Pharmacology in Nursing Womens Health Drugs Karen Ruffin


 • Development of primary and secondary sex characteristics • Menstrual")
 – Estrone")



 • Treatment of or prevention of disorders that result from estrogen")
 • Continuous-combined hormone replacement therapy (CCHRT) – Fixed estrogen/progestin combination products")


 • Amenorrhea, breakthrough uterine bleeding • Tender breasts, fluid retention,")
 – hydroxyprogesterone – megestrol (Megace)")

 • Palliative treatment of some cancers and endometriosis • Prevention of")
 • megestrol – Adjunct therapy for treatment of breast and endometrial")


 • Other contraceptive forms available – Long-acting injectable form of medroxyprogesterone")




 • May also cause: – Edema, dizziness, headache, depression,")

 • Drugs that may have reduced effectiveness if given with")




 – Bisphonates • alendronate (Fosamax), ibandronate (Boniva), risedronate (Actonel)")
 Biphosphonates • Work by inhibiting osteoclast-mediated bone resorption, thus")
 calcitonin – Directly inhibits osteoclastic bone resorption teriparatide –")

 • raloxifene – Prevention of postmenopausal osteoporosis •")

 • Bisphonates – Headache, GI upset, joint")

 • clomiphene (Clomid, others) – Nonsteroidal ovulation stimulant – Blocks estrogen")
 • Clomiphene (Clomid, others) (cont’d) – Causes increased production of Gn-RH,")
 • Mentropins (Pergonal) – Standardized mixture of FSH and LH –")
 • chorionic gonadotropin alfa (Ovidrel) – Recombinant form of human chorionic")




 Ergot alkaloids • Increase force and frequency of uterine contractions •")
 Prostaglandins • Natural hormones • Cause potent contraction of myometrium, smooth")
 Progesterone antagonist • mifepristone (Mifeprex) • RU-486, the “abortion pill” •")
—Synthetic Form • Used to induce labor at or near full-term")
—Synthetic Form (cont’d) • Other uses – Prevent or control postpartum")


 • Uterine contractions that occur between the 20 th and")
 and terbutaline (Brethine) – Beta-adrenergic drugs – Stimulation of")


 • Before giving any uterine stimulants, assess the mother’s vital signs")
 • For biphosphonates, ensure that the patient has no esophageal abnormalities")
 • Estrogens and progestins – Take the smallest dose needed –")
 • Estrogens and progestins (cont'd) – Increased susceptibility to sunburn may")
 • Follow specific administration guidelines carefully for IV administration of uterine")
 • Instruct patient taking fertility drugs to take the medication as")
 • Biphosphonates – Instruct patient to take medication upon rising in")
 • SERMs – Instruct patient that the medication will need to")
 • Monitor for therapeutic responses • Monitor for adverse effects")
- Slides: 68
Pharmacology in Nursing Women’s Health Drugs Karen Ruffin RN, MSN Ed.
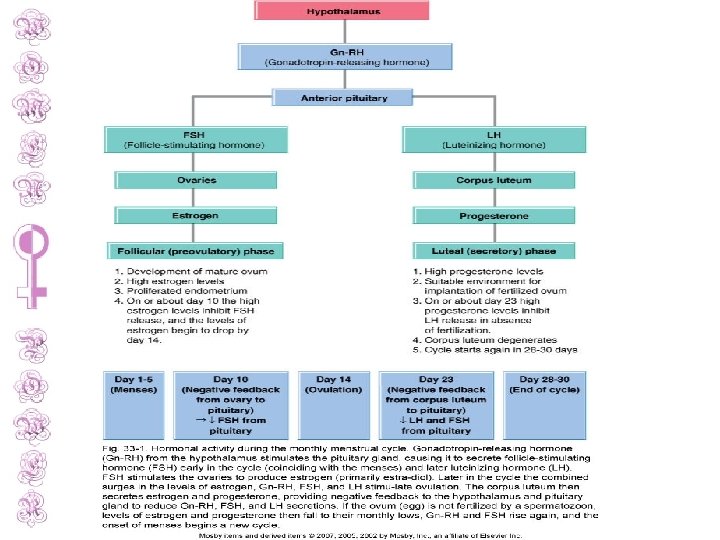
Female Reproductive Functions • Female sex steroid hormones – Estrogens – Progestins • Pituitary gonadotropin hormones – Follicle stimulating hormone (FSH) – Luteinizing hormone (LH)
Female Reproductive Functions (cont’d) • Development of primary and secondary sex characteristics • Menstrual cycle
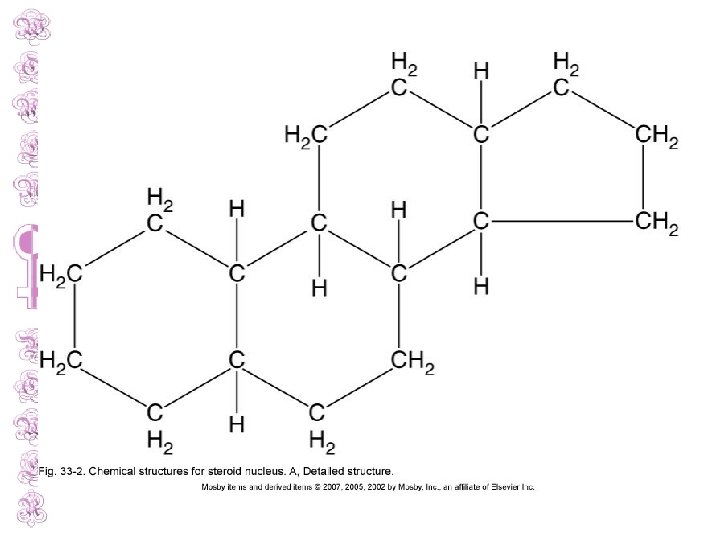
Estrogens • Three major endogenous estrogens – Estradiol (principal & most active) – Estrone – Estriol • Synthesized from cholesterol in ovarian follicles • Basic chemical structure of a steroid
Exogenous Estrogenic Drugs– Synthetic • Steroidal – Conjugated estrogens, estradiol transdermal, many others • Nonsteroidal – Chlorotrianisene, diethylstilbestrol diphosphate, others – These drugs no longer available in the United States
Estrogens Required For • The development and maintenance of the female reproductive system • The development of female secondary sex characteristics
Estrogens: Indications • Treatment of or prevention of disorders that result from estrogen deficiency – Atrophic vaginitis – Hypogonadism – Oral contraception (given with a progestin) – Dysmenorrhea – “Hot flashes” of menopause
Estrogens: Indications (cont’d) • Treatment of or prevention of disorders that result from estrogen deficiency (cont’d) – Uterine bleeding – Palliative treatment of advanced breast and prostate cancer – Osteoporosis treatment and prophylaxis – Many other indications
Estrogens: Indications (cont’d) • Continuous-combined hormone replacement therapy (CCHRT) – Fixed estrogen/progestin combination products – Reduce complications, such as endometrial hyperplasia, that occur from using estrogen alone
Estrogens: Contraindications • • • Allergy to the medication Any estrogen dependent cancer Undiagnosed abnormal vaginal bleeding Pregnancy Active thromboembolic disorder or history
Estrogens: Adverse Effects • • Thrombolytic events—most serious Nausea—most common Hypertension, thrombophlebitis, edema Vomiting, diarrhea, constipation, abdominal pain • May cause photosensitivity, chloasma
Estrogens: Adverse Effects (cont’d) • Amenorrhea, breakthrough uterine bleeding • Tender breasts, fluid retention, headaches • Others
Progestins • Synthetic derivatives of progesterone – medroxyprogesterone (Provera) – hydroxyprogesterone – megestrol (Megace) – Many others
Progestins: Indications • Treatment of functional uterine bleeding caused by: – Hormonal imbalance, fibroids, or uterine cancer • Treatment of primary and secondary amenorrhea
Progestins: Indications (cont’d) • Palliative treatment of some cancers and endometriosis • Prevention of threatened miscarriage • Alleviation of symptoms of PMS
Progestins: Indications (cont’d) • megestrol – Adjunct therapy for treatment of breast and endometrial cancers – Also used for management of anorexia, cachexia, or unexplained weight loss in AIDS patients – Used to stimulate appetite and promote weight gain in patients with cancer • Used with estrogen replacement therapy after menopause
Progestins: Adverse Effects • Liver dysfunction—cholestatic jaundice • Thrombophlebitis, thromboembolic disorders, such as PE • Nausea, vomiting • Amenorrhea, breakthrough uterine bleeding, spotting • Edema, weight gain or loss • Others
Contraceptive Drugs • Medications used to prevent pregnancy • Oral medications – Monophasic, biphasic, and triphasic forms – Most contain estrogen-progestin combinations
Contraceptive Drugs (cont’d) • Other contraceptive forms available – Long-acting injectable form of medroxyprogesterone (Depo-Provera) – Transdermal contraceptive patch – Intravaginal contraceptive ring
Contraceptive Drugs: Mechanism of Action • Prevent ovulation by inhibiting the release of gonadotropins and increasing uterine mucous viscosity, resulting in: – Decreased sperm movement and fertilization of the ovum – Possible inhibition of implantation of a fertilized egg (zygote)
Contraceptive Drugs: Other Drug Effects • Improve menstrual cycle regularity • Decrease blood loss during menstruation • Decreased incidence of functional ovarian cysts and ectopic pregnancies
Contraceptive Drugs: Indications • Primarily used to prevent pregnancy • Other uses – Treatment of endometriosis and hypermenorrhea – To produce cyclic withdrawal bleeding – Postcoital emergency contraception
Contraceptive Drugs: Adverse Effects • Drawbacks to the use of these drugs include: – – Hypertension Thromboembolism, possible PE, MI, stroke Alterations in lipid and carbohydrate metabolism Increases in serum hormone concentrations • These effects are due to the estrogen component
Contraceptive Drugs: Adverse Effects (cont’d) • May also cause: – Edema, dizziness, headache, depression, nausea, vomiting, diarrhea, increased appetite, increased weight, breast changes, many others
Contraceptive Drugs: Interactions • Drugs that decrease effectiveness of oral contraceptive drugs – Antibiotics, barbiturates, isoniazid, rifampin, griseofulvin
Contraceptive Drugs: Interactions (cont’d) • Drugs that may have reduced effectiveness if given with oral contraceptive drugs – Anticonvulsants, beta-blockers, hypoglycemic drugs, oral anticoagulants, theophylline, TCAs, vitamins, hypnotics
Osteoporosis • Low bone mass • Increased risk of fractures • Primarily affects women • 20% of those with this condition are men
Osteoporosis
Osteoporosis: Risk Factors – Caucasian/Asian descent – Slender body build – Early estrogen deficiency – Smoking – Alcohol consumption – Low-calcium diet – Sedentary lifestyle – Family history
Drug Therapy for Osteoporosis • Calcium supplements and vitamin D may be recommended for women at high risk for osteoporosis
Drug Therapy for Osteoporosis (cont’d) – Bisphonates • alendronate (Fosamax), ibandronate (Boniva), risedronate (Actonel) – Selective estrogen receptor modifier (SERM) • raloxifene (Evista) – Hormone • calcitonin • teriparatide (Forteo)
Drug Therapy for Osteoporosis (cont’d) Biphosphonates • Work by inhibiting osteoclast-mediated bone resorption, thus preventing bone loss SERMs • Stimulate estrogen receptors on bone and increasing bone density
Drug Therapy for Osteoporosis (cont’d) calcitonin – Directly inhibits osteoclastic bone resorption teriparatide – Only drug that stimulates bone formation – Derivative of parathyroid hormone – Action similar to natural parathyroid hormone
Drug Therapy for Osteoporosis: Indications • Bisphonates and calcitonin – Both prevention and treatment of osteoporosis – Biphosphanates also used for glucocorticoidinduced osteoporosis and Paget’s disease
Drug Therapy for Osteoporosis: Indications (cont’d) • raloxifene – Prevention of postmenopausal osteoporosis • teriparatide – Used for those with highest risk of fracture (prior history of fractures)
Drug Therapy for Osteoporosis Adverse Effects • SERMs – Hot flashes, leg cramps – Can increase risk of venous thromboembolism – Not used if patient is near age of menopause due to possible hot flashes – Leukopenia
Drug Therapy for Osteoporosis Adverse Effects (cont’d) • Bisphonates – Headache, GI upset, joint pain – Risk of esophageal burns if medication lodges in esophagus before reaching the stomach
Fertility Drugs • Various medical techniques used to treat infertility • Include: – in vitro fertilization – Medication therapy: ovulation stimulation
Fertility Drugs (cont’d) • clomiphene (Clomid, others) – Nonsteroidal ovulation stimulant – Blocks estrogen receptors in the uterus and brain, resulting in a false signal of low estrogen levels
Fertility Drugs (cont’d) • Clomiphene (Clomid, others) (cont’d) – Causes increased production of Gn-RH, FSH, and LH – As a result, maturation of ovarian follicles is stimulated, leading to ovulation and increased chance of conception
Fertility Drugs (cont’d) • Mentropins (Pergonal) – Standardized mixture of FSH and LH – Stimulates development of ovarian follicles, leading to ovulation – May also be given to men to stimulate spermatogenesis
Fertility Drugs (cont’d) • chorionic gonadotropin alfa (Ovidrel) – Recombinant form of human chorionic gonadotropin – Causes rupture and ovulation of mature ovarian follicles, and maintenance of corpus luteum – Used to stimulate ovulation
Fertility Drugs: Indications • Used primarily to induce ovulation in anovulatory patients • Also may be used to promote spermatogenesis in infertile men
Fertility Drugs: Adverse Effects • Tachycardia, phlebitis, DVT • Dizziness, headache, flushing, depression, anxiety, nervousness, fatigue • Nausea, bloating, constipation, others • Ovarian hyperstimulation, multiple pregnancies, blurred vision, breast pain, others
Uterine-Active Medications • Medications used to alter uterine contractions • Used to: – Promote labor – Prevent the start or progression of labor – Postpartum use: to reduce the risk of postpartum hemorrhage
Uterine Stimulants Also called oxytocics • • Ergot derivatives Prostaglandins Progesterone antagonist oxytocin (hormonal drug)
Uterine Stimulants (cont’d) Ergot alkaloids • Increase force and frequency of uterine contractions • Used after delivery of the infant and placenta to prevent postpartum uterine atony and hemorrhage • methylergonovine (Methergine)
Uterine Stimulants (cont’d) Prostaglandins • Natural hormones • Cause potent contraction of myometrium, smooth muscle fibers of the uterus • Used to induce labor by softening the cervix and enhancing uterine muscle tone • dinoprostone (Prostin E 2) and misoprostol (Cytotec)
Uterine Stimulants (cont’d) Progesterone antagonist • mifepristone (Mifeprex) • RU-486, the “abortion pill” • Stimulates uterine contractions to induce abortion • Given with a prostaglandin drug for elective abortions
Uterine Stimulants: oxytocin (Pitocin)—Synthetic Form • Used to induce labor at or near full-term gestation, and to enhance labor when contractions are weak and ineffective
Uterine Stimulants: oxytocin (Pitocin)—Synthetic Form (cont’d) • Other uses – Prevent or control postpartum uterine bleeding – Complete an incomplete abortion (after miscarriage) – Promote milk ejection during lactation
Uterine Stimulants: Adverse Effects • • • Hypotension or hypertension, chest pain Headache, dizziness, fainting Nausea, vomiting, diarrhea Vaginal pain, cramping Leg cramps, joint swelling, chills, fever, weakness, blurred vision
Uterine Relaxants: Tocolytics • Used to stop labor that begins before term to prevent premature birth • Generally used after the 20 th week of gestation
Uterine Relaxants: Tocolytics (cont’d) • Uterine contractions that occur between the 20 th and 37 th weeks of gestation are considered premature labor • Nonpharmacologic measures – Bedrest, sedation, hydration
Uterine Relaxants • ritodrine (Yutopar) and terbutaline (Brethine) – Beta-adrenergic drugs – Stimulation of beta 2 -adrenergic receptors on the uterine smooth muscle – Results in relaxation of the uterus, thus stopping premature contractions – “Off-label” use • Magnesium sulfate IV also used to stop labor
Uterine Relaxants: Adverse Effects • Palpitations, tachycardia, hypertension, others • Tremors, anxiety, insomnia, headache, dizziness, others • Nausea, vomiting, anorexia, bloating, diarrhea, constipation • Hyperglycemia, hypokalemia • Dyspnea, hyperventilation, others
Nursing Implications • Assess baseline VS, weight, blood glucose levels, renal and liver function studies • Assess whether the patient smokes • Assess history and medication history • Assess contraindications, including potential pregnancy
Nursing Implications (cont’d) • Before giving any uterine stimulants, assess the mother’s vital signs and fetal heart rate • Uterine relaxants are used when premature labor occurs between the 20 th and 37 th weeks of gestation
Nursing Implications (cont’d) • For biphosphonates, ensure that the patient has no esophageal abnormalities and can remain upright or in a sitting position for 30 minutes after the dose
Nursing Implications (cont’d) • Estrogens and progestins – Take the smallest dose needed – Give IM doses deep in large muscle masses, and rotate sites – Give oral doses with meals to reduce GI problems – Teach patient about correct selfadministration and what to do if a dose is missed
Nursing Implications (cont’d) • Estrogens and progestins (cont'd) – Increased susceptibility to sunburn may occur—advise patient to wear sunscreen or avoid sunlight – Patients should report weight gain – Annual follow-up exams should be completed, including PAP smear and breast exam
Nursing Implications (cont’d) • Follow specific administration guidelines carefully for IV administration of uterine relaxants or stimulants • Monitor the patient’s vital signs and fetal condition during therapy
Nursing Implications (cont’d) • Instruct patient taking fertility drugs to take the medication as ordered • Recommend the patient keep a journal while on fertility drugs
Nursing Implications (cont’d) • Biphosphonates – Instruct patient to take medication upon rising in the morning, with a full glass of water, and 30 minutes before eating – Emphasize that the patient should sit upright for at least 30 minutes after taking the medication
Nursing Implications (cont’d) • SERMs – Instruct patient that the medication will need to be discontinued 72 hours before and during any prolonged immobility (such as surgery or a long trip)
Nursing Implications (cont’d) • Monitor for therapeutic responses • Monitor for adverse effects