Chylous fistula after total thyroidectomy and radical lymph












.")







")




- Slides: 31
Chylous fistula after total thyroidectomy and radical lymph node dissection for anaplastic thyroid carcinoma Dr. Raad Al-Saffar, C. A. B. S consultant laparoscopic and thyroid surgeon Dr. Tarik Al-Shimmery, F. I. C. M. S. senior vascular surgeon Dr. Humam Alaa , MBCh. B, senior resident of general surgery.
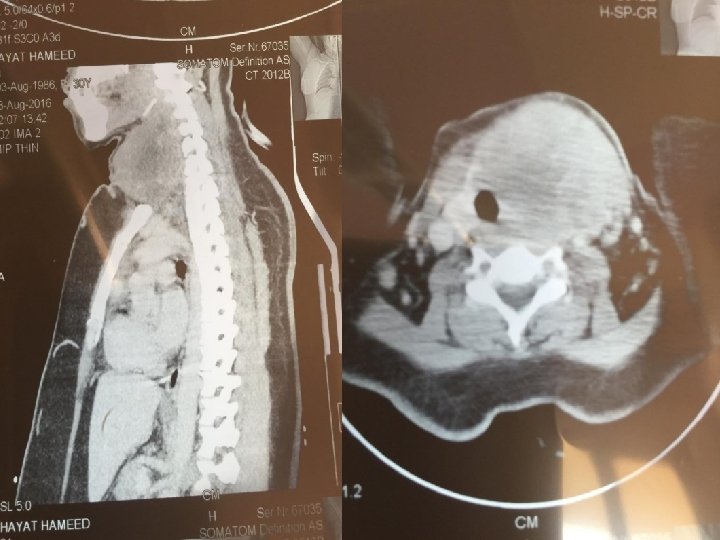
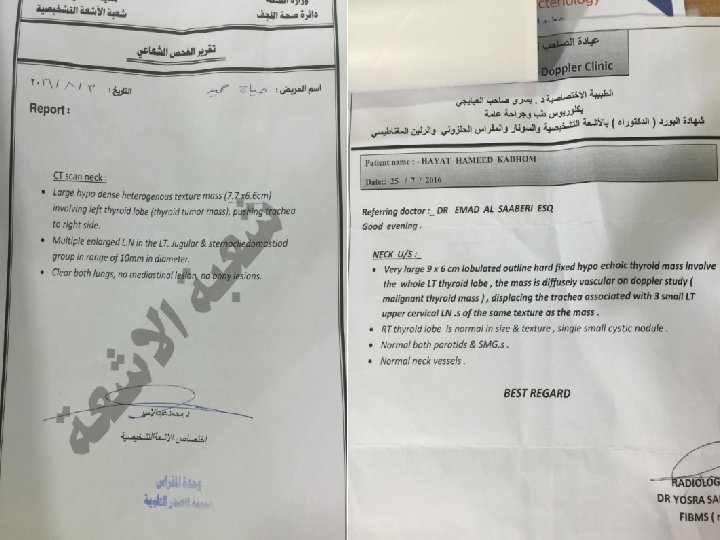
Case summary 40 years old female patient , she is a known case of anaplastic thyroid cancer which diagnosed one month ago after she had a neck swelling and addmitted for surgery. At first operation ( done by another surgeon) who did only biopsy and left tumor in situ. The histopathology result was anaplastic thyroid carcinoma. Imaging investigations were done for reassesment.
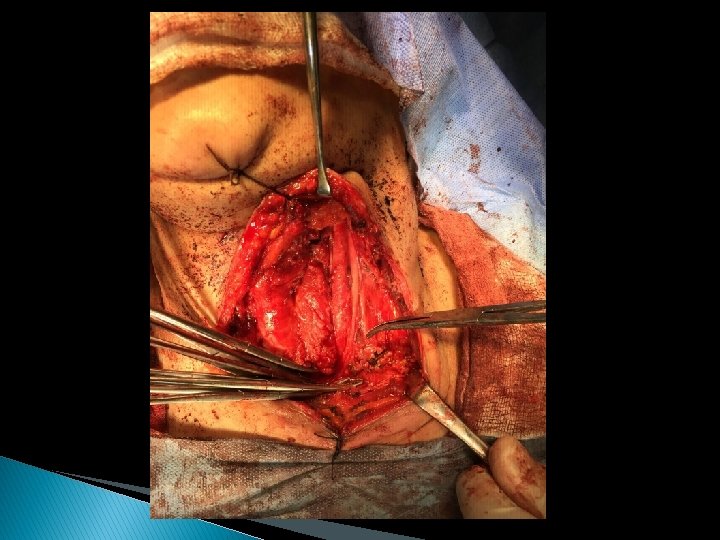
Operative notes � She had been addmitted for total thyroidectomy and neck dissection after preparation. � General anesthesia with endotracheal tube was given. � Supine position and hyperextention of the neck with mild degree head elevation. � Collar incision extended bilaterally parallel to anterior border of sternomastoid muscle up to angle of the mandible. � Upper and lower skin flaps were done.
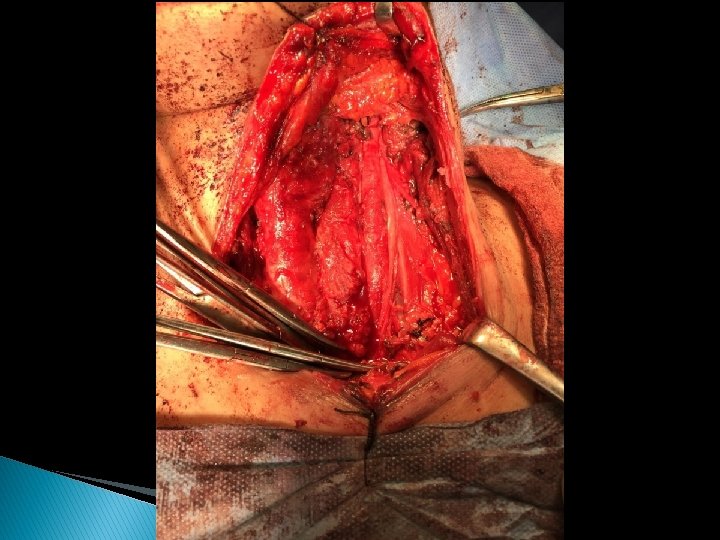
Operative procedure � Total thyroidectomy done with radical left lymph node neck dissection and selective right lymph node dissection: done by Dr. Raad Al-Saffar (thyroid surgeon) and Dr. Tarik Al-Shimmery(vascular surgeon) � Removing of all areolar tissues and lymph nodes at levels 2 , 3 , 4, 5 and 6.
Post operative follow up The vocal cords were normal on immediate postoperative examination. blood transfuion , aitibiotics and analgesia were given. Day 1 was uneventfull the drain content was serosanguineous discharge about 100 cc. per day. The patient discharged home at day 3 with drain of serous content of about 150 cc. per day. After 5 days drain was removed with few milleliters of serous fluid. At day 6 patient develop shotness of breath and neck swelling. On examination there is subcutaneos fluid collection. She addmitted and the drain inserted under local aneasthesia at site of previous drain. The discharge was thick and milky, first drainage about 300 ml.
So the diagnosis was chylous leak …. . The discharge was increased with oral feeding so we started trial of fat free diet and discharge amount decreased to 200 ml per day …. . After that she was discharged home with drain and advised to come back 3 days later …. Five days later she was addmitted because of continues and increased leak with generalized weakness and mild fever. Braod spectrum antibiotics was given with analgesia. The leak was about 600 ml/24 hrs and we started TPN with intralipid (MCT) and vamin as well as somatostatin subcutaneous injection.
� The discharge decreased gradually and stopped after 7 days of conservative treatment and drain was removed. � The patient referred to the oncology center for chemoradiation.
CHYLOUS FISTULA OF THE NECK
What is Chyle? Alkaline, milky, odourless fluid � 2 -4 L produced everyday � 1 liter of chyle contain : � 200 kcal � 20 -30 g of protein � 5 -30 g of fat �
FREQUENCY � Complication rate 1 - 2. 5% of neck dissection involving level IV. � predilection for the left side of the neck, but up to 25% of cases involve the right side of the neck.
ETIOLOGY �Post operative complication ◦ Radical neck dissection ◦ Selective neck dissection ◦ Anterior neck surgery �Penetrating trauma �Lymph node biopsy �Cervical rib excision
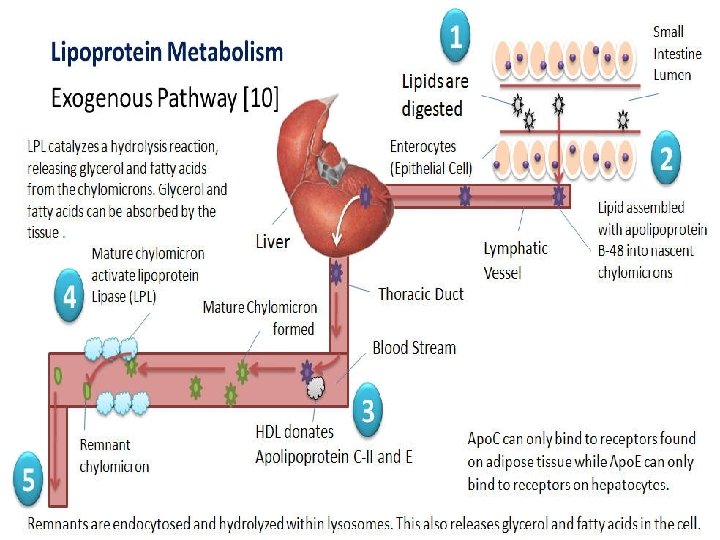
FAT METABOLISM 95% of ingested fats are triglycerides with long chain fatty acids (LCT). � These fats are re-esterified in the mucosal cells of the bowel wall, combined with an apolipoprotein and phospholipid and transported into the lymphatic system as chylomicrons. � Middle chain fatty acids (MCTs), length C 12 or less, are absorbed directly into the portal system without the formation of chylomicrons, bypassing the lymphatics; this is important in dietary therapy of chylous fistulas. �
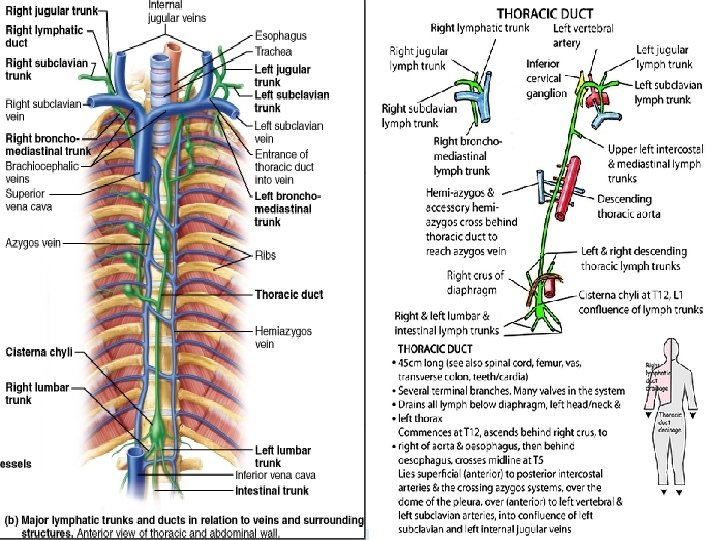
PATHOPHYSIOLOGY � � The thoracic duct is the conduit for lymph and dietary fat to reach the venous bloodstream. The flow of chyle is around 2 -4 L per day Consists of fat 1 -3% composed of TG (70% long chain), protein(3%), electrolytes content is the same as plasma except of lower calcium concentration, and lymphocytes (T lymphocyte). Its daily production is dependent on the diet and daily dietary intake.
The challenges in patient with chyle leak Hypoproteinemia � Hyponatremia � Hypochloremia � Dehydration � Emaciation � Lymphocytopenia and immunosupression � Pleural effusion - chylothorax � Wound problems - infection, suture breakdown, hemorrhage � Peripheral edema � Secondary sepsis �
MANAGEMENT OF CHYLE FISTULA Outline of management ◦ Nutritional modification ◦ Medical management ◦ Surgical management
Nutritional Management Goals of therapy ◦ Reduce chyle fluid production ◦ Replace fluid and electrolytes ◦ Maintain replete nutritional status and prevent malnutrition
Nutrition intervention � Fat free diet supplemented with MCT � TPN � Adequate protein intake ◦ Chyle contains significant amounts of protein (22 – 60 g/L)
Somatostatin � It decreases the intestinal absorption of fats, therefore TG concentration in the thoracic duct is lowered. � Somatostatin › reduces gastric, pancreatic and intestinal secretion. › It inhibit the motor activity of the intestine › slows the process of intestinal absorption › reduces splanchnic blood flow › decreases hepatic venous pressure
SURGICAL MANAGEMENT � Local procedures– ◦ reexploration of wound site after fat rich diet. ◦ And suturing with non absorbable suture or clips and local flap. ◦ Vicryl mesh overlay has been described. � Thoracoscopic approach ligation of TD. Right sided
Question & Answer from (Rush)
A 61 -year-old man with T 3 N 2 c. M 0 SCC of the supraglottic larynx undergoes total laryngectomy with left radical neck dissection / right modified radical neck dissection and primary pharyngeal closure without any intraoperative complications. Tube feeding is started on postoperative day 2. On day 3 the patient is noted to have increasingly high output of yellow/cloudy fluid from the left neck drain recorded to be 400 m. L over the past 24 hours. The hemoglobin concentration and white blood cell count are stable. The patient is afebrile with no signs of infection at the surgical site. What is the next most appropriate step in management? A. Immediate reexploration and closure of the pharyngeal Fistula. B. Thoracotomy with clamping of the thoracic duct. C. Closed wound drainage, pressure dressings, and tube feeding consisting of medium-chain triglycerides. D. Continuation of the current postoperative management. E. Removal of the left neck drain with a pressure dressing applied to the wound.
comment This patient has a chylous fistula. The initiation of tube feeding provided lipids to the lymphatic system, which increased the volume of chyle flow. Pharyngeal fistulas do not generally develop this early in the postoperative course and do not usually have such extremely high drain output. However, it is always something to consider after a pharyngeal repair. Chylous fistulas typically occur in the left side of the neck during radical neck dissections when dissecting low in the level IV/V region. The incidence is about 1% to 2%. If recognized at the time of surgery, they should be repaired immediately with ligature. If they occur in delayed fashion, such as in this patient, they can usually be initially managed conservatively, as stated in choice C.
The rationale for using medium-chain triglycerides is that they are absorbed directly through the portal circulation and not the lymphatic system. Another nutritional alternative in more severe cases is the use of total parenteral nutrition. In regard to deciding on surgical management, a general guideline accepted by many physicians is greater than 600 m. L of output over a 24 -hour period. Reexploration with control of the leak can be very difficult given the delicate nature of lymphatic tissue.
ANSWER: C