Elena Loomis MSN APRN AGNPC CDP CCRN Discussion




















































. Epidemiology and")
- Slides: 62
Elena Loomis, MSN, APRN, A-GNP-C, CDP, CCRN
• Discussion of the importance of identification and assessment of depression, delirium, and dementia • Frailty Syndrome • Discuss Late Life Depression • Discuss Delirium • Discuss Dementia • BPSD • Use of validated tools and assessments to differentiate between the 3 D’s in order to initiate appropriate treatment
� Clinically recognizable state of increased vulnerability resulting from aging-associated decline in reserve and function across multiple physiologic systems such that the ability to cope with everyday or acute stressors is comprised. � Phenotypic Criteria �Must Meet 3/5 Low grip strength Low energy Slowed waking speed Low physical activity Unintentional weight loss
Hopkins Frailty Assessment CSHA Clinical Frailty Scale
Cognitive function is the process to perceive, registering, store information and use information � Physiological �Loss of recent memory �Response time is delayed �Diminished ability to learn complex information � Pathologic �Depression �Delirium �Dementia
MUST ASSESS COGNITIVE FUNCTION & DETERMINE BASELINE ABILITY TO FUNCTION ADLs & IADLs
Late Life Depression
� 1. 2 -1. 8 million >65 years with depressive disorders � Elderly are fastest growing suicide group � 40 -50% with AD develop depression � 50% of LTC � MDD Prevalence � 1 -3% Community � 10% Primary Care � 15% Medical Inpatients � 15% Long-Term Care
� DSM-5 � Most of day over 2 week period criteria includes at least 5 with 2 including � Depressed mode most of day for over 2 weeks � Anhedonia � Weight Loss/Gain � Sleep disturbance � Psychomotor changes � Diminished ability to think/concentration � Recurrent thoughts of death SIG-E-CAPS � Sleep disturbance � Interests � Guilt low self-esteem � Energy � Appetite � Psychomotor � Suicide
� Concurrent medical diagnosis � 80% of elderly have 1 chronic illness � 50% have at least 2 chronic illnesses Most Common Comorbidities HTN 58% Chronic Pain/Arthritis 56% Cancer 57% CAD 48% Pulmonary Disease 42% Parkinson/Disease 1 -2%
� Stroke � 25 -50% � CV post CVA events � 65% following AMI � 50% s/p CABG � Orthopedic Surgeries � 20% s/p THR � 28% s/p TKA
Late life depression � Major depressive episode occurring for first time in an older person � Usually >50 or 60 years of age � Consider degree of impairment � Concurrent medical problems � Lower functional expectations
� Similar to Adult s/s but could include � More Somatic or physical c/c GI most frequent � More likely to accept “unhappiness” “I’m old. . what do you except” � Irritability � Increasing fatigue or loss of energy Symptoms � Affective �State of mind � Cognitive �Slow and Low � Somatic �Either side of normal
“Do you often feel sad or depressed? ”
92% Sensitivity 81% Specificity 93% Sensitivity 97% Specificity
“I think I’m blue” “I’m fine, just a little to much thinking” 1. 2. 3. 4. Hx of Dysthymia Is this the First Episode Abulia Demoralization
Talk Therapy/Group RX � � SSRI � � Escitalopram Start 5 mg PO daily Max 10 mg PO daily � Mild-Mod Renal no adjustments Citalopram Start 10 mg PO daily Max 20 mg PO daily � Mild-Mod Renal no adjustments � p. QTi Hyponatremia SNRI � If Chronic pain priority Venlafaxine � Start 37. 5 mg � Max 225 mg severe 375 mg � � Cr. CL 10 -70 25 -50% Cr. CL <10 by 50% Other � If sleep and appetite are priority Miratazpine � Start 7. 5 mg at HS � Max 150 mg at HS � � � Renal not defined Do not use concurrent with benzos If SSRI are contraindicated or can use in addition Buproprion SR � Start 75 mg PO daily � Max 150 mg in divided doses � � Seizure Renal How long? The treatment that gets someone well is the treatment that will keep that person well.
� Late Life Depression � Rx �Patient specific �Use recommended �Mo. CA �Prodromal � Medication to AD Review � H&P � Sensory Evaluation � Pain Evaluation � Risk vs Benefit � Metanaylsis �Many studies=good efficacy of 55 & older (P=0. 0001) �When mean age >65 years decreased efficacy (P=0. 265)
� Portion of Executive Function � Lack of ambition or drive � Lack in ability to be a self starter � Research has found that no amount of antidepressant medications makes a meaningful amount of improvement �most time using max dose with increase s/e � Some research in buproprion � Keep busy �Hobbies �Adult Daycares �Volunteer positions
� Psychological distress that involves hopelessness, helplessness, loss of purpose and meaning, and existential distress � Progressive � Cancer Disease � Approximately 71% with demoralization did not meet criteria for depression � Cancer � High Spirituality � Anxiety � Loneliness � Must thoroughly � Talk Therapy � CBT assess for depression
� Increased Morbidity � Increase Mortality � Slow recovery from surgery/illness/falls � Malnutrition � Social isolation � Increase substance abuse � Suicide
� >65 years make up 12% of population � But � are 18% of all suicides 15 : 100, 000 >65 years attempted suicide � 75. 4 million baby boomers � 11, 000 lives lost from suicide � 20% provider the day they die 40% the week they die 70% in the month they die � Depression is TREATABLE � � � 80% clinical dx can be effectively treated
� Syndrome of sudden deterioration of mental function � Triggered by illness �Body �Brain �Acute injury �Drug intoxication
Mortality rates 22 -76% as high as MI or sepsis!!! Up to 75% will die within 3 years of delirium Misdiagnosed 66%
Old School Thinking New Research Ach Deficiency Abnormal Immune Physiologic Stress Acute s/s Treatment Resolve Resume Life Unhealthy Brain in Unhealthy Body Acute BUT Can be prolonged And segway into dementia
� Male � Advanced � Whose age >60 � Cognitive Impairment � Depression � Vision & Hearing impairments at risk? �Community 8 -17% dwellers �LTC 60% residents >75 yrs �Hospitalization 50% will develop � 15 -53% post op � 70 -80% ICU
Predisposing Precipitating Perpetuating MCI Sepsis Increase sedation Dementia Surgery Restraints Comorbidities Drugs Age Hospitalization Frailty Foley IV
�Dehydration �Malnutrition �Immobility �Infection �Constipation �Psychoactive medications �Disorienting environment �Acute metabolic disturbance �Trauma �Hypoxia �ETOH/drug w/d
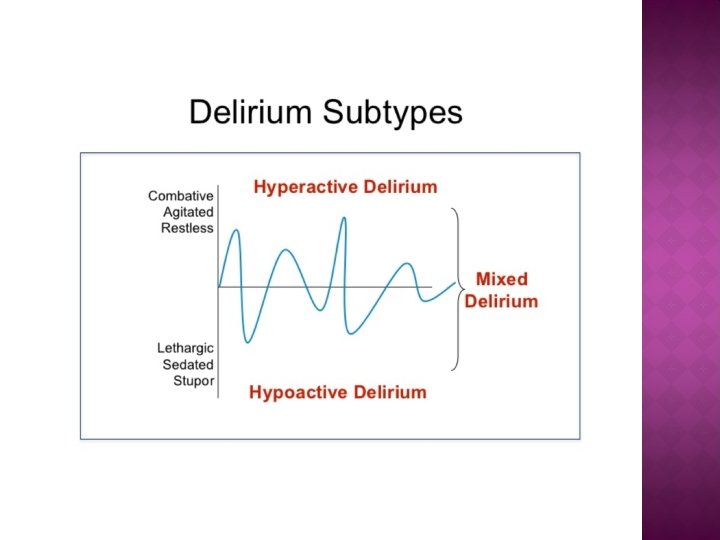
� Acute onset �Within hours or days � Fluctuating course � Poor attention � Disorganized thinking � Alerted LOC
Hyperactive Mixed Hypoactive Most Overlooked MOST DEADLY 30% 10% 60%
“Say the months of the year backwards? ” SAVEAHAART Alert Vigilant Lethargic Stuporous Will a stone float on water? Are there fish in the sea? Do 2 lbs weigh more than 1 lb? Can you use a hammer to cut wood? 94% sensitivity 89% specificity
� Out Patient �Restorative care �Treat pain minimize opioids �Hunger �Thirst �Sensory aids �Safety in Environment �Medicine reviews 30 -40% cases can be prevented Opioids Cholinergic drugs �Cognitive � Hospitals protocols Stimulation now have http: //www. americangeriatrics. org/files /documents/beers/Printable. Beers Pocket. Card. pdf
� Identify treat acute illness � Hyperactive � � � Use medication only if safety is compromised Low & Short � Start low � Use for short periods of time Haloperidol 0. 5 mg PO or IM � � Can repeat PO q 4 hrs IM q 1 Quetiapine 25 mg HS � PD � dementia
� Upon hospital discharge : � 47% still meet criteria of delirium � 1 month 33% � 3 months 26% � 6 months 21% � 2 years 55% of community dwellers will have dementia dx
� Increase risk of dementia in prolonged states � Death � Earlier LTC admission � Increase length of hospital stay �Progression to Dementia 65% vs 10% �Risk of not staying in home 33% vs 10% �Progression 38% vs 26% to death
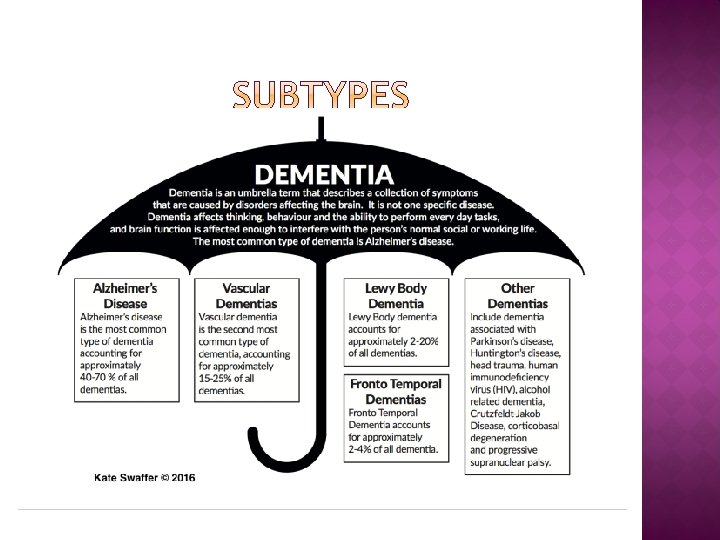
11%-28% >65 years old � 50% >80 years old � AD is 60 -80% of dementias � 2017 5. 5 mil Americans � Every 66 seconds some is dx with AD � 6 th leading cause of death � 1: 3 will seniors die from AD or other dementias � AD kills more than breast and prostate cancer combined � 35% of caregivers report their own worsening health after caring for their loved one with AD compared to 19% of loved ones w/o AD �
� MCI=more likely to develop AD or other dementia � 15 -20% � >65 years MCI does not always lead to dementia.
� 15% may convert to dementia � FORD �Finances �Orientation �Repeat questions �Direction
Normal Aging � Harder to recall info � Forget names � New acquaintances � Unable � Will � Walk to recall word remember later into room…. what did I come for � Forget were you put things Dementia � Memory impairs ability to function
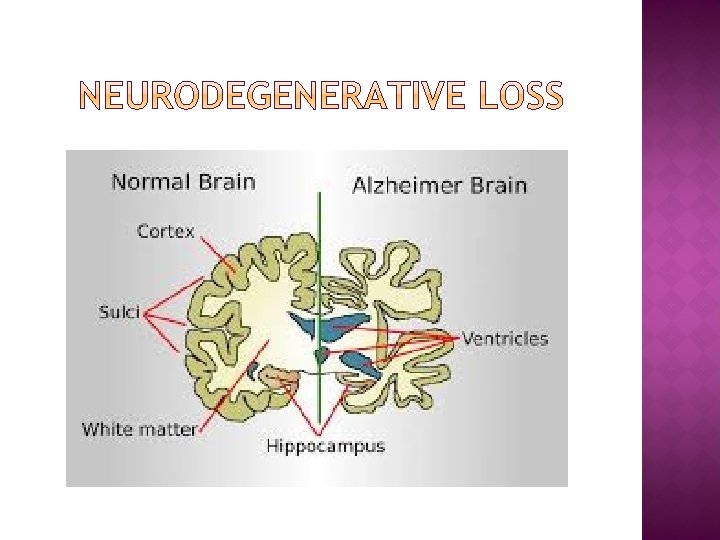
� Decline in Brain function leading to disruption in daily functioning Deficits � Memory impairment � Language � Visuospatial � Executive function � Lack of insight � Decline in social function
� Cognitive disability before memory impairment
� Age � HTN � HLD � T 2 DM � Obesity � Elevated levels of inflammatory markers � MCI � 50% Down Syndrome
� Ask Patient � Memory Worse? � Lost? � Repeat? � Help with ADLs? � Animal recall 60 secs 15 animals 4 items recall & read � <21 Insensitive to short-term memory 87% sensitive 82% specificity Ask Caregivers � What Boo’s? Has there been any consequences for memory loss? � Would you feel comfortable leaving your loved one for 1 month? � What are your doing now that you were not doing 6 mths ago? 24 -26/30 88 -100% Sensitivity 86% Specificity
� � � � � CMP CBC CT/MRI TSH FT 4 Folate Vitamin B 12 UA/culture Vitamin D 25 -OH Patient specific according to risks RPR � HIV � LP if suspicious for meningitis or Ca � CSF tap for NPH �
� Symptomatic � Behavioral disturbances � Support function � Provide for safety � Exercise � OT � Discuss palliative/hospice care � Try to maintain normality � Teach family � Do not try to reorient not argue � Community Resources � GPS tracker Educate!!!! Communicate!!!
� ACh. EI � Prevent breakdown of acetylcholine �Donepezil start 5 mg PO HS and titrate up to 10 mg �Rivastigmine 1. 5 mg PO BID 3 mg careful with titration in <50 kg 4. 6 mg/24 hrs Every 4 weeks max 9. 5 mg/24 h � NMDA-receptor antagonist � Selectively block excitotixic effects of abnormal transmission of glutamate �Memantine When Ch. EI contraindicated 5 mp PO daily Weekly titration to 20 mg in divided doses � Combinations �ACh. EI +Memantine advanced disease �MMSE <14 Mo. CA <14
� ASA � Women � Estrogen replacement � No � � Unconvincing evidence Bleeding Vitamin B and D � Medical food no clear evidence Ginkgo biloba � No benefit Axona � effect may increase incidence of dementia Cox-2 inhibitors � less cognitive decline ? Conflicting evidence for Testosterone Omeg-3 fatty Not effective
� Agitation � Aberrant motor behavior � Anxiety � Elation � Irritability � Depression � Apathy � Disinhibition � Delusions & hallucinations � Sleep or appetite changes.
� Cognitive/emotion-oriented interventions � reminiscence therapy � validation therapy � Sensory stimulation interventions � Acupuncture � Aromatherapy � light therapy � massage/touch � music therapy � Behavior management techniques � Other psychosocial interventions � animal-assisted � exercise. therapy
CNS Depression
� Akgün, K. M. , Crothers, K. , & Pisani, M. (2012). Epidemiology and Management of Common Pulmonary Diseases in Older Persons. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 67 A(3), 276– 291. http: //doi. org/10. 1093/gerona/glr 251 � Alz. org. Alzheimers Association. (2018). 2017 AD facts and figures. https: //www. alz. org/facts/ � Cerejeira, J. , Lagarto, L. , & Mukaetova-Ladinska, E. B. (2012). Behavioral and Psychological Symptoms of Dementia. Frontiers in Neurology, 3, 73. http: //doi. org/10. 3389/fneur. 2012. 00073 � Conwell, Y. , Van Orden, K. , & Caine, E. D. (2011). Suicide in Older Adults. The Psychiatric Clinics of North America, 34(2), 451– 468. http: //doi. org/10. 1016/j. psc. 2011. 02. 002 � Drummond, D. (2014). The Aging Brain: Dementia, Delirium and Depression. https: //www. youtube. com/watch? v=Aj. QQkx-zw 4 A � D'Souza, G. , Kakoullis, A. , Hegde, N. , Tadros, G. (2010). Recognition and management of abulia in the elderly. � Fiske, A. , Wetherell, J. L. , & Gatz, M. (2009). Depression in Older Adults. Annual Review of Clinical Psychology, 5, 363– 389. http: //doi. org/10. 1146/annurev. clinpsy. 032408. 153621 � Fong, T. G. , Tulebaev, S. R. , & Inouye, S. K. (2009). Delirium in elderly adults: diagnosis, prevention and treatment. Nature Reviews. Neurology, 5(4), 210– 220. http: //doi. org/10. 1038/nrneurol. 2009. 24 � Frank, Christopher. (2014). Pharmacologic treatment of depression in the elderly. Canadian Family Physician, 60, 121 -126. � Leth-Møller, K. B. , Hansen, A. H. , Torstensson, M. , Andersen, S. E. , Ødum, L. , Gislasson, G. , … Holm, E. A. (2016). Antidepressants and the risk of hyponatremia: a Danish register-based population study. BMJ Open, 6(5), e 011200. http: //doi. org/10. 1136/bmjopen-2016 -011200 � Manning, et al. (2013). Delirium. (2 nd ed. ) Stiriling: University of Striling/Hammond Press � National Alliance on Mental Health. (2009). Depression in Older Persons. https: //www. ncoa. org/wpcontent/uploads/Depression_Older_Persons_Fact. Sheet_2009. pdf � Tedeschini E. , Levkovitz, Y. , Lovieno, N. , Ameral, V. E. , Nelson, J. C. , Papkostas, G. I. (2011). Efficacy of antidepressants for late-life depression: a meta-analysis and meta-regression of placebo-controlled randomized trials. Journal of Clinical Psychiatry. Dec; 72(12 ): 1660 -8. doi: 10. 4088/JCP. 10 r 06531. � Robinson, S, , BPsych(Hons), Kissane, D. , Franz, C. P. , Brooker, J. , Burney, S. (2015) Systematic Review of the Demoralization Syndrome in Individuals With Progressive Disease and Cancer: A Decade of Research. Journal of Pain Symptom Management. (49)3, 595 -610. � Swaffer, K. (2016). Living beyond dementia. https: //livingbeyonddementia. com/tag/author-kate-swaffer 2016/ � Xue, Q. -L. (2011). The Frailty Syndrome: Definition and Natural History. Clinics in Geriatric Medicine, 27(1), 1– 15. http: //doi. org/10. 1016/j. cger. 2010. 08. 009 Progression in Neurology and Psychiatrics, Volume 14, Issue 6, November/December, p. 4– 28. DOI: 10. 1002/pnp. 178