FXR agonist in NASH 2019 04 04 Pf

 is a increasingly common cause of")



 Ligand Introduction • Besides digestive role, bile acids(BA) act as")




")

 and cirrhosis 2")




















 and cirrhosis 2")



- Slides: 41
FXR agonist in NASH 2019년 04월 04일 목요세미나 Pf 김 원 / R 4 이철형
Prevalence of NAFLD/NASH Introduction • Non-alcoholic steatohepatitis (NASH) is a increasingly common cause of chronic liver disease with increased mortality, proceeds to cirrhosis, HCC • 3 rd m/c cause of liver TPL • Overall global prevalence of NAFLD diagnosed by imaging: 25 - 30% (highest in middle east, lowest in Africa) Chalasani, N. , et al. (2018), Hepatology 67(1): 328 -357.
NAFL/NASH Introduction Chalasani N. Practice Guidance from the AASLD; Hepatology 2018; 67: 328 -357 Sleigenger and Fordtran's Gastrointestinal and Liver Disease, 10 th ed. , Chapt 87
Natural History of NAFLD Introduction “two-hit hypothesis" Diehl AM. NEJM 2017; 377: 2063 -72. Chalasani N. Practice Guidance from the AASLD; Hepatology 2018; 67: 328 -357
Treatment strategy of NAFL/NASH Introduction • Whom to treat? • Pharmacologic treatment should be limited to "biopsyproven” NASH and fibrosis >10% of Bwt PIVENS trial Chalasani N. Practice Guidance from the AASLD; Hepatology 2018; 67: 328 -357 Wong, V. W. , et al. , Nat Rev Gastroenterol Hepatol 2018; 15(8): 461 -478.
Farnesoid X Nuclear Receptor(FXR) Ligand Introduction • Besides digestive role, bile acids(BA) act as metabolically active signal molecule • Via enterohepatic circulation, BA activates nuclear Rc(FXR) which plays a key role in control of hepatic lipogenesis, plasma TG turnover, also involves insulin sensitivity • 6 -ethylchenodeoxycholic acid (obethicholic acid, OCA), a synthetic variant of natural bile acid, has shown improvement of hepatic steatosis, fibrosis in preclinical data • Less lipophilic bile acid UDCA did not show efficacy in clinical trials Trauner, M. , et al. , Dig Dis 2010, 28(1): 220 -224. Mudaliar, S. , et al. , Gastroenterology 2013, 145(3): 574 -582. e 571.
FLINT Trial F Method • Multicenter, double-blind, placebocontrolled, parallel group, randomized clinical trial at medical centers in the USA (coordinated at Johns Hopkins Univ) (phase IIb) • Non-cirrhotic NASH, with evidence of biopsy • MAR 2011 – Dec 2012
FLINT Trial Method Week: 2 4 12 24 36 Oral OCA 25 mg qd ( n=141 ) 48 60 72 96 End of Tx biopsy Placebo ( n=142 ) Interim analysis 24 wk post Tx Blood samples (lipids, glucose, insulin) at each visit Bwt, height, waist and hip circumference at initial and interim times All patients received standardized recommendation on healthy eating habits, Wt reduction, exercise, management of metabolic syn.
FLINT Trial Method •
Interim Analysis Method • Surrogate outcome: changes of ALT between week 24 • - 24% (95% C. I -45% to -3%) • pre-specified interim criteria -20% in the lower 95% CI was met • Interim analysis of primary outcome when 50% end of Tx Bx done • Lan-De. Mets method with O'Brien-Fleming Boundaries • Criteria of superiority of OCA (p=0. 0031) were met (p=0. 0024) • Decided not to biopsy the final 64 patients • Also serum cholesterol concentration increased more in the OCA group, more aggressive lipid management was adopted • More than 130 mg/d. L for non diabetics, 100 mg/d. L for diabetics
Statistical Analysis Method • Intention-to-treat analysis for primary outcome excluded 64 patients (without Bx) • All patients included secondary non-histological outcomes • Stratified by clinical center and diabetes status • Primary and binary secondary outcomes • Mantel-Haenszel test • Continuous secondary outcomes from baseline to 72 weeks • ANCOVA models
Trial Profile Result
Baseline Characteristics Result Of 282 patients, Stage 3 fibrosis 63 (22%) and cirrhosis 2 patients
Histologic outcome Result
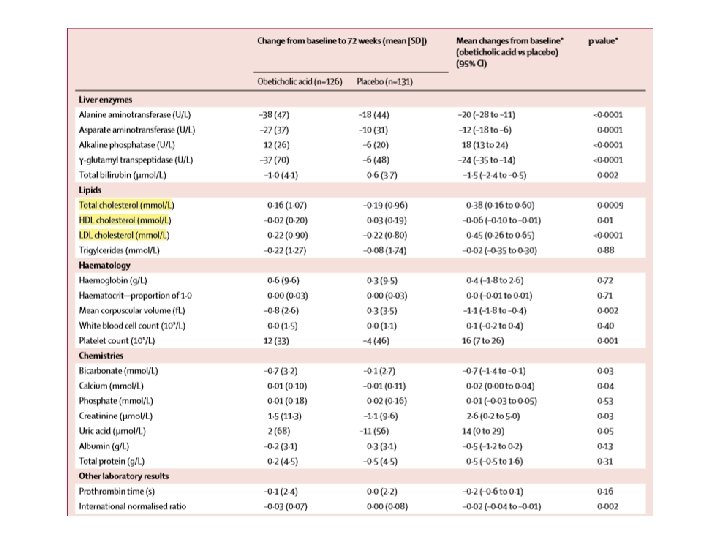
Secondary outcomes Result
Secondary outcomes Result
Secondary outcomes Result
Safety Result 30 patients in OCA group, comparable to placebo group, experienced severe adverse events. 2 mortality occurred in OCA group.
Secondary Analysis of FLINT Trial Method 50/102 in OCA group and 23/98 placebo group showed response
Secondary Analysis of FLINT Trial Method • Objectives: Identify clinical predictors of histologic response • 200 patients (OCA 25 mg n=102; placebo n=98) included in the analysis • Multivariable logistic regression model with stepwise selection • Akaike information criterion (AIC) and Bayesian information criterion (BIC) • Apply penalty on the number of selected predictors
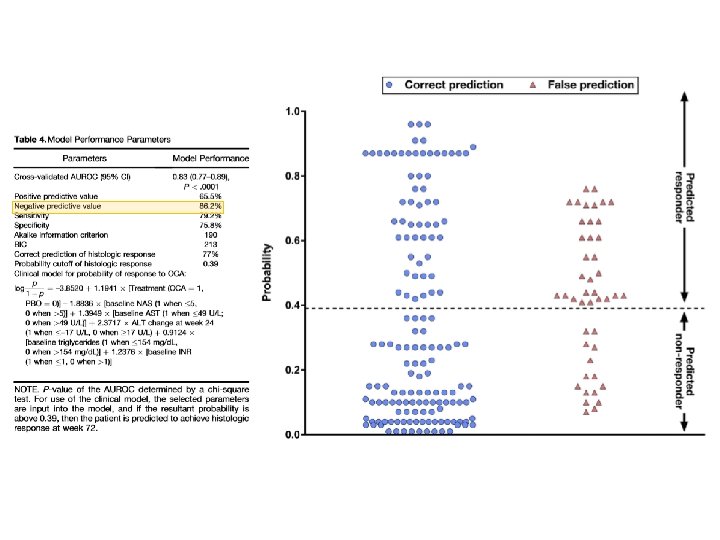
Selected Predictors Method • Parameters were used build a model for predicting histologic response • AUROC, sensitivity/specificity, PPV/ NPV, % of correctly classified cases
Method • Stepwise selection model • Significance level 0. 1 => allow a variable into model • Significance level 0. 15 => variable to stay in a model when another variable introduced
Baseline characteristics was balanced Result
Univariate analysis Result
Univariate analysis Result
Variables selected by stepwise selection Result
Multivariable analysis Result At cutpoint 0. 39, sensitivity = 77%
Discussion • OCA improved biochemical and histological features of NASH. Fibrosis as well as necroinflammatory change improved. • Obtain liver biopsy specimen before and after the treatment and assessed by expert liver pathologists • Due to multicenter nature, lack of detailed tracking of intervention including dose of statin during trial.
Discussion • Although OCA had an effect on the primary endpoint, did not cause a significant portion to reach resolution of NASH. • NAS score does not fully reflect the status of NASH. Long-term outcome studies are needed to determine the histological measures with greatest clinical significance. • Overall histological improvement rates were similar with PIVENS study • OCA 50/110 (45%), Vitamin E 36/84 (43%), Pioglitazone 27/80 (34%)
Dyslipidemia in OCA group Discussion • FXR activation decreases hepatic lipogenesis by down-regulating SREBP 1 c and increasing SIRT 1 • However, it reduces bile acid synthesis by inhibiting the conversion of cholesterol to bile acids • FXR agonists promote reverse cholesterol transport out of tissue via HDL • Treatment with statin might contributed to the changes toward baseline, should prospectively monitor lipid profile. • Besides 3 patients with severe pruritis, OCA was well tolerable to most of patients
Hepatic insulin resistance Discussion • Previous phase IIa study with OCA showed increased insulin sensitivity via hyperinsulinemic euglycemic clamp technique - Sunder M. et al. Gastroenterology 2013; 145: 574 -5 • Effect of OCA on insulin resistance might be transient and would be reversed by adaptive mechanisms to longterm treatment. • However, along with elevated serum cholesterol pool, insulin resistance could signal an increased risk of atherogenesis.
Factors associated with histologic response in NASH pts Discussion • High NAS score, low baseline TG, INR<1, low baseline AST, early decrease in ALT level are significant predictors • High NAS – quantitatively measurable change more likely • Fasting TG level • Reflection of hepatic secretion and peripheral lipolysis • Lower level of TG reflects higher capacity of liver function improvement • AST, ALT levels are metrics of liver injury • Patients with higher disease activity but still with conserved liver function are likely having potential to improve
Critical Appraisal Discussion • Obethicholic acid regulates lipid metabolism via FXR pathway and coupled with TGR 5, also mediates anti-inflammatory and antifibrotic properties. • OCA groups shows higher insulin resistance at baseline. Along with administration of vitamin E, pioglitazone, statin Tx, this could exaggerates potency of OCA. • Two mortalities (CHF, cardiac infarction) occurred in OCA group and 30/141 patients experienced severe adverse events. Close monitoring with side effect profile would be required in further study, especially cardiac events. • The model predicted low baseline AST to be predictive value for histologic response. There remains further study regarding patients with high necroinflammatory activity.
Baseline Characteristics Result Of 282 patients, Stage 3 fibrosis 63 (22%) and cirrhosis 2 patients
Safety Result 30 patients in OCA group, comparable to placebo group, experienced severe adverse events. 2 mortality occurred in OCA group.
Critical Appraisal Discussion • From biochemical evidence, the pharmacologic effect seems transient. Large clinical trials with prolonged therapy should be considered. • As NAFLD has multifaceted nature in pathophysiology, combination of future drug would be needed.