Sexual health in primary care Dr Louise Knowles



















 � Blood")








 � Discharge PV/urethral")

 �")
 � Urethral swab?")





;")



")




 �Anti-mitotic ( Podophyllotoxin) �Immune modfication ( Imiquimod)")
































 �")
- Slides: 84
Sexual health in primary care Dr Louise Knowles, GP. 12/12/16
Aims for today � STI trends � Sexual history taking/techniques � Management of common STI’s � Vaginal discharge
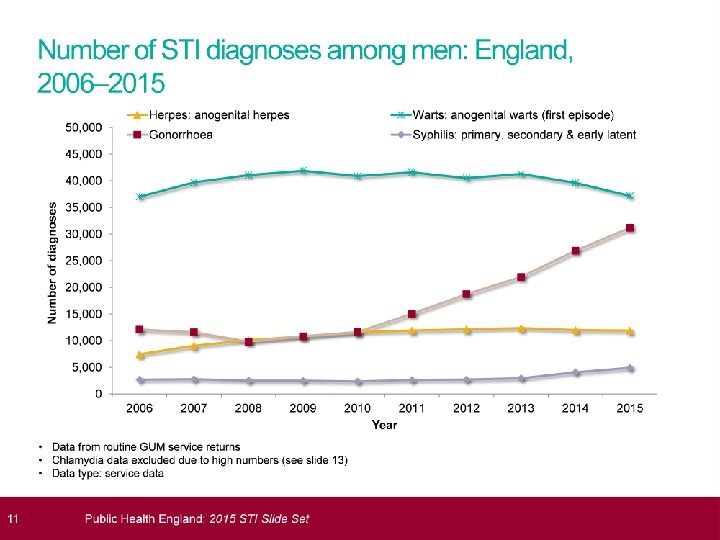
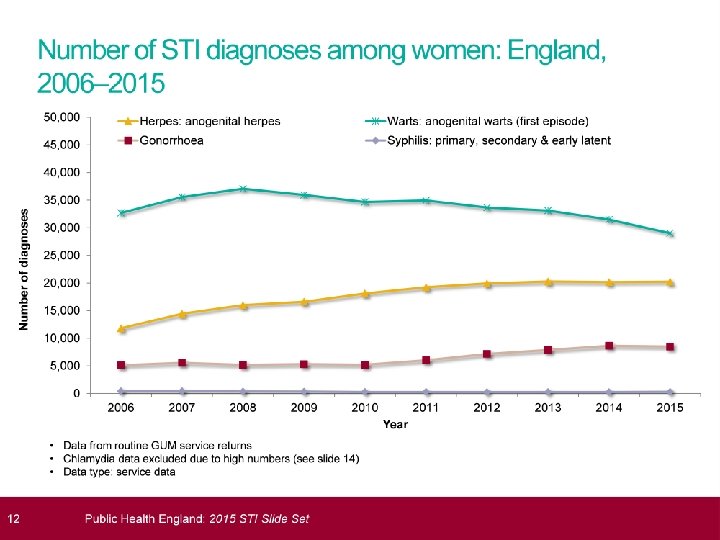
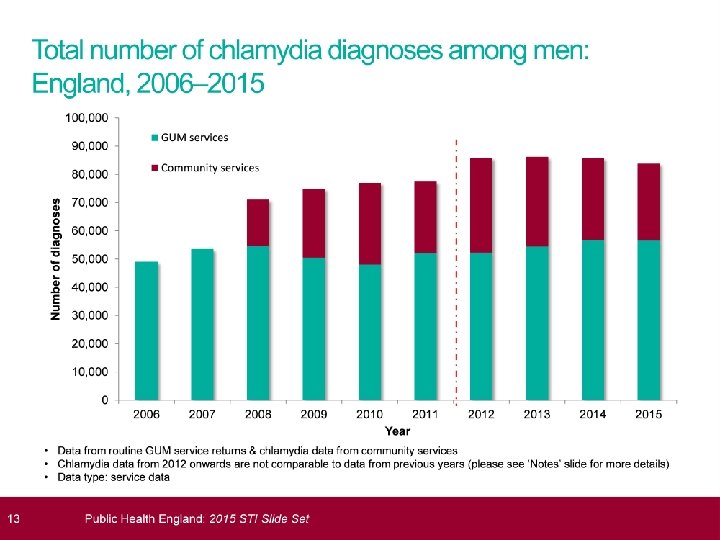
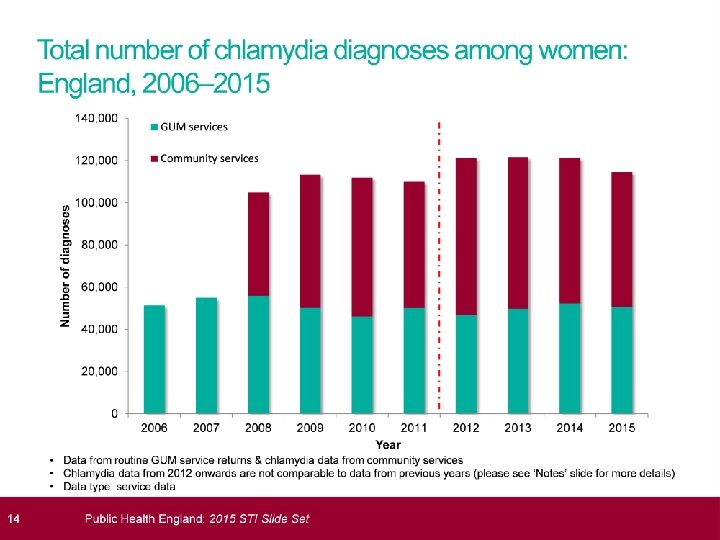
STI’s 2015; HPA data � 435, 000 diagnoses STI � Mainly heterosexuals<25 and MSM � Most common chlamydia; 200, 288 cases � Largest proportional increases in syphllis (20%increase) and gonorrhoea ( 11%increase) � Genital warts ( new) reduced by 7% � More than 1. 5 million chlamydia tests and 129, 100 cases. � Overall reduction in rate of chlamydia testing
NATSAL 2010 � 4. 3% men have paid for sex � 5. 4% men and 4. 9% women same sex contact � 14% men and 9% women have concurrent sexual relationships � 1/3 men and 1/10 women had at least 10 lifetime partners.
What is sexual health care? �Risk assessment �STI; prevention, diagnosis, treatment �Contraception �Management of unplanned pregnancy.
Setting the scene �You are running 20 minutes behind �Just moved from 15 to 10 minute appointments �Your nurse is off sick �“while I’m here. . . ”
Typical scenario; � 17 year old Emma , attends for cocp �Last 3 months bleeding after sex and between periods. �Commonest cause BTB? �What will you ask? �What tests will you do?
Emma, post coital bleeding � Boyfriend, 18, 2 weeks. � Previous BF “cheated” on her � UPSI at a party with another boy last month. � No missed pills � What are the minimum tests you will offer to Emma?
Minimum investigation � Chlamydia � Gonorrhoea � HIV � Syphilis.
Which tests? Woman with symptoms PV exam, triple swabs. Endocervical swab for chlamydia/gonorrhoea Urine for chlamydia not sensitive enough If unable/declines swab/Friday pm; self taken vaginal swab almost as good. Arrange blood test for HIV, syphilis( and hep B if at risk)
HIV/Hepatitis risk � IVDU � Sex with someone from overseas � Commercial sex workers � MSM/bisexual � Sexual assault victims � Operations/transfusions abroad � If high risk; check serology, offer Hep B vaccination.
Essential components sexual history; warning shot? � How long with current partner? Date last sexual contact. � Any other partners in the last 3 months? � When did you last have sex with someone else? � Partner gender and sites of exposure. � Female; LMP and contraception. � Condoms? � Assess risk HIV/hepatitis B and C/vaccination? � Child protection issues. � How to access results.
Sexual history taking; good questions �I need to ask you some routine questions � Do you have a regular partner? � When did you last have sex? � Was that with a regular partner? � How long have you been with them? � Do/did you use condoms at all? � Have you had any accidents? � When did you last have sex with anyone other than them? � Is your partner ok?
Sexual history taking; questions to avoid!! � Don’t be embarrassed but… � Are you married? � When did you last make love? � Was that with your boy/girl friend or a one night stand? � Have you been unfaithful? � Have you had a one night stand?
Taking a sexual history �Be non judgmental �Reassure re confidentiality �Be comfortable talking about sex �Communicate with clarity; avoid slang and euphemisms. �Do not make assumptions about sexual behaviour or their partner’s gender.
Child Protection � If under 16; ask about age partner � If concerns; ask about coercion, gifts, age sexual debut, are parents aware. � DISCUSS WITH COLLEAGUES.
Men with symptoms. �John 18 , presents Friday pm with a tender swollen testicle. �What are you going to ask?
John, acute epididymo-orchitis � John is a student, girlfriend Jane for several months. � Last summer while away with friends in Thailand he paid for sex with a female sex worker. This was 2 months ago. � He has no discharge but says it does hurt on occasions when he passes urine. � He and his girlfriend do not use condoms, she is on the pill.
Men with symptoms. � First pass urine for chlamydia and gonorrhoea( NAAT) � Blood tests HIV and syphilis. � Can do swabs eg urethral swab if discharge. � Urgent GUM referral
Acute scrotal pain � Rapid onset � Radiates to groin, loin � ? Trauma � High riding, oblique lie � Occured in past? � Loss cremasteric reflex � Urine NAD � Hot, swollen, tender � Pyrexia � +/_ groin LN � +/_ penile discharge � Assoc. LUTS � Often part of STI Torsion Epididymo-orchitis
Acute epididymo-orchitis � Usually complication of urethritis; don’t forget mumps. � Ideally; urgent GUM referral. � If you suspect non-gonococcal and GUM referral not possible, may treat empirically; after tests taken and before results back; � Doxycyline 100 mg bd, 14 days � OR Ofloxacin 200 mg bd , 14 days
Why refer GUM? � Partner notification � More rapid diagnosis � Culture and senstivity needed for gonorrhoea � Counsellors and support service. � Gonorrhoea; complex; treatment includes injection � Gold standard tests. � Uncertainty about diagnosis � Free treatment
Common STI’s � Many opportunities � High index suspicion in under 25’s � Basic knowledge of how may present. � Reservoir of asymptomatic infection! � Have procedures in place for initial investigation. � Be aware of onward path referral/partner notification.
Don’t forget… � Agree how you are going to communicate results. � Ensure up to date mobile number.
Common STI’s � Chlamydia � Genital warts � Genital herpes � Trichomoniasis � Gonorrhoea � (HIV)
Chlamydia. � Obligate intracellular pathogen, lifecyle 48 - 72 hrs � Infects mucous membranes; urethra, cervix, pharynx, conjunctiva. � Commonest bacterial STI in UK � 70% asymptomatic � 2/3 partners of those infected will also be infected
Chlamydia � <25 yrs � More than one partner in 1 yr � Recent new partner; most significant � Lack consistent condom use � Infection persists >1 yr in 50%(untreated) � 95% clear spontaneously by 4 yrs.
How does chlamydia present? � Abnormal bleeding ; IMB/PCB ( cervicitis) � Discharge PV/urethral � Urinary symptoms; beware sterile pyuria � Testicular pain � Pelvic pain/dyspareunia � Ectopic pregnancy/infertility � RUQ pain; perihepatitis; “Fitz Hugh Curtis” � Neonatal conjunctivitis/pneumonitis � Reactive arthritis
Chlamydia testing � Opportunistic screening…. NCSP � TOP � Change partner; suggest 2 week time window
Which test? ~women � Symptomatic; endocervical swab 360 degrees in cervical os. (NAAT) � Or if not possible; self taken vulvovaginal swab has good sensitivity � Self taken swab; 2 inches inside vagina, rotate for 30 secs. . . BASHH guidelines. � NAAT samples can be tested several days later
Which test; men � First pass urine( hold for one hour) � Urethral swab? � Look back period; 4 w for acute urethritis, 6 m for other presentations.
Chlamydia positive � Need full STI screen � Will need GUM referral for partner notification � Document reasons for this. Treatment; Azithromycin 1 G stat or Doxycyline 100 mg bd 7/7 IUD in situ; no need to remove
Chlamydia in pregnancy � BNF suggest avoiding azithromycin but no evidence harm; off licence � Can use erythromycin 500 mg bd 10 -14 d. or ofloxacin 200 mg bd 7 d. � SIGN recommends use of azithro for pragmatic reasons; compliance. � Test of cure recommended
NO SEX FOR 7 DAYS AFTER STAT DOSE.
Genital herpes � Most infection acquired without symptoms � 80% UNAWARE they are infected � HSV 1 and 2 oral and genital � Infection is LIFELONG � Primary attack may be many months after exposure. � Increasing numbers first episodes; change sexual behaviour and use highly sensitive diagnostic tests.
Genital herpes �Primary infection; malaise, flu like symptoms, tingling sacral dermatomes �Tender inguinal LN �Dysuria and blister; 3 weeks �The “dripping tap”
Genital herpes � Inv; � HSV � Rx. � � viral swab ( NAAT); 71% detection culture will miss 30% Saline bathing Oral antiviral Lidocaine ointment 5% � Follow up; full STI screen 2 -3 w later.
Episodic treatment HSV � No advantage between different antivirals. � Consider short course treatment ( more cost effective/better compliance) BASHH � Rx Aciclovir 800 mg tds 2/7 � ( Aciclovir 200 mg 5 times daily 5/7) � Patient intiated treatment
Recurrent genital herpes �Prodromal symptoms �Less severe �Start with prodrome �Average recurrence higher with HSV 2 �Can consider suppressive therapy. �eg aciclovir 400 mg bd.
Points you should cover; HSV � Abstain during prodrome/lesions � Asymptomatic viral shedding � Male condoms reduce risk transmission � Disclosure advised. � Document these discussions.
Genital herpes � Partner notification? � BASHH statement of criminal prosecution 2011. ( Golding) � UK: COURT OF APPEAL UPHOLDS MAN’S CONVICTION FOR RECKLESSLY PASSING ON GENITAL HERPES DURING SEX WITH EXGIRLFRIEND
Pregnancy and HSV � Primary infection higher risk � Refer GUM � Rare but catastrophic neonatal infection � Aciclovir may be given from 36 weeks � Aim for vaginal delivery if no vulval lesions at labour.
Psychological distress+++ � When did I catch this? � Will my partner get warts? � Does it mean I will get cervical cancer? � Should I have more frequent smears? � How can I get rid of it? � Will it come back? � Can I be cured?
Genital warts; the facts � HPV 6 and 11 � CIN 16 and 18 � Head and neck cancers 16 � 30 -50% sexually active adults have postive serology for genital HPV � Sexual transmission; digital or oro-genital � Most commonly in areas of abrasion but CAN OCCUR ANYWHERE.
Warts are just cosmetic. � There is often a long latent period before wart appears � Most infection is sub-clinical � <10% of those infected get lesions � HPV DNA no longer detectable in 95% by 2 yrs post infection. � Worse in smoker, pregnancy, immunosuppressed. � Don’t assume perianal warts due to anal intercourse.
Genital warts; treatment �None �Destruction ( cryo) �Anti-mitotic ( Podophyllotoxin) �Immune modfication ( Imiquimod) �Surgery
Warts; refer GUM? � Podophyllotoxin, cream or solution � Apply bd for 3 days, 4 day break, up to 4 courses � Imiquimod; apply nightly 3 nights per week for up to 16 weeks. � No partner notification , screen other STD’s
Gonorrhoea; who? � Urban areas � Young adults � MSM � Black/ethinic minority populations � Partners of the above!
Gonorrhoea. � Infects mucous membranes, oropharynx, rectum, urethra, conjunctivae. � Enhances transmission HIV � Test no less than 3 days after contact; convention is to test 14 d after for GC and chlamydia � Which test?
Testing for gonorrhoea � Endocervical/self taken swab for culture; minimal delay to lab � NAAT’s more sensitive, less invasive. ( can be done on first pass urine men, self taken HVS women) � If NAAT positive always need swabs for culture for sensitivities. � GUM referral!
Gonorrhoea resistance. � Outbreak high level azithromycin resistant cases originated in Leeds, heterosexuals. � 17 cases so far this yr, spreading into MSM population � First case in 2016 of dual resistance to azithromycin/ceftriax one
Treatment of gonorrhoea � REFER GUM � Testing required to test sensitivity. � Treatment is with IM ceftriaxone and oral azithromycin, both as stat dose. � Not a role for primary care!
Dan age 19 � First year student, come home for holidays � Pain when passes urine. � What else are you going to ask? � Take a sexual history.
Dan, 25 , dysuria � Which � A. of the following would you do? Give 7/7 trimethoprim, see if no better. � B. Check msu and see with results � C. Take sexual history, urine for chlamydia � D. Take sexual history, urine for GC and chlamydia. � E. Recommend he attends GU clinic.
Dan, dysuria � Dan has long standing girlfriend Fiona at home who he met at school; she was his second sexual partner and is on the pill so they don’t use condoms. � During first term one episode UPSI at party 3 weeks ago. � Uses some recreational drugs but no high risk behaviour. � Hurts to pass urine, also admits to slight urethral discharge.
Male urethritis/NGU � Mostly sexually acquired � Chlamydia � Mycoplasma genitalia � “non specific urethritis”; various organisms. This is really a diagnosis of exclusion. eg mycoplasma, ureaplasma, adenovirus, HSV � REFER GUM; needs partner notification
Suspected chlamydia/GC/NSU � “syndromic” treatment; ie without tests, not recommended � “empirical “ treatment( ie treatment at time of consultation, before test results); may be appropriate, eg Friday pm, where investigation is declined or not possible. Don’t forget treatment for partners!
Vaginal discharge �Physiological �Commensals; candida, staph aureus, group B strep; can “overgrow” �Consider non infective causes �Eg. Foreign body, cervical ectopy, endometrial polyps, malignancy.
Infective causes Sexually transmitted Chlamydia Gonorrhoea Trichomonas HSV Non sexually transmitted Bacterial vaginosis Candida
Vaginal discharge; history. � Type of discharge. � Any itch or malodour? � What treatment tried otc? � Any symptoms to suggests PID? � Take a sensitive sexual history. � Symptoms or recent treatment for partner. � PMH � Cyclical symptoms?
Trichomonas � Infects vagina, urethra, under foreskin � Invariably sexually transmitted � Both sexes; 50% asymptomatic � Symptoms; discharge, dysuria, itch++ � Comps; preterm delivery, low birth weight � Enhances HIV transmission
Trichomonas � If you suspect it; refer GUM � If you find it; treat and refer for PN � Treatment; metronidazole 2 G stat/400 mg bd 5 -7 days. � Partners should be screened for all STI’s and treated for TV regardless of results.
BV or candida? � Thin discharge � Odour+ � No itch � Vulva; NAD � Ph>4. 5 � BV � Thick discharge � Odourless � Itch++ � Vulvitis/dysuria � Ph<4. 5 � Candida
Bacterial Vaginosis � Commonest cause “abnormal” PV discharge reproductive age. � Mixed anaerobes � Rx; oral metronidazole 2 g stat or 400 mg bd/metronidazole vaginal gel/ topical clindamycin; equally effective � Pregnancy; increased risk preterm birth /late miscarriage; so treat; either of above ok but avoid high stat dose metronidazole.
Lactobacilli Mixed anaerobes Vaginal p. H Interplay between vaginal p. H, normal and abnormal bacteria
Recurrent BV � Avoid douching/excessive cleansing � Acidifying gels may help prevent � More common in smokers/IUD users � Association, not causation sex; more common with new partner. � Oestrogen favours lactobacilli. � Often co-exists with other STI’s � Suppressive treatment? (Metronidazole 0. 75% gel, twice a week 16 weeks. )
Recurrent candida; myths � Do not arise from re-infection by partner � No evidence for pro-biotics, natural yoghurt or special yeast free diets! � Believe negative swabs! � Asking for culture may yield non albicans.
Pathogenesis recurrent VVC � Some women have aggravated inflammatory response; genetic predisposition; atopic? � Minimal plaques but lots of inflammation v obvious candida plaques but minimal symptoms. � Topical skin care essential
Treatment of recurrent VVC Fluconazole 150 mg ; 3 doses 72 hrly then 150 mg weekly for 6 months. Median time to clinical recurrence, fluconazole v placebo; 387 with proven recurrent VVC; � Fluconazole 10. 2 months � Placebo 4. 0 months. Sobel, NEJM 2004
HIV; always think about it! � HIV is treatable � Late diagnosis leads to high HIV related morbidity and mortality in UK � Test if indicator diseases. � In depth “counselling” not necessary � Insurance? � 3/12 “window”
HIV ; indicator diseases � Bacterial pneumonia � Severe seborrhoiec dermatitis � Peripheral neuropathy � Oral candidiasis � Chronic diarrhoea unknown cause � Weight loss unknown cause � Lymphadenopathy unknown cause � Neutropenia, lymphopenia
HIV PEPSE 2015 � Post exposure prophylaxis after sexual exposure � To start within 72 hrs, preferably within 24 � One month antiretroviral therapy � Patients may ask for it or you may feel it is worth giving after sexual history. � REFER GUM
Acute PID �¼ due to chlamydia/gonorrhoea; also implicated; gardnerella, anaerobes. � Positive predictive value of clinical diagnosis is 65 -90% � Low threshold for prompt empirical treatment � Repeated PID; exponential rise infertility � Need to always exclude pregnancy � Partners need testing and treating. � Treatment governed by local epidemiology.
Acute pelvic inflammatory disease, BASH 2011 � 500 mg im ceftriaxone stat. & doxycyline 100 mg bd 14/7 &mnz 400 mg bd 14/7 OR( when low incidence gonorrhoea) � Ofloxacin 400 mg bd & mnz 400 mgbd 14/7 Swabs may be negative Test and treat contacts.
Zika virus � All returning female travellers from at risk areas should avoid becoming pregnant for 8 weeks. � Male travellers returning should use condoms for 6 months. � Pregnant women are advised to postpone non -essential travel to endemic areas � If travel cannot be avoided pregnant women can use 50% DEET � www. gov. uk; Zika primary care. virus infection; guidance for
Take home messages. � Test for chlamydia if sexually active<25 annually or at change or partner. � Consider also testing for GC � Encourage condoms � Take more sexual histories! � Enable rapid access to treatment and partner notification.
References � www. bashh. org( � www. fsrh. org joint guidelines RCGP 2013) � www. chestersexualhealth. co. uk � 2013 national guidelines sexual history taking; BASHH. � Management of vaginal discharge in non GU settings, FSRH 2012