PSG Scoring for the Pediatric Patient Jennifer Chen








 present at birth Spindles 2 to 3 mo")
 - AKA: Dominant Posterior Rhythm (DPR) - Their “alpha” rhythm")
")


")






 Transcutaneous CO 2")




- Slides: 27
PSG Scoring for the Pediatric Patient Jennifer Chen Hopkins, M. D. D. ABP, ABIM & Sleep Medicine Texas Society of Sleep Professionals October 28, 2011
Objectives Indications for pediatric sleep study Normal sleep and EEG changes during childhood development Differences between adult and pediatric PSG scoring and interpretation
Kids who may need a sleep study Suspected OSA (snoring + “ADHD”/behavior problems, tonsillar hypertrophy, Down syndrome, craniofacial malformation, obesity, HTN) Suspected Narcolepsy Suspected PLMD Suspected seizure disorder Congenital neuromuscular disorder Suspected central hypoventilation Infants: apnea of prematurity, severe GER, ALTEs/SIDS
Normal sleep in kids Birth to 1 year: Sleep 50 -75% of day, gradually decreases Circadian rhythm begins by 6 mo. , still 2 -3 naps NREM-REM cycles shorter (50 min/50 wga), gradually increases More REM: 40 -50% of TST Preschool kids: 12 -14 hours sleep/24 h Usually phase advanced Take 1 -2 naps Behavioral sleep problems start
Normal sleep in kids School-age kids: 9 -11 hours sleep/24 h No nap 90 minute NREM-REM cycle Increase in slow wave sleep More phase-delayed, towards puberty
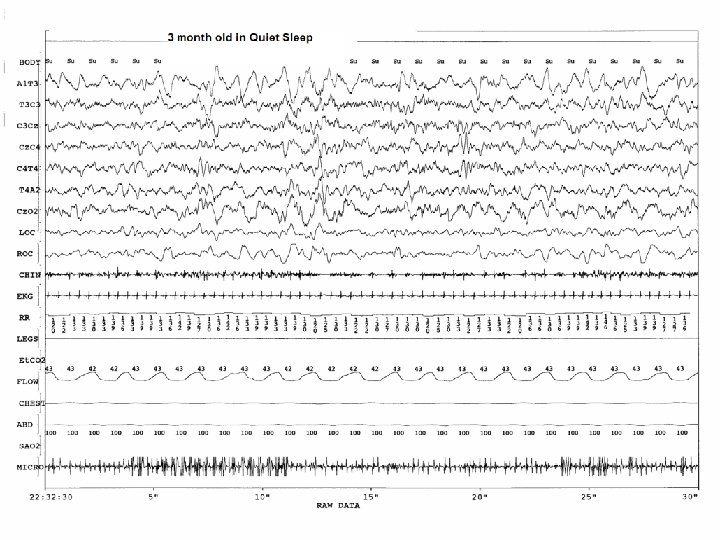
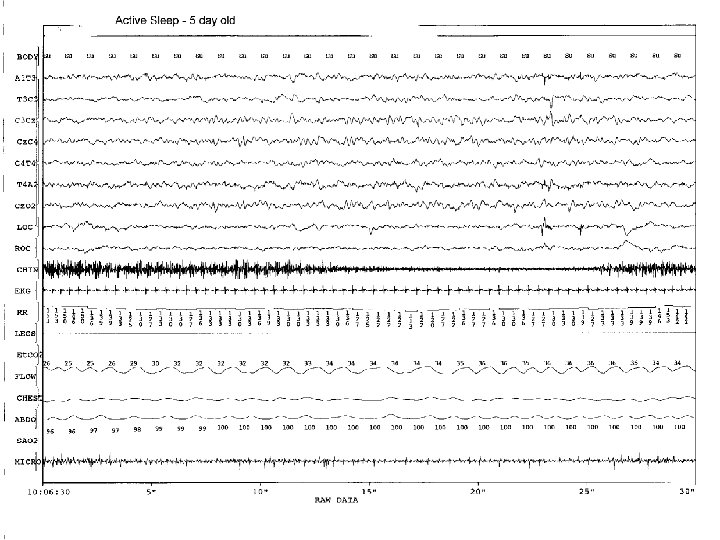
Normal sleep
When to use Pedi Scoring Rules 2 months to 12 yrs – use pedi rules 13 yrs to 17 – can use either adult or pedi rules Better to use 3% desat if use adult rules (C. Marcus, SLEEP v 33, n 10, 2010)
Normal Pediatric Sleep EEG
Normal EEG in kids ODR (“alpha”) present at birth Spindles 2 to 3 mo Delta waves 4 to 5 mo K-complex 4 to 6 mo By 6 mo, should be able to distinguish NREM from REM sleep with EEG.
Occipital Dominant Rhythm (ODR) - AKA: Dominant Posterior Rhythm (DPR) - Their “alpha” rhythm - Occipital leads during eyes closed 3 mo = 3 Hz 6 mo = 6 Hz 3 yr = 8 Hz
Occipital Dominant Rhythm (ODR)
Development of EEG Characteristics Spindles 2 to 3 mo Delta waves 4 to 5 mo K-complex 4 to 6 mo Infants: - May have to stage sleep as Quiet (N) vs. Active (R) sleep. - Use other parameters to help stage: eye movements, chin tone, RR, HR, etc.
Things that look funny but really are quite normal… Tracé alternans Hypnagogic hypersynchrony
Trace Alternans - NREM sleep - Seen in full term newborns (until 3 mo)
Hypnagogic hypersynchrony - Synchronous, high voltage theta waves associated with sleep onset - Seen in infants and children
Pediatric Scoring: Respiratory Events
Respiratory Events OA 90% decreased flow At least 2 missed breaths OH 50% decreased nasal pressure for at least 2 breaths Associated with arousal or 3% desaturation
Respiratory events RERA Discernable fall or flattening of nasal pressure, but <50% Snoring or increase in p. CO 2 Increased respiratory effort At least 2 breaths Central Apnea Absence of respiratory effort for 2 breaths + arousal or 3% desaturation 20 sec or longer without arousal or desat
Pedi Diagnostic Criteria for OSA Mild AHI 1 to 5 Moderate AHI 5 to 15 Severe AHI >15 Only need 7 events during a 7 hour PSG to earn a diagnosis of Sleep-disordered breathing!!!
Other respiratory considerations Hypoventilation: >25% of TST with CO 2 >50 mm Hg Periodic breathing: >3 episodes of central apnea lasting >3 sec, separated by no more than 20 sec of normal breathing. (Physiologic in infants)
Non-invasive CO 2 End Tidal CO 2 (more common) Transcutaneous CO 2
Periodic Limb Movements PLMS in kids are scored the same way as in adults. Only need PLMAI ≥ 5 for diagnosis of PLMD. Can support a diagnosis of RLS.
Take-Home Points Kids need sleep studies for some of the reasons that adults do but also for some reasons specific to Pedatrics (hyperactivity/behavior problems, tonsillar hypertrophy, dysmorphic features). EEG characteristics and sleep staging vary dramatically with age from birth to age 17. Pay attention to ODR and be able to recognize normal EEG patterns commonly seen in pedi patients. Respiratory scoring in pediatrics: NOT the same as adults. Being meticulous is paramount because every event counts!
References The AASM Manual for the Scoring of Sleep and Associated Events, 2007. Sheldon SH, Ferber R, Kryger MH. Principles and Practice of Pediatric Sleep Medicine, 2005. C. Marcus, “Differences in Overnight PSG Scores using Adult and Pediatric Criteria for Respiratory Events in Adolescents”, SLEEP v 33, n 10, 2010. http: //naraamt. or. jp/Academic/kensyuukai/2005 Google images
Questions?