Hemostatic Disorders Hemostasis vessels platelets clotting factors Platelet





 Partial thromboplastin Time ( PTT) Prothrombin Time ( PT")





 - Type 3")

 * weight(kg) * 0. 5")
: X-linked, 1 in 25000 males Dose for F 9=")
- Slides: 16
Hemostatic Disorders
Hemostasis: - vessels - platelets - clotting factors
Platelet Phase Vascular injury -> change of v. WF -> binds to platelets -> activation of plts -> aggregation of plts -> platelet plug
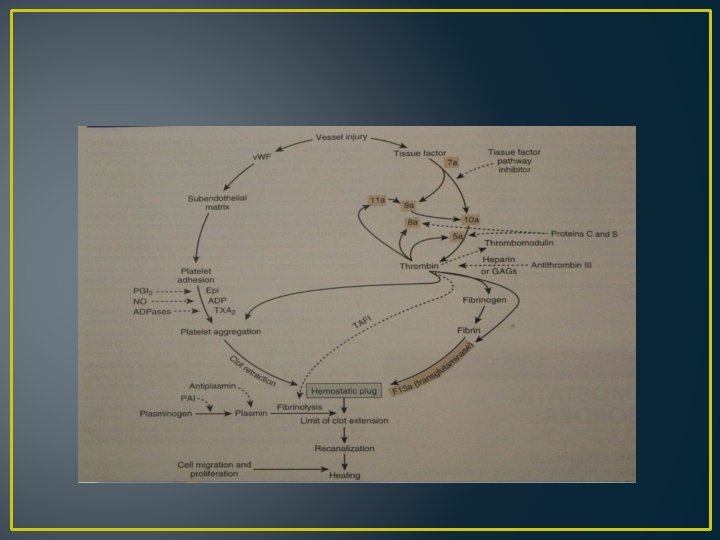
Coagulation Phase
Approach to hemostatic Disorders Clinical manifestation: Petechia/ purpura Ecchymoses Hematomas Easy bruising Bleeding ( GI, hematuria, epistaxy, …)
Laboratory testing CBC ( platelets) Partial thromboplastin Time ( PTT) Prothrombin Time ( PT ) Bleeding Time ( BT ) Fibrinogen
Disorders of platelets Thrombocytopenia: 1 -decreased plts production: Amegakaryocytic thrombocytopenia, TAR syn. , wiskott Aldrich, 2 - Increased destruction: ITP 3 - sequestration
Disorders of Plt function: - Bernard Soulier syn. - Glanzmann thrombasthenia
ITP -immune mediated mechanisms -Child appears well -most common cause of thrombocytopenia -rarely ITP is due to an autoimmune disease such as SLE
Clinical manifestations -young children -typically 1 – 4 weeks after acute viral infection -abrupt onset of petechiae, purpura & epistaxis -thrombocytopenia usually severe -adenopathy & hepatosplenomegaly is unusual
-RBC & WBC counts are normal -bone marrow examination : increased megakaryocytes & normal erythroid and myeloid elements.
Von willebrand Disease - Type 1 - Type 2 ( dysproteinemia) - Type 3 Treatment : - DDAVP - v. WF containing concentrates
Hemophilia A: deficiency of F 8 X- linked, 1 in 5000 males, - Mild : > 5% - Moderate : 1 -5% - Severe : < 1% Prolonged PTT
Dose for Factor 8 = desired level(%) * weight(kg) * 0. 5
Hemophilia B( factor 9 deficiency): X-linked, 1 in 25000 males Dose for F 9= desired level(%) * weight (kg) * 1. 5