Medical University of Sofia Faculty of Medicine Department



")



 • keep regular bedtimes and rising")


 – on the green Rp b Bromazepam,")
 is probably the most important inhibitory transmitter in the CNS.")

 Zolpidem, Zopiclone s Z BD te si + GABAAsite +")
 • Flurazepam (t 1/2")


")
")


")






")



 promotes elimination of the drug. Urine")



")
- Slides: 39
Medical University of Sofia, Faculty of Medicine Department of Pharmacology and Toxicology HYPNOTICS Assoc. Prof. I. Lambev E-mail: itlambev@mail. bg
Insomnia is characterized by the complaint of poor sleep, with difficulty either in initiating sleep or maintaining sleep throughout the night. It can occur exclusively in the course of another physical disorder such as pain, mental disorder, e. g. depression, or sleep disorder, e. g. sleep apnoea. In a large proportion of patients it is a primary sleep disorder and causes significant impairment in social, occupational or other important areas of functioning. One survey showed similar deficits in quality of life in insomniacs as in patients with long-term disorders such as diabetes. About 60% of patients with insomnia have abnormal sleep.
Transmitters: waking state and sleep. During the sleep dominates GABA. Lüllmann, Color Atlas of Pharmacology – 2 nd Ed. (2000)
Lüllmann, Color Atlas of Pharmacology – 2 nd Ed. (2000)
Normal hypnogram
Effect of hypnotics on proportion of REM/NREM Lüllmann, Color Atlas of Pharmacology – 2 nd Ed. (2000)
Transmitters: waking state and sleep Lüllmann, Color Atlas of Pharmacology – 2 nd Ed. (2000)
Sleep hygiene (adapted from Bennett and Brown, 2003) • keep regular bedtimes and rising times • daytime (but not evening) exercise and exposure to daylight • avoid stimulants, alcohol and cigarettes in evening • establish bedtime routine — 'wind down' — milk drink may be helpful • avoid dwelling on problems in bed • bed should be comfortable and not too warm or too cold.
In the treatment of long-term insomnia the most important factor is anxiety about sleep, arising from conditioning behaviors that predispose to heightened arousal and tension at bedtime. Thus the bedroom is associated with not sleeping and automatic negative thoughts about the sleeping process occur in the evening. Cognitive behavioral therapy is helpful in dealing with 'psychophysiological insomnia and together with education and sleep hygiene measures as above is the treatment of choice for long-term primary insomnia. Cognitive behavioral therapists are specially trained in changing behavior and thoughts about sleep, particularly concentrating on learned sleep-incompatible behaviors and automatic negative thoughts at bedtime.
TREATMENT OF INSOMNIA Timely treatment of short-term insomnia is valuable, as it may prevent progression to a chronic condition, which is much harder to alleviate. Psychological treatments are effective and pharmacotherapy may be either unnecessary or used as a short-term adjunct. The approaches are to: 1. Treat any precipitating cause 2. Educate about trigger factors for sleep and reassure that sleep will improve 3. Establish good sleep hygiene 4. Consider hypnotic medication
IL® CLASSIFICATION OF HYPNOTICS 1. Benzodiazepines (euhypnotics) – on the green Rp b Bromazepam, Flurazepam, Flunitrazepam Nitrazepam, Midazolam, Triazolam etc. 2. Benzodiazepine like drugs (euhypnotics, Z-drugs) Zaleplon, Zolpidem, Zopiclone 3. Barbiturates • Very short-acting (i. v. anaesthetics): Methohexital, Thio • Intermediate-acting barbiturates: Cyclobarbital, Secoba • Long-acting: Phenobarbital (t 1/2 96 h) 4. H 1 -blockers – I generation: Diphenhydramine, Promet 5. Piperidinеdiones: Gluthetimide 6. Some Phenothiazines: Thioridazine 7. Combinations: Reladorm (cyclobarbital/diazepam) 8. Herbal preparations: Valerian, Dormiplant , Re. Dormin
Gamma aminobutyric acid (GABA) is probably the most important inhibitory transmitter in the CNS. GABA-ergic neurones are distributed widely in the CNS. GABA controls the state of excitability in all brain areas and the balance between excitatory inputs (mostly glutamatergic) and the inhibitory GABA-ergic activity. If the balance swings in favour of GABA, then sedation, amnesia, muscle relaxation and ataxia appear and nervousness and anxiety are reduced. The mildest reduction of GABA-ergic activity elicits arousal, anxiety, restlessness, insomnia and exaggerated reactivity.
Most drugs used in insomnia act as agonists a t t h e G A B AA - r e c e p t o r and have effects other than their direct sedating action, including muscle relaxation, memory impairment, and ataxia, which can impair performance of skills such as driving. Clearly those drugs with onset and duration of action confined to the night period will be most effective in insomnia and less prone to unwanted effects during the day. Those with longer duration of action are likely to affect psychomotor performance, memory and concentration; they will also have enduring anxiolytic and muscle-relaxing effects.
G ABA Benzodiazepines (BDZs) Zolpidem, Zopiclone s Z BD te si + GABAAsite + + Cl+ Barbitu- rate sate Ethanol Adapted from Bennett and Brown, Clinical Pharmacology – 9 th Ed. (2003) Barbiturates
The most used BENZODIAZEPINES • Bromazepam (t 1/2 20 h) • Flurazepam (t 1/2 > 40 h) • Flunitrazepam (t 1/2 15 h) • Nitrazepam (t 1/2 26 h tab. 5 mg) • In anaesthiology • Diazepam (long t 1/2) • Midazolam (t 1/2 2 h) • Triazolam (t 1/2 3 h)
When GABA binds with the GABAA-receptor, the permeability of the central pore of the receptor to chloride ions increases, allowing more ions into the neurone and decreasing excitability. Classical benzodiazepines (BDZs) in clinical use enhance the effectiveness of GABA by lowering the concentration of GABA required for opening the channel. These drugs are agonists at the receptor and there is an antagonist (flumazenil) which prevents agonists from binding at the receptor site and enhancing GABA function.
A model of the GABAA receptor-chloride ion channel macromolecular complex Basic & Clinical Pharmacology – 10 th Ed. (2007)
BDZs enhance GABA-ergic inhibition. Lüllmann, Color Atlas of Pharmacology – 2 nd Ed. (2000)
Lüllmann, Color Atlas of Pharmacology – 2 nd Ed. (2000)
All BDZs and newer benzodiazepine-like drugs are safe and effective for insomnia, if the compound with the right timing of onset of action and elimination is chosen. However, care should be taken in prescribing them to patients with co-morbid sleep-related breathing disorders such as obstructive sleep apnoea syndrome, which is exacerbated by BDZs. Objective measures of sleep show that BDZs decrease time to sleep onset and waking during the night; subjective effects of improved sleep are usually greater than the objective changes, probably because of their anxiolytic effects.
Pharmacokinetics BDZs are effective after administration by mouth but enter the circulation at very different rates that are reflected in the speed of onset of action, e. g. alprazolam is rapid, oxazepam is slow. The liver metabolizes them, usually to inactive metabolites, but some compounds produce active metabolites, some with long t 1/2 which greatly extends drug action, e. g. chlordiazepoxide, clorazepate and diazepam.
Biotransformation of benzodiazepines Lüllmann, Color Atlas of Pharmacology – 2 nd Ed. (2000)
Uses • Benzodiazepines are used for: insomnia, anxiety, alcohol withdrawal states, muscle spasm due to a variety of causes, including tetanus and cerebral spasticity, epilepsy (clonazepam), anaesthesia and sedation for endoscopies and cardioversion. • The choice of drug as hypnotic and anxiolytic is determined by pharmacokinetic properties.
Tolerance to the anxiolytic effects does not seem to be a problem. In sleep disorders the situation is not so clear; studies of subjective sleep quality show enduring efficacy but about half of the objective (EEG) studies indicate decreased effects after 4– 8 weeks, implying that some tolerance develops. The necessity for dose escalation in sleep disorders is rare. Dependence. Animal and human research has shown that brain receptors do change in character in response to chronic treatment with BDZs and therefore will take time to return to premedication levels after cessation of medication.
Features of withdrawal and dependence vary. Commonly there is a kind of psychological dependence based on the fact that the treatment works to reduce patients' anxiety or sleep disturbance and therefore they are unwilling to stop. If they do stop, there can be relapse, where original symptoms return. Withdrawal of BDZs should be gradual after as little as 3 weeks' use but for long-term users it should be very slow, e. g. about 6– 12 weeks. Withdrawal should be slowed if marked symptoms occur and it may be useful to substitute a long t 1/2 drug (e. g. diazepam) to minimize rapid fluctuations in plasma concentrations. In difficult cases withdrawal may be assisted by concomitant use of an antidepressant.
Adverse effects In addition to those given above, BDZs can affect memory and balance. Hazards with car driving or operating any machinery can arise from amnesia and impaired psychomotor function, in addition to sleepiness (warn the patient). Amnesia for events subsequent to administration occurs with i. v. high doses, for endoscopy, dental surgery (with local anaesthetic), cardioversion, and in these situations it can be regarded as a blessing. Women (1 in 200), may experience sexual fantasies, including sexual assault, after large doses of BDZs as used in some dental surgery, and have brought charges in law against male staff.
Plainly a court of law has, in the absence of a witness, great difficulty in deciding whom to believe. Paradoxical behavior effects and perceptual disorders, e. g. hallucinations, can occur. Headache, giddiness, GI upset, skin rashes and reduced libido can occur. Extrapyramidal reactions, reversible by flumazenil, are rare. The PRC of BDZs is D. BDZs cross the placenta and can cause fetal cardiac arrhythmia and muscular hypotonia, suckling hypothermia and respiratory depression in the new born.
Interactions All BDZs potentiate the effects of alcohol and other central depressants, and all are likely to exacerbate breathing difficulties where this is already compromised, e. g. in obstructive sleep apnoea. BDZs potentiate the action of analgetics too. The fluoroquinolones block BDZs receptors and decrease the action of BDZs. Overdose. Flumazenil (Anexate®) selectively reverses benzodiazepine effects and is useful in diagnosis and in treatment of intoxication with them. Flumazenil is a competitive partial agonist.
Fluoroquinolones Adapted from Bennett and Brown (2003)
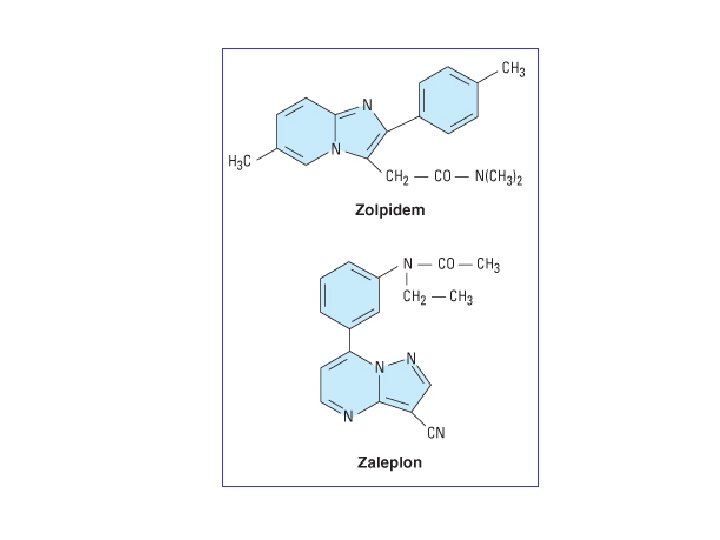
Nonbenzodiazepine hypnotics that act at the GABAA-benzodiazepine receptor Zopiclone is a cyclopyrrolone in structure. It has a fairly fast (about 1 h) onset of action which lasts for 6– 8 h, making it an effective drug both for initial and maintenance insomnia. It may cause fewer problems on withdrawal than BDZs. Its duration of action is prolonged in the elderly and in hepatic insufficiency. About 40% of patients experience a metallic aftertaste. Care should be taken with concomitant medication that affects its metabolic pathway. The dose is 3. 75– 7. 5 mg p. o. Zolpidem is an imidazopyridine in structure and has a fast onset (30– 60 min) and short duration of action. Patients over 80 years have slower clearance of this drug.
Barbiturates have a low therapeutic index, i. e. relatively small overdose may endanger life; they also cause dependence and have been popular drugs of abuse. Lüllmann, Color Atlas of Pharmacology – 2 nd Ed. (2000)
The use of intermediate-acting drugs (cyclobarbital, se is now limited to severe intractable insomnia in patients a taking barbiturates (they should be avoided in the elderly The long-acting phenobarbital is used for epilepsy, and very short-acting thiopental and methohexital for ana The barbiturates are enzyme inducers. They can cau in children and osteomalacia in elderly. They cross the pl and have teratogenic activity (PRC: D). The phenobarbi may produce tolerance and drug dependence. Overdose following self-poisoning by barbiturates m severe features including hypotension (may lead to renal hypothermia, respiratory depression and coma. Supportiv sures may suffice with i. v. fluid to restore central venous and so cardiac output and, if that fails, using a cardiac dru
A good urine volume (e. g. 200 ml/h) promotes elimination of the drug. Urine alkalinisation accelerates removal of phenobarbital (an acid, p. Ka 7. 2) as do repeated doses of activated charcoal. Active elimination by haemoperfusion or dialysis may be needed in particularly severe and complicated cases. Antihistamines. Promethazine has a slow (1– 2 h) onset and long (t 1/2 12 h) duration of action. It reduces sleep onset latency and awakenings during the night after a single dose but there have been no studies showing enduring action. It is sometimes used as a hypnotic in children. There are no controlled studies showing improvements in sleep after other antihistamines.
Barbiturates, glutethimide, and meprobamate should be avoided for the management of insomnia. They have high abuse potential and are dangerous in overdose (Charney et al. : GOODMAN & GILMAN'S THE PHARMACOLOGICAL BASIS OF THERAPEUTICS. 11 th Ed. (2006)
Melatonin is the hormone produced by the pineal gland during darkness, has been investigated for insomnia but it appears to be ineffective. The impressive nature of the diurnal rhythm in melatonin secretion has stimulated interest in its use therapeutically to reset circadian rhythm to prevent jet-lag on long-haul flights and for blind or partially sighted people who cannot use daylight to synchronize their natural rhythm. There is controversy about dose and timing of treatment and in most countries pharmaceutical preparations are not generally available.
Herbal preparations Randomized clinical trials have shown some effect of valerian in mild to moderate insomnia, and hops, lavender and other herbal compounds show promise in pilot studies that are presently being pursued more fully. The valerian extract contain valeopotriates, which possesses GABA-mimetic action. Dormiplant® (coat tabl. ) contain ethanol extract: Rad. Valerianae 160 mg and fol. Mellissae 80 mg. It possesses sedative and hypnotic effect. Re. Dormin®, Benosen®
Valeriana officinalis Leonurus cardiaca Съвременна фитотерапия (1972)