be referred to a professional with expertise in the treatment of very young children. • Evidenced based treatments • Circle of Security (www. circleofsecurity. org) • Child-Parent Psychotherapy (Child First) • ABC (Attachment & Biobehavioral Catch up) • Part C services can provide modeling for interaction and play with the infant to promote healthy development
Important Linkages for the Medical Home: Nurse Family Partnership Part C – Early Intervention Lactation Specialists Parent Educators Family Support Groups Parent-child groups Mother’s morning out Early Head Start Child Care Health Consultants Mentoring and Home Visitation • Parents as Teachers Program • Healthy Families America Program • Faith based and other volunteers • Community mental health providers • • •
“Closing the Loop” • It is possible to measure rates of screening in practice, BUT • Continued challenges: • Tracking referrals – need for registry functionality in EHRs; navigators as part of practice • Obtaining feedback – how to standardize communication with “non-medical” partners • Assessing outcomes for children and families • Examples of systems for feedback and follow-up • North Carolina NCCare 360 and Healthy Opportunities • Help Me Grow
Coordinate Services and Supports • Provide coordinated, integrated care • Standardize co-management processes • Work across sectors
Systems Building, Cross-sector Collaboration • Needed to provide support to practices for the “heavy lift” • Role of the AAP Chapter as convener and advocate? • Engage state partners • Goal: to remove barriers, align policies and payment with priorities for children and families
What We Are Learning • Routinely eliciting patient/family strengths is transformative to practice • Clinicians and patients/families can discuss social determinants- those that increase risk, and those that are protective • Adverse Childhood Experiences (ACE’s) are common, but resiliency can ameliorate their impact • Trauma-informed care needs to include a focus on promotion and prevention as well as intervention • Engaging the patient/family as a partner is key • Promoting resiliency is central to addressing social determinants of health
SDo. H & ACE Screening Resources The AAP Resilience Project Tools https: //www. aap. org/en-us/advocacy-and-policy/aap-health-initiatives/resilience/ Pages/Clinical-Assessment-Tools. aspx The AAP screening website (STAR Center) SDo. H tools https: //www. aap. org/en-us/advocacy-and-policy/aap-health-initiatives/Screening/ Pages/Screening-Tools. aspx
Trauma –Informed Resources • Implementing Trauma-Informed Integrated Care (toolkit) https: //picc. jhu. edu/the-toolkit. html • The National Child Traumatic Stress Network https: //www. nctsn. org/
Screening Resources The AAP Resilience Project Tools https: //www. aap. org/en-us/advocacy-and-policy/aap-health-initiatives/resilience/ Pages/Clinical-Assessment-Tools. aspx The AAP screening website (STAR Center) SDo. H tools https: //www. aap. org/en-us/advocacy-and-policy/aap-health-initiatives/Screening/ Pages/Screening-Tools. aspx
The STAR (Screening Technical Assistance & Resource) Center www. aap. org/screening