Determinants of Global Health and Primary Health Care

Determinants of Global Health and Primary Health Care Global Health 101 by Stephen Gloyd, MD, MPH Professor Department of Global Health University of Washington January 2014

Outline of talk ¡ Global health status & early responses ¡ Principal determinants affecting health ¡ Historical improvements in health ¡ ¡ Primary Health Care - concept & evolution Alternatives to PHC – Selective PHC & Child Survival
 ¡ Tropical diseases ¡ Diseases of poverty")
Common diseases in low income countries (LICs) ¡ Tropical diseases ¡ Diseases of poverty ¡ Epidemic diseases (malaria, schistosomiasis, hookworm, trypanosomiasis) (diarrhea, pneumonia, tuberculosis, measles, whooping cough) (HIV/AIDS, influenzas, SARs) Disparity in who is affected by these
")
Evolution of health care and disease prevention Colonial Health Care (1800 s – 1960) ¡ Separate care for colonists, indigenous people Vertical Programs: 1910 - 1960 (1977) ¡ Malaria, yellow fever, yaws, small pox, (polio) Era of optimism: 1960’s and 70’s ¡ ¡ Independence, decolonization Disillusion with clinical, vertical approaches l l l China, Cuba social revolutions Kerala, Sri Lanka equity strategies Experiments in Africa
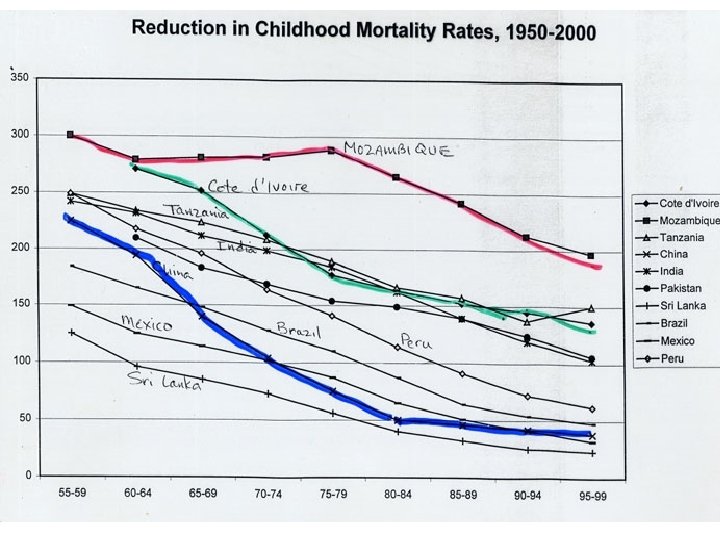

What are the principal factors associated with child mortality?

Children born to educated mothers are healthier

Education effect is independent of poverty

How important is parental education? ¡ Greater than income and access to health services combined ¡ Accounts for most of the rural/urban, family size mortality associations ¡ Maternal is more important than paternal education ¡ Primary to secondary is more important than literacy to primary ¡ Maternal education overrides the effect of decreased nursing, earlier weaning
")
Effect of Education in Women of Reproductive Age on Child Mortality (1970 vs 2009) Source: Gadkidou, E. et al. Increased Educational Attainment and its Effect on Child Mortality in 175 Countries,

Africa has the most severe nutrition problem
 Poorest families have much higher child mortality")
Impact of family assets (income) Poorest families have much higher child mortality

Drinking Water ‘Dirty water kills 1. 5 m children‘ UNICEF 2006 Source: Progress on Drinking Water and Sanitation – UNICEF and WHO Report (2008)
")
Sanitation Source: Progress on Drinking Water and Sanitation – UNICEF and WHO Report (2008)

Decline of respiratory tuberculosis What about the impact of health care? Health interventions and mortality in England & Wales, 1850 -1950 Thomas Mc. Keown The role of Medicine: Dream, Mirage, or Nemesis. 1980 Decline in childhood diptheria Decline in childhood measles

Medicine does make a difference

Worldwide HIV Prevalence Source: UNAIDS website

Medical care can make a difference Source: Towards Universal Access, Progress Report WHO Sept 2009 13 million in ART by end of 2013!

Disparity & mortality

What are the principal factors associated with child mortality? Education Nutrition Family income Water, Sanitation, housing Health Care War and violence Inequality ****** Common denominator: Poverty and Disparity

Determinants of global health Underlying Intermediate Proximate Interests of rich Education Malnutrition Status of women Poverty Water Disparity Sanitation Job conditions Housing Land tenure Debt-SAPs Weak governments Militarism Gender issues Civil strife Health services Health behaviors Imperialism National global Community -national Family Diseases Diarrhea Pneumonia Perinatal conditions HIV Injury Malaria Measles Ebola Individual
 Kerala (India), China, Sri Lanka – Taiwan, S. Korea")
Health success stories (1950 -80) Kerala (India), China, Sri Lanka – Taiwan, S. Korea Common Policies ¡ Primary education ¡ Housing, Water, Sanitation for poor (all) ¡ Food/agriculture subsidies (all) ¡ Land Reform (all) ¡ Protection of nascent industries (Taiwan, S. Korea) ¡ Simple health services (all) - Universal and compulsory (all) Common Denominator – all require government intervention, taxation

Infant Mortality Changes Sri Lanka Kerala State 1940 150 180 1960 100 95 165 1980 35 40 115 1993 15 13 80 $200 $260 1980 GNP/Cap All of India

Thus, we can reduce poverty & improve health, by ¡ Expanding government services ¡ Economic growth helps, but only when the poor get a significant share ¡ Recognition of critical government role (education, health care, agriculture credits, food subsidies, land reform, etc) (1960 -70 s with NIEO, PHC-Alma Ata)
 • Health is a fundamental human right")
Primary Health Care Declaration of Alma-Ata (1978) • Health is a fundamental human right & worldwide goal and requires inter-sectoral action (education, nutrition, poverty reduction) to attain • Improved health and peace requires economic and social development based on New Intl Economic Order • Governments have responsibility to provide adequate health and social measures for health • International cooperation is necessary • Primary health care is appropriate, accessible, acceptable, affordable and requires community participation • HFA 2000 requires redirecting resources from military to social expenditures (including health) Source: WHO 1978

“Essential components” of Primary Health Care 1. Health education 2. Environmental sanitation, especially food and water 3. The employment of community or village health workers 4. Maternal and child health programs, including immunization and family planning 5. Prevention of local endemic diseases 6. Appropriate treatment of common diseases and injuries 7. Provision of essential drugs 8. Promotion of nutrition 9. Traditional medicine Source: Alma-Ata Conference documents.
 Hospital MOH Central Planning Budgeting Procurement Provincial Health")
Primary Health Care Theory Tertiary (National) Hospital MOH Central Planning Budgeting Procurement Provincial Health Supervision Drugs, Lab Office Secondary (Provincial) Hospital M&E Private NGO clinics District Hospital District Health Office CHW Health Post TBA All services Service support Integration of services

Rural Hospital in Mozambique Physician in Pharmacy

Obstacles to PHC – Condition of health facilities Worse and better than we think Maintenance, logistics, management are critical

Crowded clinics, long waits

Rural health post with one nurse

Most resources allocated to tertiary level of care

Why did PHC fail to take off? ¡ Inadequate national political & resource commitment ¡ Internal conflicts in resource allocation - tertiary vs ¡ Western (US) resistance to social change - primary care, private vs public, urban vs rural, doctor-nurse l l right-wing/corrupt dictators in Philippines, Zaire/Congo, Chile, Brazil, Argentina, Pakistan, wars in Central America, Mozambique ¡ Debt and structural adjustment programs – reduction of overall budgets ¡ Child survival programs “adjustment with a human face”

Rise of Neoliberalism “Government is not the solution to our problems. Government is the problem. ” Ronald Reagan, Inaugural Address, 1981 “New World Order” - George HW Bush “Market fundamentalism” - George Soros
 Selective Primary Health Care (Walsh, Warren) Child Survival (USAID) GOBI-FFF")
Alternatives to PHC (Alma-Ata) Selective Primary Health Care (Walsh, Warren) Child Survival (USAID) GOBI-FFF (UNICEF) Growth monitoring Oral Rehydration Therapy Breast Feeding Immunizations Family Planning Female Literacy Food

Global Diseases - 1986 version

Selective Primary Health Care Rationale PHC is great, but can’t afford it PHC requires political will that isn’t there PHC need immense organizational support Ideology of Cost-effectiveness Establish priorities (Can’t do everything at once) Quick fix (short term goals) Trust in power of technology to address social & economical problems

Thank you!
- Slides: 38