Diabetes mellitus Zhang jinan Endocrinology Department of the
 Endocrinology Department of the First Affiliated Hospital, Medical")
Diabetes mellitus Zhang jin-an (张进安) Endocrinology Department of the First Affiliated Hospital, Medical College, Xi’an Jiaotong University
 : a syndrome Factors contributing to hyperglycemia may include DM causes")
Diabetes mellitus (DM) : a syndrome Factors contributing to hyperglycemia may include DM causes secondary pathophysiologic changes

Prevalence In China, 1980: 0. 67% 1994: 2. 51% 1996: 3. 21% In the world, 1997: 135 million 2000: 175 million 2025: 300 million

Diabetes mellitus result in • DM is the leading cause of blindness between the ages of 20 and 74 in the United States • Diabetic nephropathy is the leading cause of ESRD in the United States and a leading cause of DM-related morbidity and mortality • DM is the leading cause of nontraumatic lower extremity amputation in the United States. • coronary heart disease events and mortality are two to four times greater in patients with type 2 DM

Severe economic load of diabetes mellitus Medical cost of DM in USA (100 million USD per year)

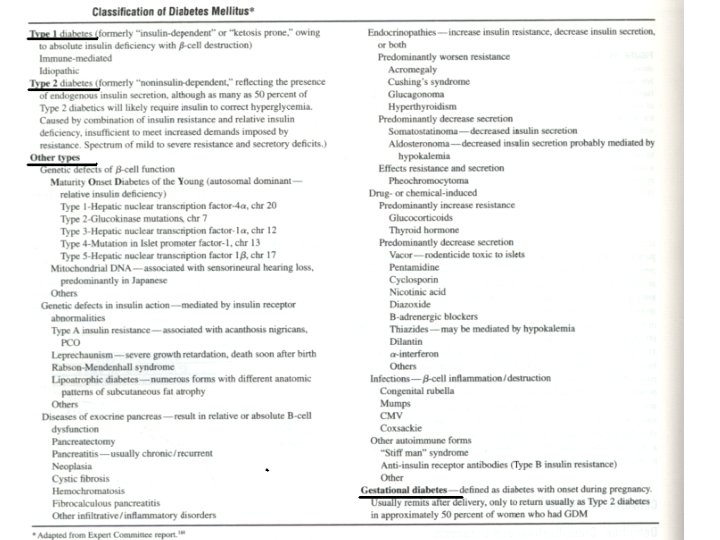
Etiologic Classification of Diabetes Mellitus • I. Type 1 diabetes (β-cell destruction, usually leading to absolute insulin deficiency) A. Immune-mediated B. Idiopathic II. Type 2 diabetes (may range from predominantly insulin resistance with relative insulin deficiency to a predominantly insulin secretory defect with insulin resistance) III. Other specific types of diabetes IV. Gestational diabetes mellitus (GDM)

• III. Other specific types of diabetes A. Genetic defects of β-cell function characterized by mutations in: • • • • Hepatocyte nuclear transcription factor (HNF) 4α (MODY 1) Glucokinase (MODY 2) HNF-1α (MODY 3) Insulin promoter factor (IPF) 1 (MODY 4) HNF-1β (MODY 5) Neuro. D 1 (MODV 6) Mitochondrial DNA Proinsulin or insulin conversion B. Genetic defects in insulin action Type A insulin resistance Leprechaunism Rabson-Mendenhall syndrome Lipodystrophy syndromes C. Diseases of the exocrine pancreas—pancreatitis, pancreatectomy, neoplasia, cystic fibrosis, hemochromatosis, fibrocalculous pancreatopathy D. Endocrinopathies—acromegaly, Cushing's syndrome, glucagonoma, pheochromocytoma, hyperthyroidism, somatostatinoma, aldosteronoma E. Drug- or chemical-induced—Vacor, pentamidine, nicotinic acid, glucocorticoids, thyroid hormone, diazoxide, β-adrenergic agonists, thiazides, phenytoin, α- interferon, protease inhibitors, clozapine, beta blockers F. Infections—congenital rubella, cytomegalovirus, coxsackie G. Uncommon forms of immune-mediated diabetes—“stiff-man” syndrome, antiinsulin receptor antibodies H. Other genetic syndromes sometimes associated with diabetes—Down's syndrome, Klinefelter's syndrome, Turner's syndrome, Wolfram's syndrome,
 1. Type 1 diabetes: absolute INS deficiency (Immune mediated, Idiopathic)")
Classification: (ADA 1997) 1. Type 1 diabetes: absolute INS deficiency (Immune mediated, Idiopathic) 2. Type 2 diabetes: INS resistance and relative INS deficiency 3. Other specific types: cause is clear 4. Gestational diabetes: during pregnancy determine if DM after 6 ws of delivery.
 genetic factors: concordance in")
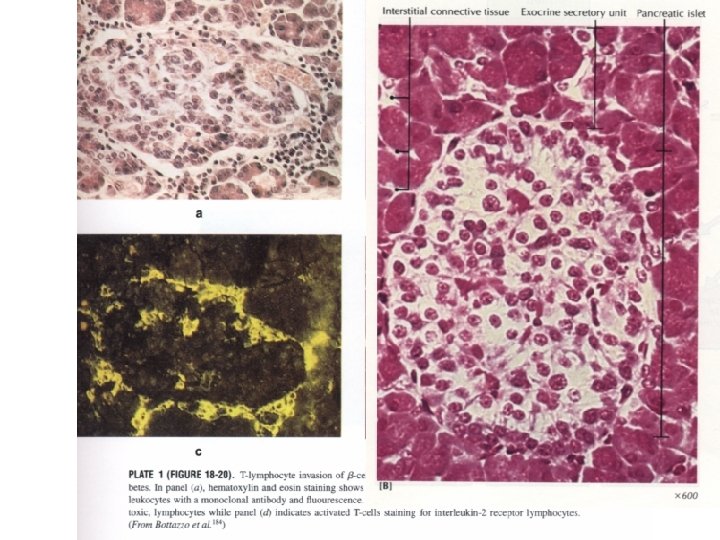
Etiology and pathogenesis 1. Type 1 DM : (1) genetic factors: concordance in identical twins 50% HLA-DR 3, DR 4 (+), DQA 1*0102, DQB 1*0602(-) at least 17 different genetic loci (2) autoimmune factors: insulitis: CD 4+/CD 8+, IL-1, TNF-α, IFN-γ ICAs(GAD, insulin, IA-2) (3) environment factors: virus infection: Coxsackie B, mumps chemicals: vacor, streptozotocinum; diet: bovine milk proteins
 ICA(+)")
H. E ICA(-) ICA(+)
 genetic factors: ---concordance in identical twins 70~90% --- Various")
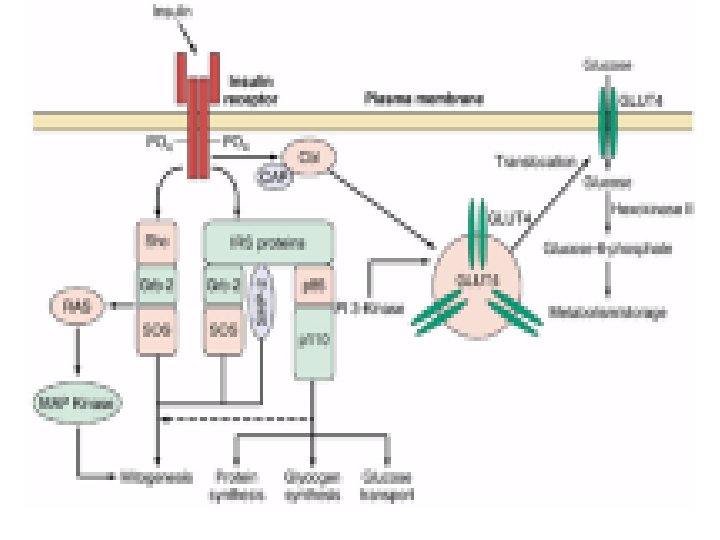
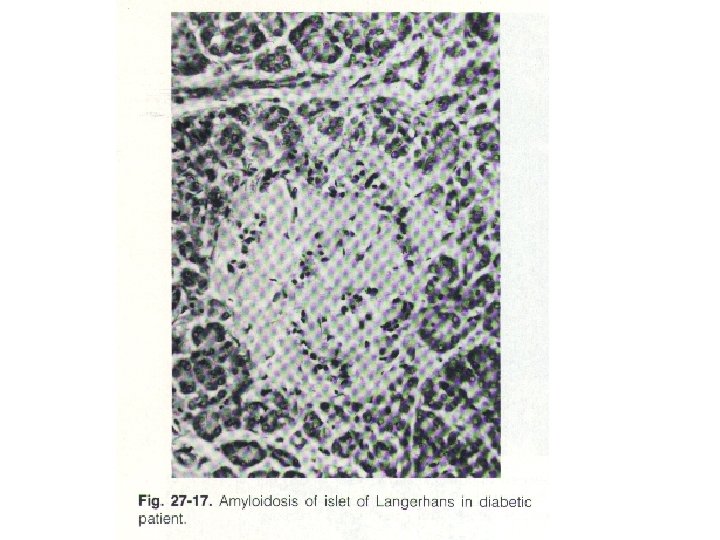
2. Type 2 DM: (1) genetic factors: ---concordance in identical twins 70~90% --- Various genetic loci (2) Environment factors: obesity: high calorie diet, less exercise INSULIN RESISTANCE (a) result: impairs glucose utilization; increases hepatic glucose output (b) molecular mechanism: postreceptor defects (Polymorphisms in IRS-1; GLUT 4 ) IMPAIRED INSULIN SECRETION (a) Heavy burden to islet cell (b) amyloid fibrillar deposit in islet (c) glucose toxicity (d) lipotoxicity
- Slides: 15