Hepatic nodules Tumors Lecture 10 Focal Nodular Hyperplasia







 Unifocal massive tumor. (2) Multifocal tumor nodules of variable size. (3)")




: Two main types of gallstones: 1 - Cholesterol stones: q Composed of")


 # Small in")








- Slides: 32
Hepatic nodules & Tumors Lecture 10
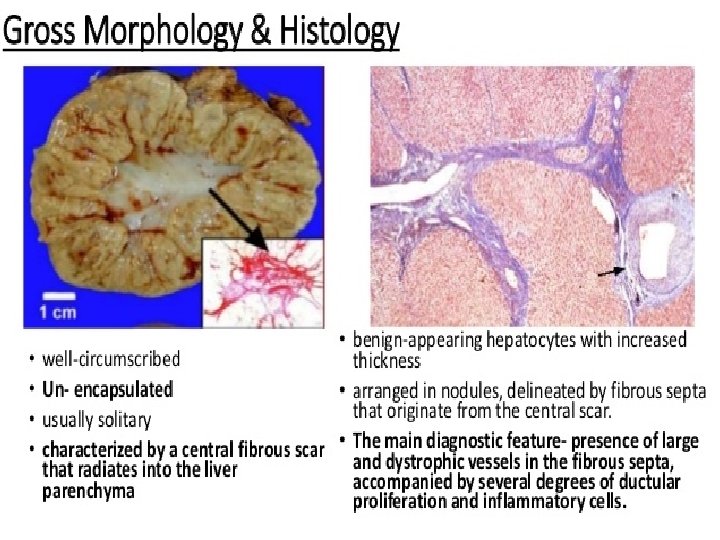
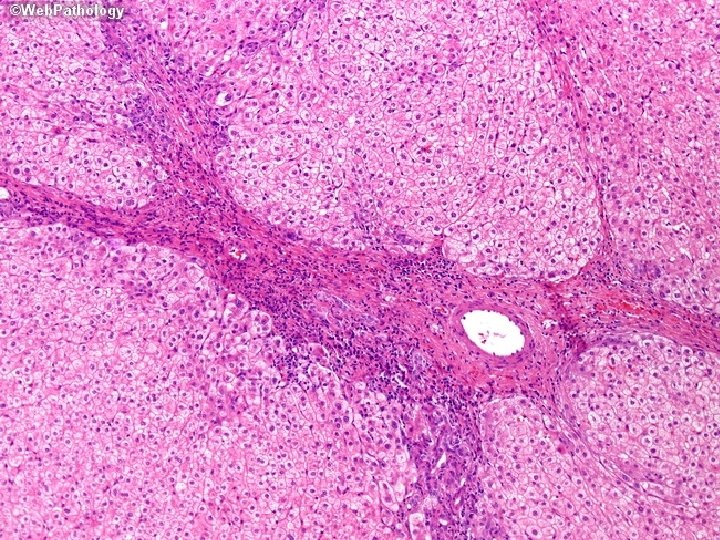
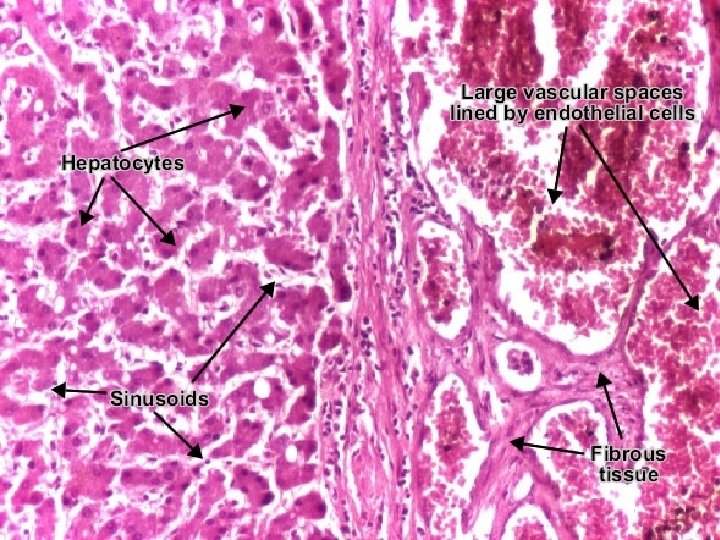
Focal Nodular Hyperplasia: v. Localized, well-demarcated, poorly encapsulated. v. Not a true neoplasm. v. No risk for malignancy. v. Nodules consist of: v. Hyperplasic hepatocyte with central stellate shap fibrous scar. (Star shape) Cause: (Suggestion) v. A response to abnormal blood flow Alternating areas of parenchymal regeneration & atrophy. v. Most common in women in reproductive age, growing in response to estrogens. (Female sex H. ) (Including those found in contraceptive pills).
Benign Tumors Most common: Cavernous hemangiomas: Well circumscribed lesions consist of blood vessels & intervening stroma. Gross: Red-blue, soft nodules. Less than 2 cm in diameter.
Hepatic Adenoma: Benign neoplasm. v. Occurs in women in child-bearing age who have used oral contraceptive pills. v. Regress by discontinuity of hormone use. v. Well demarcated lesion. v. Not encapsulated tumors. v. Pale, yellow-tan, or bile-stained.
Histologic examination: v. Sheets & cords of cells. v. Resemble normal hepatocytes. v. Or have minimal variation in cell & nuclear size. v. Portal tracts are absent. (Loss of normal architecture). v. Prominent arterial vessels & draining veins.
Hepatic malignancies: 1 - Primary hepatic malignancies: Most common is hepatocellular carcinomas. 2 - Metastatic cancers: q Liver is most commonly involved by metastatic cancers. q Most common metastatic hepatic neoplasm are carcinomas from colon, lung, & breast.
Hepatocellular Carcinomas: Hepatoma: Three major etiologic associations: v 1 - Infection with HBV or HCV. Chronic HCV infection is the most important risk factor in development of liver cancer. . v 2 - Alcoholic cirrhosis: 90% of cases develop cancer v 3 - Aflatoxin exposure: v. Carcinogenic toxins found in moldy grains & peanuts that results in mutations.
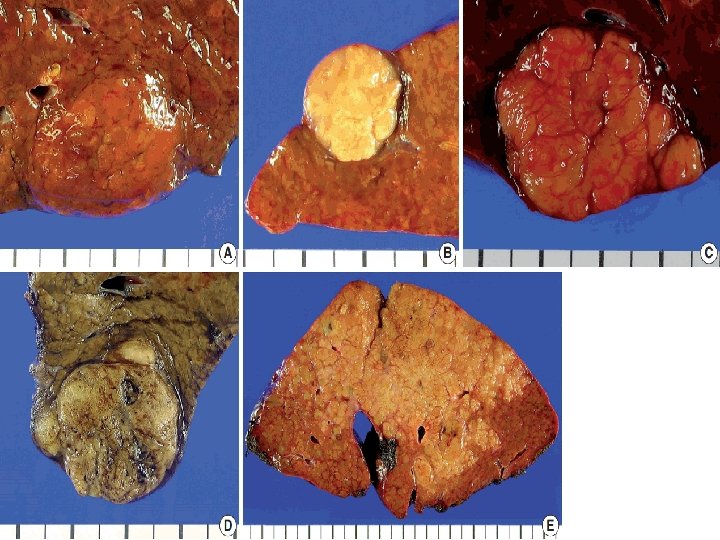
Morphology: Gross: (1) Unifocal massive tumor. (2) Multifocal tumor nodules of variable size. (3) Diffusely infiltrative cancer involving the entire liver, blending into the cirrhotic background. Tumor masses: v. Yellow white. v. Or bile staining & hemorrhage or necrosis. v. Soft in consistency because of little C. T. stroma in most hepatocellular carcinomas.
Histologic examination: 1 - Well differentiated lesions: Hepatocytes arranged in cords, trabeculae or glandular patterns with globules of bile found within the cytoplasm of cells.
Well-differentiated hepatocellular carcinoma: Distortions of normal structures: Liver cell plates are markedly widened & frequent pseudoacinar structures (arrows)—abnormal bile canaliculi contain bile.
2 - Poorly differentiated lesions: Composed of large, multinucleate anaplastic giant cells.
Disorders of gallbladder & extrahepatic biliary tract Gallbladder diseases: 1. 95% of these diseases: Cholelithiasis =Gallstones. 2 - Cholecystitis: Inflammation. 3 - Tumors of biliary tract: Cholangiocarcinoma.
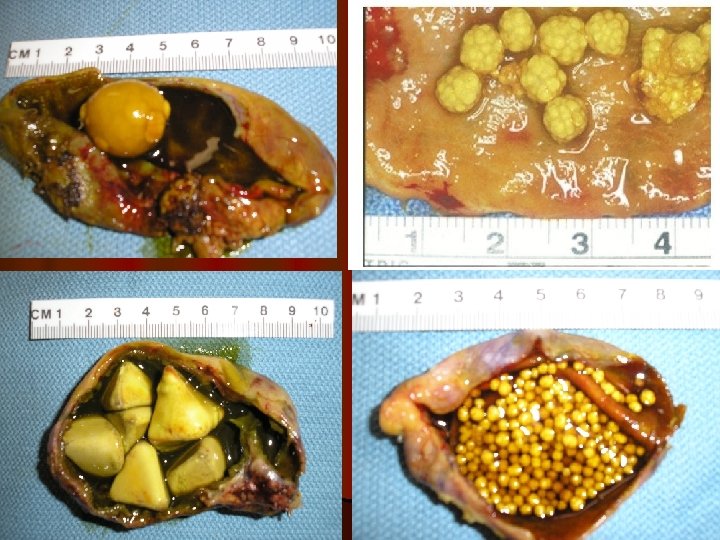
Cholelithiasis (Gallstones): Two main types of gallstones: 1 - Cholesterol stones: q Composed of cholesterol. q Formed when there is cholesterol supersaturation (Increase concentrations) 2 - Pigment stones: q Made of bilirubin calcium salts. q Form due to the presence of unconjugated bilirubin in biliary tree. (In hemolytic anemia).
1. Cholesterol stones: Morphology: v. Arise exclusively in gallbladder. v. Consist of 50 -100% cholesterol Pale yellow. v. Increasing proportions of calcium carbonate, phosphates & bilirubin Gray-white to black. v. Ovoid & firm. v. Occur singly, but most often are numerous. v. Most cholesterol stones are radiolucent in X-ray. v 20% have sufficient calcium carbonate to appear radiopaque. v. Gallbladder mucosa: Redness due to acute & chronic cholecystitis.
2. Pigment stones: v. Arise anywhere in the biliary tree. v. Contain calcium salts of unconjugated bilirubin & lesser amounts of other calcium salts, mucin, glycoproteins, & cholesterol. Classified into: 1. Black stones. 2. Brown stones.
1 - Black stones: # Found in sterile gallbladder. (Not infected) # Small in size, fragile to touch & numerous. # 50 -75% appears as radiopaque. (Because of calcium carbonates & phosphates).
2 - Brown stones: # Found in infected intra- or extra-hepatic ducts. # Soft, greasy, soap like consistency (radiolucent). # Results from retained fatty acid salts.
Clinical Features: ØAsymptomatic throughout life in 70 -80%. ØSymptoms are striking in unfortunate minority. Sever biliary pain, localizes at the right upper quadrant or epigastric region, constant or, less commonly, spasmodic. Pain is caused by: 1. Obstruction of gallbladder or biliary tree. 2. Or by inflammation of gallbladder itself. More severe complications: Empyema, perforation, fistulas, infl. of biliary tree & obstructive cholestasis or pancreatitis.
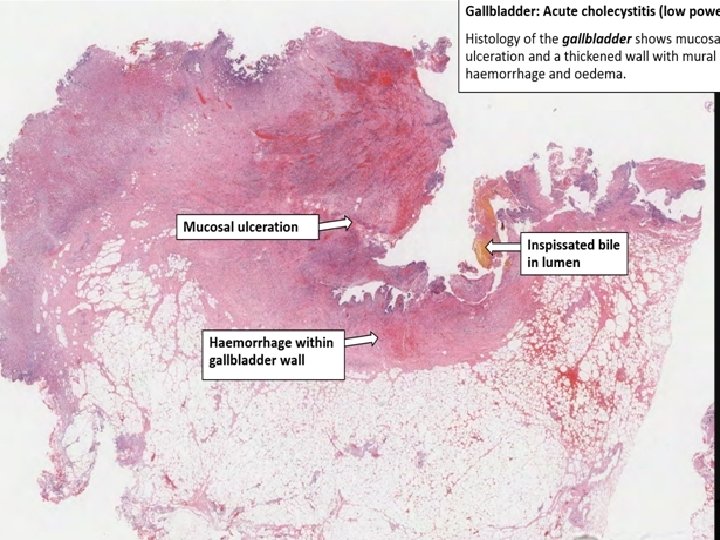
Cholecystitis v. Inflammation of gallbladder. v. Always occurs in association with gallstones. v. Acute, chronic, or acute superimposed on chronic. Morphology: Acute cholecystitis: v. Gallbladder: v. Enlarged, . v. Tense. v. Bright red or motteled violaceous color due to subserosal Hg.
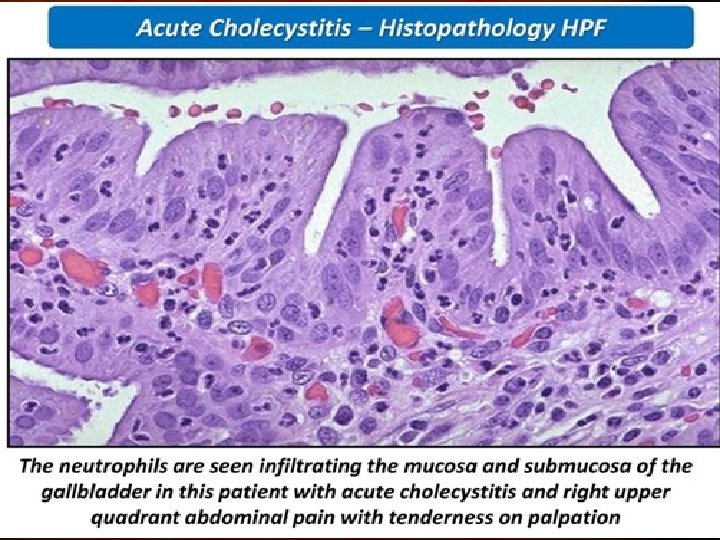
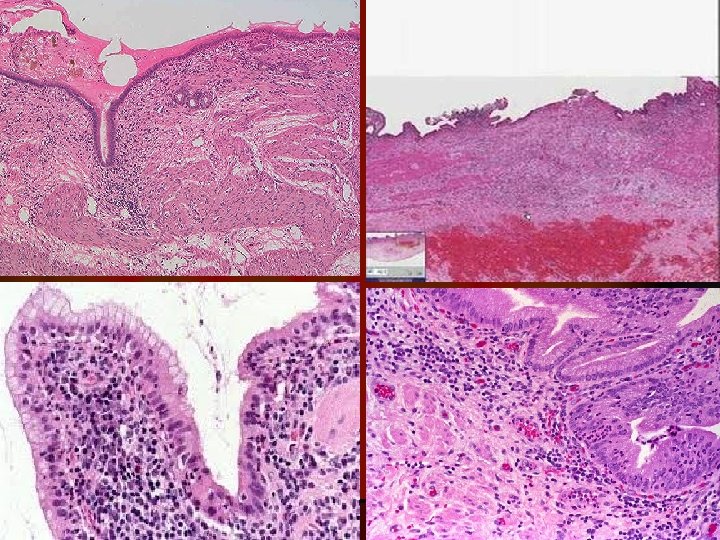
Serosa: Covered by fibrinous or fibrinopurulent exudate. Lumen: Filled with cloudy or turbid bile contain fibrin, blood & pus (Empyema) Wall: Thickened, edematous & hyperemic. In more severe cases: Gallbladder is transformed into green-black necrotic organ: Gangrenous cholecystitis. v. Histologic examination: v. Inflammatory reactions: Acute inflammation: v. Edema, leukocytic infiltration, congestion, frank abscess formation, or gangrenous necrosis.
Morphology of chronic cholecystitis: v. Presence of stones within gallbladder. v. Gallbladder: v. Contracted, normal size or enlarged. v. Submucosa & subserosa: Thickened by fibrosis. Clinical Features: Acute cholecystitis: q. Sever biliary pain: q. Steady, upper abdominal in location. q. Radiates to right shoulder. q. Fever & nausea. q. Leukocytosis & intolerance for fatty foods.
Tumors: Carcinoma of Gallbladder: v. Most common malignant tumor of biliary tract. v. Cause: Gallstones: v. Present in 60 -90% of cases Recurrent trauma & chronic inflammation Cancer. v 1. Adenocarcinoma: Most common type. v 2. Squamous cell carcinomas: 5%. Morphology: 1 -Exophytic mass: Grows into lumen as cauliflower like mass & also invades the underlying wall. 2 -Infiltrating growth causing diffuse thickening & induration of gallbladder wall. (Loss of elasticity due to fibrosis)
Adenocarcinoma of gallbladder. Opened gallbladder contains a large, exophytic tumor fills the lumen & Glandular structures histologically.
Thank you