Lower Gastrointestinal Tract KNH 411 2007 Thomson Wadsworth












, low-fat 45")
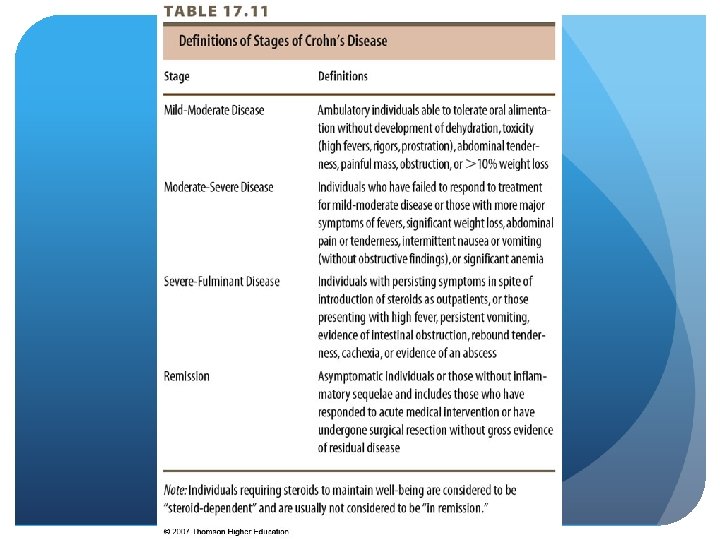
 Abdominal pain with two of the")




 Assess")


![Pathophysiology: Lower GI Tract IBD - Nutrition Therapy] Antibiotics May require nut support, TPN](https://slidetodoc.com/presentation_image_h2/06037f5cdbac8f7ccd2bee059b7954e9/image-31.jpg "Pathophysiology: Lower GI Tract IBD - Nutrition Therapy] Antibiotics May require nut support, TPN")







- Slides: 39
Lower Gastrointestinal Tract KNH 411
© 2007 Thomson - Wadsworth
Pathophysiology: Lower GI Tract Malabsorption - maldigestion of fat, CHO, Protein Number one concern Decreased villious height, enzyme production Decreased transit time- recesting, surgury can alter or stress the GI Might need time to recover- Chrons, CD, diverticulitis Disfunction of an accessory organ
Pathophysiology: Lower GI Tract Malabsorption - fat Steatorrhea- fat travels undigested and malabsorbed , ADEK a concern, worry about kidney stones Fat-soluble vitamins malabsorbed Potential for excess oxalate(kidney stones) Abdominal pain, cramping, diarrhea Dg; fecal fat test or D-xylose absorption test, or small bowel x-ray
Pathophysiology: Lower GI Tract Malabsorption - Fat – Nutrition Restrict fat 25 -50 g/day= #1 Use of MCT supplements- medium chain triglycerides- must be shorted chain, body cannot activate enzymes and cab absorbed right into the system. Give gut a rest Pancreatic enzymes Chrones- take before their meals
Pathophysiology: Lower GI Tract Malabsorption - CHO Lactose malabsorption Increased gas, abdominal cramping, diarrhea Restrict milk and dairy products Diagnosed by lactose tolerance test- breath test Products such as Lactaid can be rec.
Pathophysiology: Lower GI Tract Malabsorption - protein Protein-losing enteropathy- excess of protein loss Reduced serum protein (shows in this lab value) Short term uses pre albumin Peripheral edema- Cells cannot hold water, fluid overloaded
Pathophysiology: Lower GI Tract Malabsorption - Nutrition Therapy Results in weight loss, loss of vit/ min Chronic PEM (protein energy malnutrition) Treat underlying disease/ nutrient being malabsorbed Amino acid formula Simple carbs Short chain triglycerides
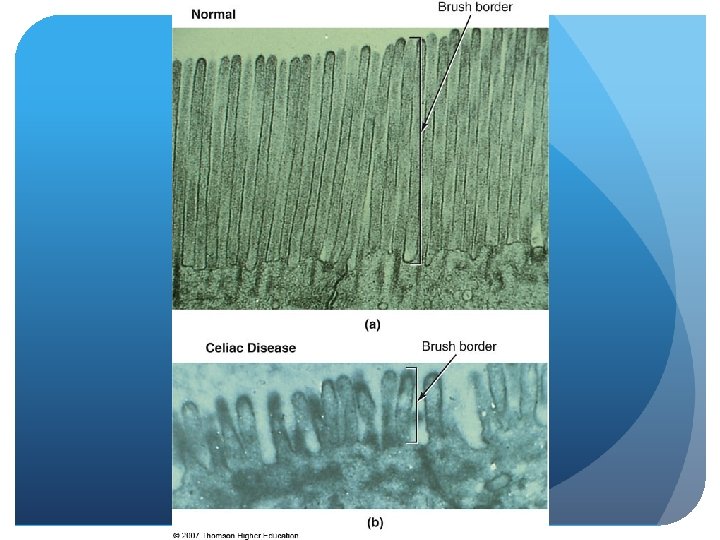
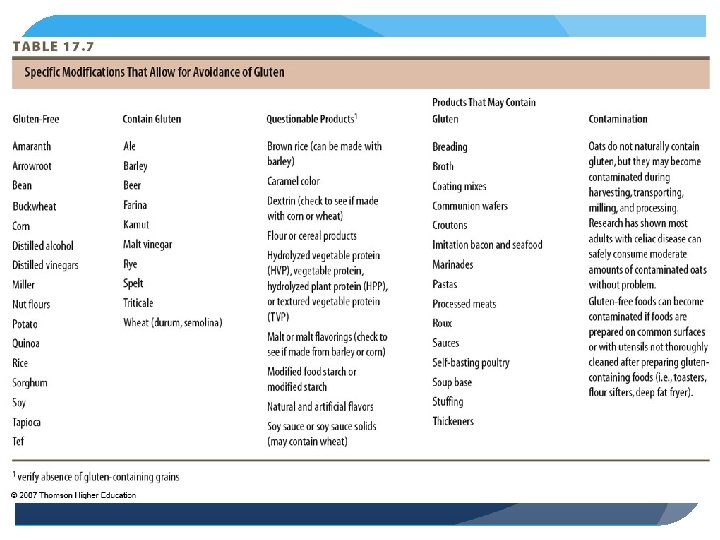
Pathophysiology: Lower GI Tract Celiac disease Genetic and autoimmune Occurs when wheat rye barely is eaten (oats can be contaminated as well) Inflammatory state that creates antibodies Occurs when alpha-gliadin from wheat, rye, malt, barley are eaten Infiltration of WBC, production of Ig. A antibodies
Pathophysiology: Lower GI Tract Celiac disease - pathophysiology Damage to villi Decreased enzyme function Maldigestion and malabsorption Occurs with other autoimmune disorders- type 1 diabetes, r. arthritis, psorisis
Pathophysiology: Lower GI Tract Celiac disease - clinical manifestations Bone and joint pain, mouth sores Diarrhea, abdominal pain, cramping, bloating, gas Muscle cramping, fatigue Skin rash Higher risk for lymphoma and osteoporosis
Pathophysiology: Lower GI Tract Celiac Disease - Diagnosis/Treatment/Prognosis Biopsy of small intestinal mucosa Reversal of symptoms following gluten-free diet Refractory CD; d/t coexisting disease
Pathophysiology: Lower GI Tract Celiac Disease - Nutrition Intervention Low-residue (min diarrhea), low-fat 45 -50 g no more, lactosefree, gluten-free diet Identify hidden sources of gluten Specialty products Oats controversial- no more than 1/2 cup per day Much easier for individuals So many not CD are using this diet Of course you lose weight, its an elimination diet (eliminating calories), physiological effect, lose a lot of B complex/ fiber Make sure to supplement with B complex vitamins and get enough fiber Slight change in taste
Pathophysiology: Lower GI Tract Irritable Bowel Syndrome (IBS) Abdominal pain with two of the following, to truly have IBS: Pain relieved with defecation Onset associated with change in frequency of stool Onset associated with change in form of stool Eliminate “red flag” symptoms Difficulty eliminating waste products
Pathophysiology: Lower GI Tract IBS Most common GI complaint difficulty eliminating - more common in women Etiology unknown Increased serotonin, inflammatory response, abnormal motility, pain Stress trauma, emotional paindepression
Pathophysiology: Lower GI Tract IBS - clinical manifestations Abdominal pain, alterations in bowel habits, gas, flatulence Increased sensitivity to certain foods Concurrent dg Lactose, wheat, high fiber foods, fibormyalgia, CFS, food allergies
Pathophysiology: Lower GI Tract IBS - Treatment Guided by symptoms Antidiarrheal agents Tricyclic antidepressants, SSRIs (selective seretonin reuptake inhibitors (another antidepressant) Bulking agents, laxatives Behavioral therapies- to relieve stress
Pathophysiology: Lower GI Tract IBS - Nutrition Therapy Can lead to nutrient deficiency, underweight, or malnourished Due to constant pain/ depression Decrease anxiety, normalize dietary patterns (for dietitian to do)
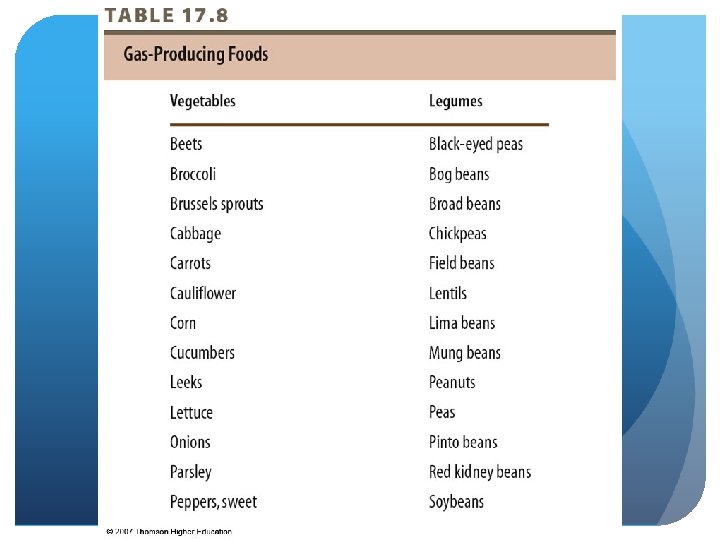
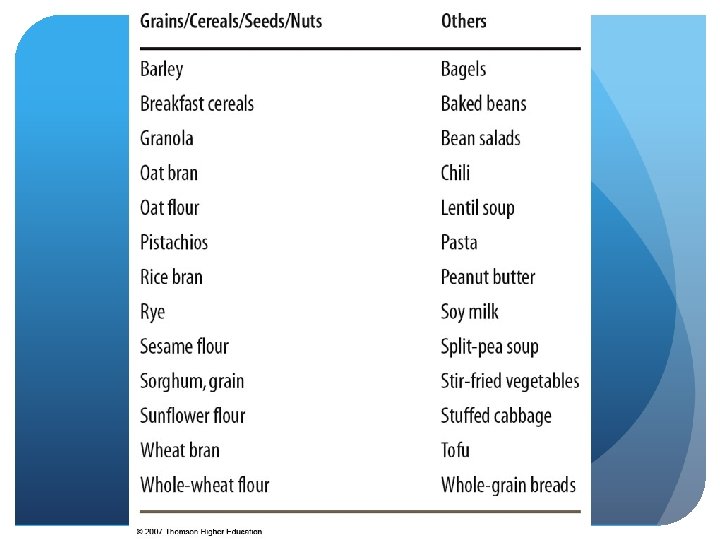
Pathophysiology: Lower GI Tract IBS - Nutrition Therapy Assess diet hx (trigger foods) Assess nutritional adequacy Focus on increasing fiber intake- to 25 grams per day after crisis state Adequate fluid- 2, 000 cc for a 2, 000 calorie diet Pre- and probiotics- rebuild gut flora Avoid foods that produce gas!! AND SWALLowed air- straws
© 2007 Thomson - Wadsworth
© 2007 Thomson - Wadsworth
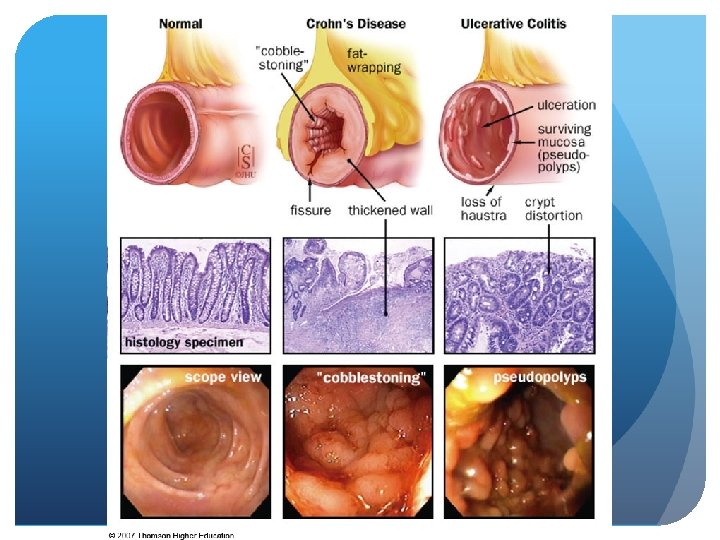
Pathophysiology: Lower GI Tract IBD - Nutrition Therapy] Antibiotics May require nut support, TPN Malnutrition High cal, pro, fiber regimen Fe, Zn, Mg, electrolytes concern (Na, K, Cl replacement) May need to increase kcal, protein, micronutrients
Pathophysiology: Lower GI Tract IBD - Nutrition Interventions During exacerbation- if gut works use it, Ensure, supplement to keep GI tract function Supplement Assess energy needs + stress factor- 200 -500 extra calories per day May need to increase protein 1. 5 - 1. 7 g/kg bw Low-residue, lactose-free diet Small, frequent meals- that are high calorie, high protein Glutamine and AGRININE decrease inflammation
Pathophysiology: Lower GI Tract IBD - Nutrition Interventions May use MCT oil (for problems with steatorrhea) Restrict gas-producing foods Increase fiber and lactose as tolerated (out of crisis stage, up to 40 grams per day) Advancement of oral diet- individual basis Multivitamin- make sure they have one, B 12, Fe, Zn, Ca, Mg, Cu- want to make sure these are included in the MV specifically
Pathophysiology: Lower GI Tract IBD - Nutrition Interventions During remission/rehabilitation Maximize energy & protein Weight gain and physical activity Food sources of antioxidants, Omega-3 s Pro- and prebiotics- help gut flora become stronger
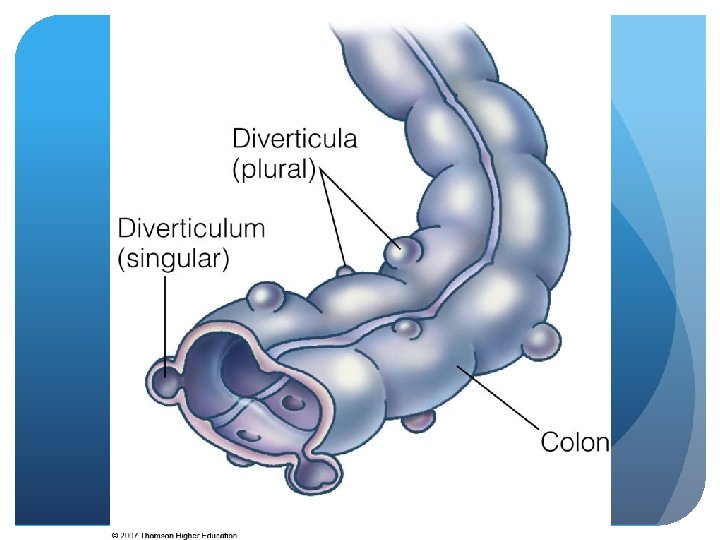
Pathophysiology: Lower GI Tract Diverticulosis/diverticulitis – abnormal presence of outpockets or pouches on surface of SI or colon/inflammation of these pockets In SI and/ or colon Low fiber intake- when they have it/ crisis state (minimize) History of constipation Increases inflammatory response Other risks Obese Steroids- for other disease states Alcohol/ caffeine Cigarette smoking Sedentary
Pathophysiology: Lower GI Tract Diverticulosis- do instruction then/diverticulitis pathophysiology Fecal matter trapped Development of pouches Diverticulitis- when matter is caught- bursts, GI bleeding, fever, abdominal pain, increased WBC count Food stuff- caught, infection Bleeding abscess, obstruction, fistula, perforation Worse case scenarios
Pathophysiology: Lower GI Tract Diverticulosis/-itis – Treatment/ Nutrition Therapy Specific focus on fiber- increase when not in crisis Pro- and prebiotic supplementation- help gut flora Acute- it is, NBO, bowel rest Antibiotics given to help inflammation Surgical resection
Pathophysiology: Lower GI Tract Diverticulosis/-itis – Nutrition Therapy -osis Avoid nuts, seeds, hulls- could get caught (may not be of a concern, new research? ) Fiber supplement (35 + 6 TO 10 grams) need some type of supplement -itis Bowel rest, clear liquids Avoid nuts, seeds, fibrous vegetables- want low fiber if they are able to eat at all