Lower Gastrointestinal Tract KNH 411 Lactose and low















 - Most common Pain relieved with")















- Slides: 39
Lower Gastrointestinal Tract KNH 411
Lactose and low residue
Stimulate acids Insulin release Between meals looking at motility © 2007 Thomson - Wadsworth
Large intestine looking at 24 to 48 hrs. holding for waste products
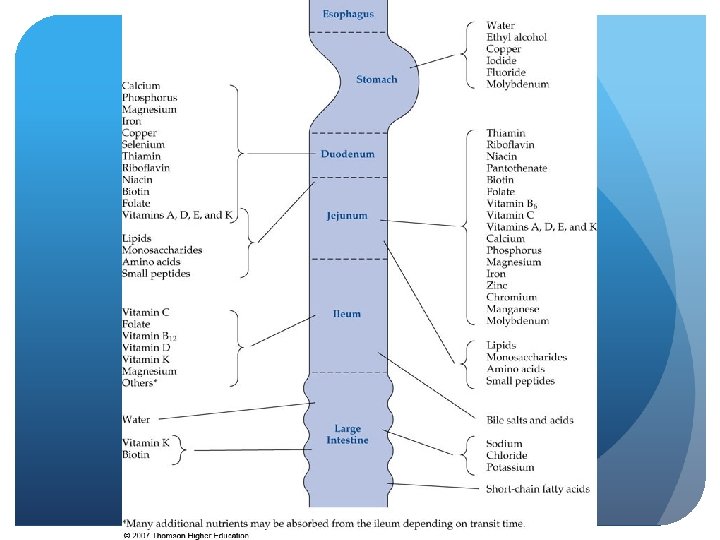
Pathophysiology: Lower GI Tract Malabsorption - maldigestion of fat, CHO, Protein # 1 concern- diarrhea and constipation Decreased villious height, enzyme production Decreased transit time With surgery can alter GI might need rest, decreased use in pancreas or liver
Pathophysiology: Lower GI Tract Malabsorption - fat Steatorrhea – fat travels undigested to large intestine and diarrhea Fat-soluble vitamins malabsorbed- ADE and K Potential for excess oxalate- kidney stones Abdominal pain, cramping, diarrhea Dg; fecal fat test or D-xylose absorption test, or small bowel x-ray
Pathophysiology: Lower GI Tract Malabsorption - Fat – Nutrition Restrict fat 25 -50 g/day Use of MCT supplements w/ infants Pancreatic enzymes- aid w/ malabsorption (chromes) Take before meals
Pathophysiology: Lower GI Tract Malabsorption - CHO Lactose malabsorption Increased gas, abdominal cramping, diarrhea Restrict milk and dairy products Products such as Lactaid can be rec. Celiac’s, Type 2 Diabetics & blood is swimming in sugar and water - concern with gastroperisis dumping syndrome - alcoholic malabsorption of CHO and PRO
Pathophysiology: Lower GI Tract Malabsorption - protein Protein-losing enteropathy- excessive protein loss albumin 21 day ½ life Reduced serum protein Peripheral edema cells cannot hold in water, fluid overload, low onconic pressure pre-albumin has 2 day ½ life which is useful for short term (ICU)
Pathophysiology: Lower GI Tract Malabsorption - Nutrition Therapy Results in weight loss Low vitamins and minerals, chronic PEM Treat underlying disease/ nutrient being malabsorbed
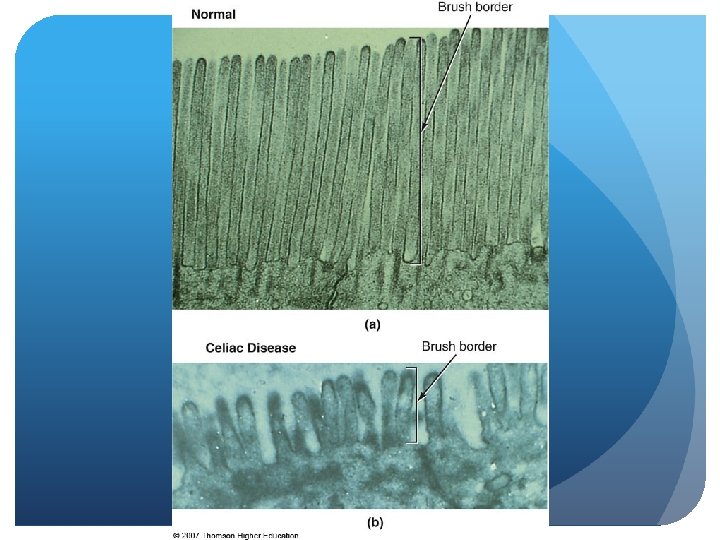
Pathophysiology: Lower GI Tract Celiac disease Damage to lower GI Genetic and autoimmune Occurs when alpha-gliadin from wheat, rye, malt, barley are eaten, can include oats Infiltration of WBC, production of Ig. A antibodies
Pathophysiology: Lower GI Tract Celiac disease - pathophysiology Damage to villi reduce height and flatten Decreased enzyme function Maldigestion and malabsorption Occurs with other autoimmune disorders type 1 diabetes, rheumatoid arthritis, dermatitis
Pathophysiology: Lower GI Tract Celiac disease - clinical manifestations Diarrhea, abdominal pain, cramping, bloating, gas -Bone and joint pain Muscle cramping, fatigue Skin rash and mouth ulcerations Higher risk for lymphoma and osteoporosis
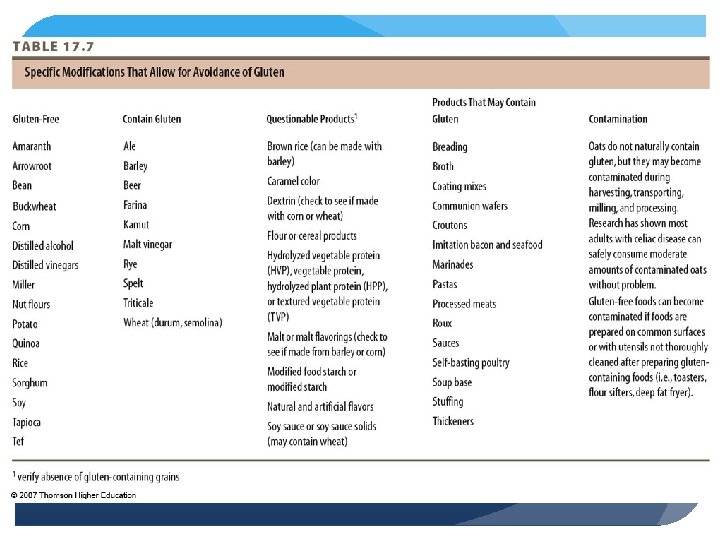
Pathophysiology: Lower GI Tract Celiac Disease - Diagnosis/Treatment/Prognosis Biopsy of small intestinal mucosa Reversal of symptoms following gluten-free diet Refractory CD; d/t coexisting disease
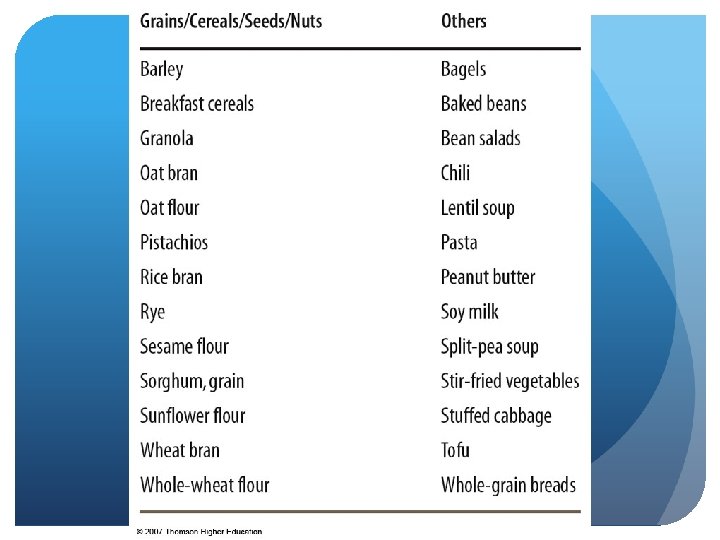
Pathophysiology: Lower GI Tract Celiac Disease - Nutrition Intervention Low-residue, low-fat, lactose-free, gluten-free diet No more than 45 to 55 g/day Identify hidden sources of gluten Specialty products max. allowance of oats ½ cup per day
Pathophysiology: Lower GI Tract Irritable Bowel Syndrome (IBS) - Most common Pain relieved with defecation Onset associated with change in frequency of stool Onset associated with change in form of stool Eliminate “red flag” symptoms
Pathophysiology: Lower GI Tract IBS Most common GI complaint -pain w/ defecation, women most common Etiology unknown Increased serotonin, inflammatory response, abnormal motility, pain Any emotional trauma can trigger
Pathophysiology: Lower GI Tract IBS - clinical manifestations Abdominal pain, alterations in bowel habits, gas, flatulence Increased sensitivity to certain foods lactose, wheat, high fiber Concurrent dg - fibermyalgia chronic fatigue syndrome, food allergies
Pathophysiology: Lower GI Tract IBS - Treatment Guided by symptoms Antidiarrheal agents Tricyclic antidepressants, SSRIs Bulking agents, laxatives Behavioral therapies - Relieve stress
Pathophysiology: Lower GI Tract IBS - Nutrition Therapy Can lead to nutrient deficiency, underweight - Due to constant pain and depression Decrease anxiety, issues with trying to normalize dietary patterns
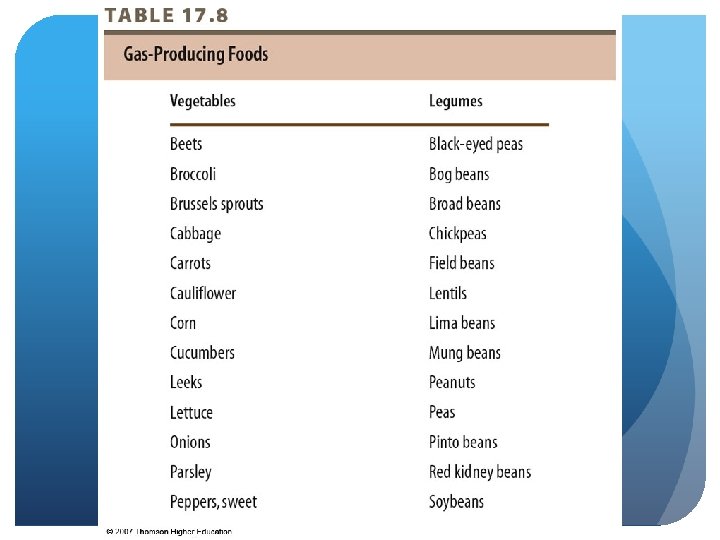
Pathophysiology: Lower GI Tract IBS - Nutrition Therapy Assess diet hx- what’s triggering? Assess nutritional adequacy- 24 hour recall Focus on increasing fiber intake- 25 g/day Adequate fluid- help with GI motility Pre- and probiotics- rebuild flora Avoid foods that produce gas – swallowed air- no straws
© 2007 Thomson - Wadsworth
© 2007 Thomson - Wadsworth
Pathophysiology: Lower GI Tract IBD - Nutrition Therapy Malnutrition May need to increase kcal, protein, micronutrients low Key: iron, zinc, magnesium, electrolytes (K, Na, Cl)
Pathophysiology: Lower GI Tract IBD - Nutrition Interventions- parental in worst case scenario During exacerbation- inflammed- enteral products (ensure) Supplement –glutamine and arginine Assess energy needs + stress factor- 200 to 500 cal extra May need to increase protein- 1. 5 to 1. 7 g/kg body weight Low-residue, lactose-free diet Small, frequent meals
Pathophysiology: Lower GI Tract IBD - Nutrition Interventions May use MCT oil Restrict gas-producing foods Increase fiber and lactose as tolerated Advancement of oral diet Multivitamin – B 12, iron, zinc, calcium, magnesium and copper
Pathophysiology: Lower GI Tract IBD - Nutrition Interventions During remission/rehabilitation Maximize energy & protein Weight gain and physical activity Food sources of antioxidants, Omega-3 s Pro- and prebiotics
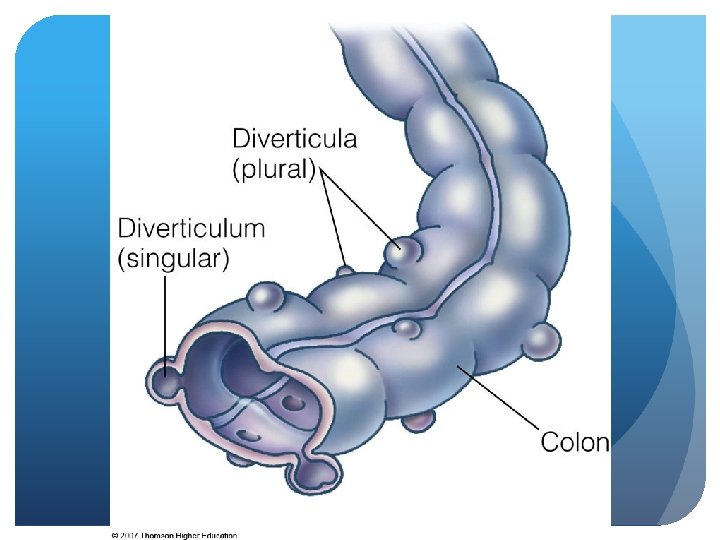
Pathophysiology: Lower GI Tract Diverticulosis/diverticulitis – abnormal presence of outpockets or pouches on surface of SI or colon/inflammation of these Low fiber intake Increases inflammatory response Other risks - strong history of cigarettes, obesity, sedentary lifestyle, caffeine
Pathophysiology: Lower GI Tract Diverticulosis/diverticulitis – pathophysiology Fecal matter trapped Development of pouches Diverticulitis Food stuff Bleeding abscess, obstruction, fistula, perforation
Pathophysiology: Lower GI Tract Diverticulosis/-itis – Treatment/ Nutrition Therapy Specific focus on fiber Pro- and prebiotic supplementation Acute Antibiotics - Nothing by mouth, clear liquids, food liquids, reg. diet
Pathophysiology: Lower GI Tract Diverticulosis/-itis – Nutrition Therapy -osis Avoid nuts, seeds, hulls Fiber supplement- add 6 to 10 g total to current rec. for fiber -itis Bowel rest Avoid nuts, seeds, fibrous vegetables - May not be as concerned