Medical University of Sofia Faculty of M Department



 may modify the perception o and remove the")
. It causes the release of")

 tran principally")

 input (e.")


 •")


:")

 enkephalins activate μ and δ-receptors b) endorphins activate μ,")

 and biliary tract spa Bronchospasm Retentio")






 i. m.")
 Similar action to morphine More active than morphine More")

 Almost identical to morphine Tends to cause")



 Less")
 is structural to methadone and differs in that it")
 with remar very high potency, more than")


 Naltrexone (μ, κ and δ-antagonist) Nalorphine")
- Slides: 40
Medical University of Sofia, Faculty of M Department of Pharmacology and Toxico OPIOID ANALGESICS © Assoc. Prof. Ivan Lambev E-mail: itlambev@mail. bg
Pain is the most common symptom for which pa see a doctor. Different types of drugs are used fo treatment of pain. In general, they include: 1. Drugs, relieving pain due to multip causes (analgesics) Ø narcotic analgesics (morphine, fentanyl etc): act chiefly in the CNS Ø non-narcotic analgesics (paracetamol, metam act chiefly peripherally
2. Drugs, relieving pain due to a sing cause or specific pain syndrome only They are not classified as analgesics: e. g. naratriptan (migraine), carbamazepine (neuralgias), glyceryl trinitrate (angina pectoris), adrenal steroids (inflammatory pain), butylscopolamine (spasm of visceral smooth muscles), baclofen (spasm of striated muscl
3. Adjuvant drugs (anxyolitics, neuroleptics antidepressants) may modify the perception o and remove the concomitants of pain such as fear, depression. Placebo gives relief in 3%. 4. Anaesthetics (general and local) are use during surgical operations, some diagnostic and other painful procedures.
Nociception is a consequence of tissue injur (trauma, inflammation). It causes the release of chemical mediators (ACh, PGE, NA, 5 -HT, glutamate, bradykinin, endogenous opioids, adenosine). They have neuronal or non-neurona origin. These mediators activate nociceptors. Nociceptors are pain-receptors. Nocice transmit information by thin myelin (A-delta) and non myelin (C) fibers to the spinal cord and
Pain perception has a complex mechanism It is a result of nociceptive impulses reaching the brain (thalamus, cortex), plus impulses from other peripheral receptors, e. g. heat and mechanoceptors, whose threshold of response is reduced by the same chemical mediators. These are processed in the brain whence modulated inhibitory impulses pass down to regulate the continuing afferent input. But pain can occur without nociception (e. g. some neuralgias). Pain is a psychological though most types of pain have a physical cause
MAIN TYPES OF PAIN Acute pain (defined as < 3 months duration) tran principally by fast conducting myelin A-delta fibers major nociceptive input (physical trauma, pleurisy, myocardial infarction, perforated peptic ulcer). The narcotic (opioid) and sometimes non-narcotic analgesics are used for treatment of acute pain.
Chronic pain (defined as > 3 months duratio transmitted principally by slow conducting non myelin C fibers. It is better regarded as a syndrome rather than symptom. It is depressing to the patient who sees no prospect for relieving the suffering. Analgesics alone are often insuffici and adjuvant drugs (antidepressants or neurolep as well as non drug therapy (including psychoth have increasing importance.
Neuropathic pain follows damage of the nervous Acute pain without nociceptive (afferent) input (e. g neuralgias) is less susceptible to analgesics. The drugs are some antidepressants and carbamazep Transient pain is provoked by activation of nocice skin and other tissues in absence of tissue damag It protects humans from physical damage coming environment or excessive stressing of tissue. It is of normal life and does not need treatment.
HISTORY Opium is the dried juice of seed head of poppy. It wa in prehistorical times (e. g. in Egypt, Ebers’papirus – b. n. c) as analgesic, tranquillizer, antitussive drug a treating of diarrhoea. The principal active ingredient opium – morphine, was isolated in 1806 from Freder Sertűrner, who tested pure drug on himself and three young men. He observed that morphine caused cere depression and relieved toothache. Gay Lussac nam drug, which was the first discovered alkaloid, after Morpheus (the son of Somnus) – morphine.
Poppy
Opium contains two groups of alkaloids: • with phenantrene structure (morphine, codeine, thebaine) • with isochinoline structure (papaverine, noscap Morphine and codeine are narcotic analgesic; papaverine is a vasodilator; noscapine is antitus agent which is suspected of genotoxicity. Opium contains ≈10% morphine.
Some terminology OPIOID: produces morphine-like effects. OPIATE: has a morphine-like structure. Opioid is the preferred modern term.
Opioids can be divided into two groups: - Morphine analogues – with structure similar to morphine - Synthetics – with structure unrelated to morphine methadone
Mechanism of actions of opioid analgesics Effects are mediated via opioid recep m (mu): mediate analgesia at the supraspinal level d (delta): analgesia in the periphery k (kappa): analgesia at the spinal leve ORL 1 (opioid receptor like 1): depend
There are endogenous analgesic substances with peptide structure and morphinolike action. They are called endogenous pept and was discovered during the investigation of mechanism of analgesic action of morphine.
Endogenous opioid peptides a a) enkephalins activate μ and δ-receptors b) endorphins activate μ, κ and δ-recepto c) dynorphins activate μ, κ and δ-recepto d) nociceptin – ORL 1 (tolerance) Opioid peptides act in CNS as: - neurotransmitters - modulators of response (usually inhibito
The main effects of morphine ar on the CNS Depression, leading to analgesia, respiratory depression (decrease in sensitiv of the respiratory centre to PCO 2), depressi of cough reflex, sleep) Excitation, leading to vomiting, miosis (pupil constriction), convulsions (very rare) Changes of mood – euphoria (sense of well being) or dysphoria. Tolerance and dependence (psychological and physical)
Smooth muscle stimulation Gastrointestinal muscle spasm (with constipation) and biliary tract spa Bronchospasm Retentio urinae Cardiovascular system Dilation of resistance and capacitance vessels Other effects Sweating, histamine release, pruritus, piloeraction, antidiuretic effect
Phenomenon of Stra
Tolerance and dependence Tolerance it is increasing dose of drug required to produce the same effect. It occurs rapidly with opioids (with morphine 12– 24 hours, e. g. hot plate test – in mice, after 3 days dose of morphine required for analgesia increases 5 -fold). Important in drug addiction – may need to increase dose 50 -fold.
Tolerance is not shown equally on all effects. Tolerance extends to: analgesia euphoria resp. depression To much less extent on: constipation pupil constriction This is why constipation can be such a big problem with opioids
Why does tolerance occur? There are several potential reasons: - Increased metabolism of the drug - Decreased receptor affinity
DEPENDENCE Takes two forms : physical psychological Physical dependence – problems include withdrawal syndrome (addiction): - Irritability - Weight loss - Shakes - Sweating - Piloeraction “cold turkey” - Effects last off in 8– 10 days
Psychological dependence Problems are: - Desire for the drug - Want to experience the “rush” – positive - Don’t want the withdrawal – negative - Some opioids e. g. codeine & pentazocine are much less likely to cause dependence
Morphine and its analogues Morphine Hydrochloride 1% 1 ml (= 10 mg) i. m. Morphine Sulphate (Sulfate): 1 tab. /12 h p. o. (depot-effect Codeine: 10– 20 mg/dose Dihydrocodeine: 1 tab. /12 h p. o. (depot-effect Oxycodone: p. o.
HEROIN (diamorphine – BAN, diacetylmorphine) Similar action to morphine More active than morphine More lipid soluble – crosses BBB faster to give greater rush Shorter duration of action than morphine
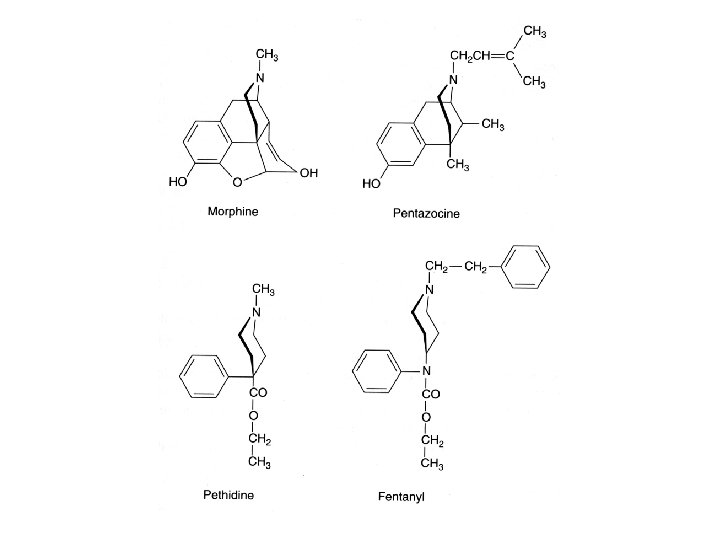
Synthetic derivatives PHENYLPIPERIDINES pethidine, fentanyl METHADONES methadone, dextropropoxyphene BENZOMORPHANS pentazocine THEBAINES buprenorphine, etorphine
PETHIDINE (Meperidine – USAN; Lydol® – Sopharma) Almost identical to morphine Tends to cause restlessness rather than sedation Antimuscarinic effects: dry mouth blurred vision Less antitussive Shorter duration of action (4 -6 h) – preferred in labour
FENTANYL >80 times more potent than morphine in analgesia Main use is in anaesthesia, used in conjunction with droperidol to produce neuroleptanalgesia Effentora® – buccal tablets from 100 to 800 mcg, used in cancer BTP (breakthrough pain) Durogesic®: TTS/72 h
Durogesic TTS
NEUROLEPTANALGESIA • Fentanyl 100 mcg + • Droperidol 5 mg i. m. Similar to Fentanyl: • Alfentanil (NB: without “y”) • Sufentanil (NB: without “y”)
METHADONE Similar actions to morphine Longer duration of action (t 1/2 37 h) Less problems withdrawal Can be used to wean heroin and morphine addicts off the drug
DEXTROPROPOXYPHENE (t 1/2 5 h) is structural to methadone and differs in that it is less analgesi less dependence producing. It is weak μ/κ/δ-agon analgesics usefulness approximates to that of cod but its duration of action is longer.
Pentazocine – κ/δ-agonist/weak μ-antagon ETORPHINE (strong μ/κ/δ-agonist) with remar very high potency, more than 1000 times that a mor It is used to immobilize wild animals for trapping an research purposes, since require dose, even for an elephant, is small enough to be incorporated into a dart or pellet.
Low efficacy for mild and moderate codeine, dihydrocodeine, dextropropoxiphe oxycodone, pentazocine High efficacy for severe pain alfentanil, buprenorphine, heroin, fentanyl, methadone, morphine, pethidine, sufentanil, tramadol Tramadol – partial μ-agonist, inhibitor of NA and 5 -HT reuptake.
OPIOID COMPETITIVE ANTAGONISTS Naloxone (μ, κ and δ-antagonist) Naltrexone (μ, κ and δ-antagonist) Nalorphine (Allylnormorphine) μ-antagonist/κ-agonist)