J Parkinson Antiparkinsonian drugs Abstract Assoc Prof Iv
 Assoc. Prof. Iv. Lambev E-mail: itlambev@mail. bg www. medpharm-sofia.")
J. Parkinson Antiparkinsonian drugs (Abstract) Assoc. Prof. Iv. Lambev E-mail: itlambev@mail. bg www. medpharm-sofia. eu
 is a progressive neurodege disorder. It is caused by degeneration of")
Parkinson’s disease (PD) is a progressive neurodege disorder. It is caused by degeneration of substantia nig midbrain, and consequent loss of DA-containing neurons nigrostrial pathway. Two balanced systems are important extrapyramidal control of motor activity at the level of the striatum and substantia nigra; in the first the neurotransm ACh, in the second – DA. The symptoms of PD are connected with loss of nigros neurons and DA depletion. The symptomatic triad inclu bradykinesia, rigidity and tremor with secondary manif like defective posture and gait, mask-like face and sialorr dementia may accompany.
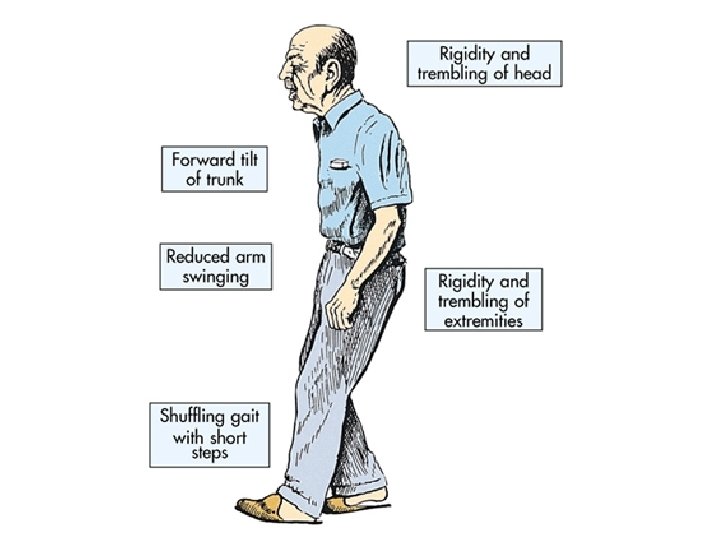

Parkinsonism
")
Clinical Pharmacology – 9 th Ed. (2003)
")
Rang et al. Pharmacology – 5 st Ed. (2003)

Distribution and characteristics of DA receptors in the central nervous system Goodman & Gilman's The Pharmacologic Basis of Therapeutics - 11 th Ed. (2

The normally high concentration of DA in the basal gangli brain is reduced in PD, and pharmacologic attempts to re DA-ergic activity with levodopa and DA agonists have bee successful in alleviating many of the clinical features of th An alternative but complementary approach has been to r normal balance of cholinergic and dopaminergic influence basal ganglia with antimuscarinic drugs. The pathophysio for this therapy is that in idiopathic parkinsonism, dopamin neurons in the substantia nigra that normally inhibit the ou GABA-ergic cells in the corpus striatum are lost. In contrast, Huntington's chorea involves the loss of som ergic neurons and an even greater loss of the GABA-ergi exit the corpus striatum. Drugs that induce parkinsonian s are DA receptor antagonists (e. g. , antipsychotic agents) w lead to the destruction of the DA-ergic nigrostriatal neuron

The cause of selective degeneration of nigrostrial neuron is not precisely known. It appears to be multifactorial. Oxi DA by MAO-B and aldehyde dehydrogenase generate hy free radicals (˙OH) in the presence of ferrous iron (basal are rich in iron). Normally these radicals are quenched by thione and other endogenous antioxidants. Age-related (e atherosclerosis) and/or otherwise acquired defect in prote antioxidant mechanisms allows the free radicals to dama membranes and DNA resulting in neuronal degenerations tic predisposition may contribute to high vulnerability of su nigra neurons. Environmental toxins or some infections (g may accentuate these defects. A synthetic toxin N-methy tetrahydropyridine (MPTP), which occurs as a contamina some illicit drugs, produces nigrostrial degenerations sim Neuroleptics and other DA blockers may cause temporar

Production of free radical by the metabolism of dopam DA is converted by MAO and aldehyde dehydrogenase (A 3, 4 -dihydroxyphenylacetic acid (DOPAC), producing hydr peroxide (H 2 O 2). In the presence of ferrous ion hydrogen oxide undergoes spontaneous conversion, forming a hydr free radical (The Fenton reaction). Goodman & Gilman's The Pharmacologic Basis of Therapeutics - 11 th Ed. (2
 Factors contributing to")
Grippe Essential of Medical Pharmacology – 5 st Ed. (2003) Factors contributing to degeneration of nigrostrial DA-ergic neurones causing PD

The key steps in the synthesis and degradation of dopamine and the sites of action of various psychoactive substances at the dopaminergic synapse

Objectives of antiparkinsonian pharmaco The dopaminergic/cholinergic balance may be restored by two mechanisms. 1. Enhancement of DA-ergic activity by drugs which m (a) replenish neuronal DA by supplying levodopa, which is its natural precursor; administration of DA itself is ineffective as it does not cross the BBB; (b) act as DA agonists (bromocriptine, pergolide, cabergo (c) prolong the action of DA through selective inhibition o metabolism (selegiline); (d) release DA from stores and inhibit reuptake (amantad 2. Reduction of cholinergic activity by antimuscarinic drugs; this approach is most effective against tremor and less effective in the treatment of bradykinesia.
 Selegiline MAO-B (-) Amantadine Reuptake Amantadine (+) The")
Central DA-ergic Drugs Levodopa Dopamine (-) Selegiline MAO-B (-) Amantadine Reuptake Amantadine (+) The Principles of Medical Pharmacology (1994) D 2 -receptors Bromocriptin Pergolide
 is a")
▼LEVODOPA (DOPA – Dihydro. Oxy. Phenyl. Alanine; (t 1/2 1, 5 h) is a natural amino acid precursor of DA. The major disadvantage is the extensive decarboxylation of levodopa to DA in periferal tissues. So that only 1– 3% of an oral dose reaches the brain.
")
Basic & Clinical Pharmacology – 10 th Ed. (2007)

Thus large quantities of levodopa would have to be given Levodopa and its metabolites cause significant adverse r (ARs) by peripheral actions, notably nausea, arrhythmia, hypotension. This problem has been largely circumvented decarboxylase inhibitors (benserazide, carbidopa), whi not enter the CNS; they prevent only the extracerebral m of levodopa. The inhibitors are given in combination with levodopa; but in this case only 25% of the dose of levodo required and ARs diminish significantly. Levodopa alone combination is introduced gradually and titrated according clinical response; the dose being altered every two weeks • Co-careldopa (carbidopa and levodopa in proportions 12. 5/50 mg, 25/100 mg, 25/250 mg) – Sinemet®. • Co-beneldopa (benserazide and levodopa in proportion 12. 5/50 mg, 25/100 mg, 50/200 mg) – Madopar®.
")
Basic & Clinical Pharmacology – 10 th Ed. (2007)
 – a derivative of ergot (Ergot de savle, Secale")
▼BROMOCRIPTINE (t 1/2 5 h) – a derivative of ergot (Ergot de savle, Secale cornutum). It is a D 2 -receptor agonist, but also a weak alpha-adrenoceptor anatagonist. Bromocriptine is monly used with levodopa. It should be started at very low doses (1– 1, 25 mg p. o. at night), increasing at weekly inte and according to clinical response. It is also used for trea of prolactin-secreting adenomas, amenorrhea/galactorrhe hyperprolactinemia, to stop lactation, acromegaly. ADRs: Nausea and vomiting, which may be prevented w domperidone; postural hypotension (may cause dizziness syncope); after prolonged use – pleural effusion and retroperitoneal fibrosis.

▼CABERGOLINE, also an ergot derivative, has a t 1/2 > This allows it to be used in a single daily (or even twice dose. Cabergoline alleviates night-time problems in par nian patients due to lack of levodopa. ▼PRAMIPEXOLE is a non-ergot D 2 -receptor agonist; i more effective against tremor than the others. ▼ROPINIROLE (Requip®) is a new non-ergot direct D 2 -receptor agonist. There are insufficient data to allow an informed choice between pramipexole and ropinirole ▼ENTACAPONE inhibits COMT (Catechol-Ortho-Meth pherase), one of the main enzymes responsible for the metabolism of DA; the action of levodopa is thus prolon Entacapone is most effective for patients with early end-of-dose deterioration.

▼SELEGILINE. The problem with nonselective MAO inh that they prevent degradation of dietary adrenomimetic a especially tyramine, by MAO-A inhibition which causes hypertensive “cheese reaction”. Selegiline does not cause the cheese reaction, because MAO-A is still presented in the liver to metabolize tyrami MAO-A also metabolizes tyramine in the sympathetic ne endings in periphery. Selegiline inhibits selectively an irreversibly only MAO-B in the CNS and protects DA from intraneuronal degradation. It is used as an adjunct drug in PD if levodopa/carbidop levodopa/benserazide therapy is deteriorating. In a transdermal patch selegiline is used as a treatment for major depression.

▼AMANTADINE is an antivirus drug which, given for influ to a parkinsonian patient, was noted to be beneficial. Anti and antiparkinsonian effects of amantadine are probably unrelated. Antiparkinsonian effect is due to increase synthesis and release of DA, and diminish neuronal reuptake too. Amantadine also has slight antimuscarinic effect. It is used for oral adjunct treatment of PD and influenza A virus infection. Amantadine is relatively free from ARs, which, however, includes ankle edema (probably a local effect on blood vessels), orthostatic hypotension, insomnia, hallucinations, rarely – fits.
 Radix Belladonnae: (cura bulgara) –")
Central antimuscarinic drugs Atropa belladonna L. (Deadly night shade) Radix Belladonnae: (cura bulgara) – atropine Belladonna roots have been empirically used for treatment of PD in 1920 s in Bulgaria by healer Ivan Raev (Sopot: 1876– 1938).
. They parkinsonism by blocking ACh receptors")
▼BIPERIDEN, TRIHEXYPHENIDYL, TRIPERIDEN are synthetic compounds (central M-cholinolytics). They parkinsonism by blocking ACh receptors in the CNS, the partially redressing the imbalance created by decreased activity. They also produce modest improvement in tre rigidity, sialorrhoea (hypersalivation), muscular stiffnes cramp, but little in bradykinesia, which is the most disabl symptom of Parkinson’s disease. ARs of antimuscarinic include dry mouth (xerostomia), blurred vision, constipati urine retention, glaucoma, hallucinations, memory defects, toxic confusional states and psychoses (which should be distinguish from presenile dementia). Trihexyphenidyl
 The main features")
Pharmacotherapy of PD (Clinical Pharmacology – 9 th Ed. , 2003) The main features that require alleviation are tremor, rig and bradykinesia. Drug therapy has the most important symptom relief, but it does not alter the progressive cour Treatment should begin only when it is judged necessary each individual case. Two conflicting objectives have to be balanced: the desire for satisfactory relief of current s and the avoidance of ARs as a result of long-continued t There is a debate as to whether the treatment should co with levodopa or a synthetic DA agonist. Levodopa provi the biggest improvement in motor activity but its use is a with the development of dyskinesia (involuntary moveme of the face and limbs) after 5– 10 years, and sometimes s

DA agonists have a much less powerful motor effect but likely to produce dyskinesias. The treatment usually beg levodopa in low doses to get a good motor response and a DA agonist when the initial benefit begins to wane. A typical course is that for about 2– 4 years on treatment levodopa or DA agonist, the patient’s disability and moto performance remains near normal despite progression o underlying disease. After some 5 years about 50% of pa exhibit problems of long-term treatment, namely, dyskine and end-of-dose deterioration with the “on-off” phenome After 10 years virtually 100% of patients are affected.

End-of-dose deterioration is managed by increasing the frequency of dosing with levodopa (e. g. to 2 or 3 -hourly) this tends to worsen the dyskinesia. The motor response becomes more brittle with abrupt swings between hyper hypomobility (the on-off phenomenon). In this case a mo effective approach is to use a COMT inhibitor, e. g. entac which can sometimes allay early end-of-dose deteriorati without causing dyskinesia. Some 20% of the patients with Parkinson’s disease, nota Elderly ones, develop impairment of memory and speec fluctuating confusional state and hallucinations. As these symptoms are often aggravated by medication, it is prefe gradually to reduce the antiparkinsonian treatment.

Antimuscarinic drugs are suitable only for younger patien minantly troubled with tremor and rigidity. They do not be dyskinesia, the main disability symptom. The ARs of acut glaucoma, retention of urine, constipation and psychiatric bance are general contraindications to their use in the eld Drug-induced Parkinsonism is alleviated by antimuscarin not by levodopa or DA agonist, because antipsychotics b D 2 -receptors by which these drugs act. The piperazine phenothiazines (e. g. trifluoperazine) and butyrophenones (e. g. haloperidol) often cause Parkinsonism because they D 2 -receptors.

Treatment approaches to newly diagnosed idiopathic PD

Comparison of levodopa + benserazide, levodopa + benserazide + selegiline and bromocriptine on progression of PD symptoms
- Slides: 32