By Dr Amr Aly Abd El Moety Assistant


By Dr. Amr Aly Abd El Moety Assistant professor of Hepatology
 and refers to a bag or sack. The")
Ascites is of Greek derivation ("askos") and refers to a bag or sack. The word is a noun and describes. Pathologic fluid accumulation within the peritoneal cavity.

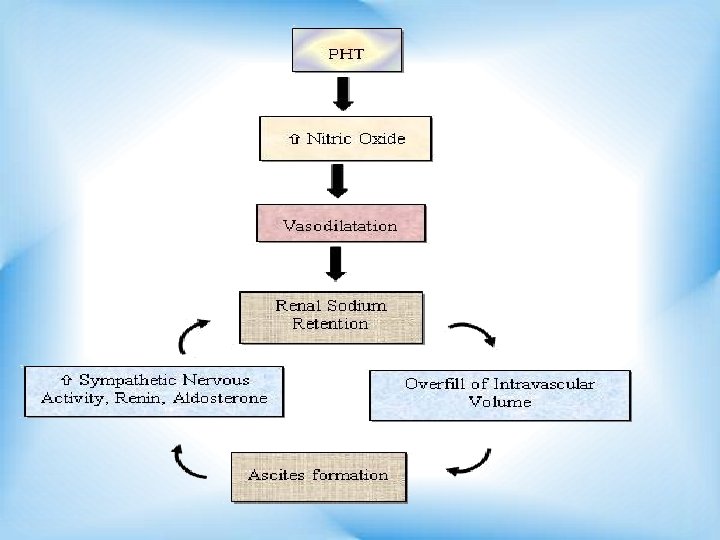
A- CIRRHOTIC ASCITES The most recent theory of ascites formation, the "peripheral arterial hypothesis, " proposes hypotheses, the that underfill vasodilation both and older overflow theories, are correct, but that each is operative at a different stage.

B- Noncirrhotic Ascites ü Peritoneal carcinomatosis: Appears to cause ascites through the production of proteinaceous fluid by tumor cells lining the peritoneum. Extracellular fluid enters the peritoneal cavity to reestablish oncotic balance. ü Massive liver metastases: Portal hypertension due to occlusion of portal veins by tumor nodules.

3. Hepatocellular carcinoma: Ascites forms because of the underlying cirrhosis-related portal hypertension, tumorinduced portal vein thrombosis, or both. 4. Chylous ascites: In patients with malignant lymphoma appears to be caused by lymph node obstruction by tumor and rupture of chyle-containing lymphatics.

5. High-output or low-output heart failure or nephrotic syndrome: As in cirrhosis, effective arterial blood volume appears to be decreased, and the vasopressin, renin-aldosterone, and sympathetic nervous systems are activated. These changes lead to renal vasoconstriction and sodium and water retention. 6. Tuberculosis, Chlamydia infection, and coccidioidomycosis: Probably cause ascites through the production of proteinaceous fluid, as in peritoneal carcinomatosis.
: Does not appear to cause fluid to accumulate; infection")
7. Spontaneous bacterial peritonitis (SBP): Does not appear to cause fluid to accumulate; infection develops only in preexisting ascites. 8. Pancreatic or biliary ascites fluid: Forms by leakage of pancreatic juice or bile into the peritoneal cavity or by a "chemical burn" of the peritoneum. 9. Abdominal surgery: Especially extensive retroperitoneal dissection, lymphatics may be transected.

Causes of Ascites 1. Liver Cirrhosis 6. Tuberculous peritonitis 2. Non alcoholic steatohepatitis 7. Acute hemorrhagic pancreatitis. 3. Alcohol 8. Fitz-Hugh-Curtis syndrome 4. Hepatocellular Carcinoma 9. Nephrotic syndrome 5. Congestive heart failure 10. Myxedema 11. Connective tissue disease

1. History of alcohol intake, intravenous drug use, blood transfusions, sex with a member of the same sex, acupuncture, tattoos, ear piercing, and country of origin. 2. Long-standing obesity (NASH). 3. Patients with a long history of stable cirrhosis and the sudden development of ascites should be suspected carcinoma. of harboring a hepatocellular

4. History of cancer malignancy-related ascites. However, cancer in the past does not guarantee a malignant cause of ascites. 5. History of heart failure may raise the possibility of cardiac ascites. Alcoholics in whom ascites develops may have alcoholic cardiomyopathy or alcoholic liver disease, but usually not both. 6. Tuberculous peritonitis is usually manifested by fever and abdominal pain.

7. Fitz-Hugh-Curtis syndrome caused by Chlamydia may cause inflammatory ascites in a sexually active woman. 8. Patients in whom ascites and anasarca develop in the setting of diabetes should be suspected of having nephrotic ascites. 9 Ascites in a patient with symptoms and signs of myxedema should prompt measurement of thyroid function. 9. Serositis in connective tissue disease may be complicated by ascites.

Full bulging abdomen should lead to percussion of the flanks. If they are dull then check for "shifting. " Approximately 1500 m. L of fluid must be present before dullness is detected.

is not worth testing for gaseous distention of the bowel, a thick panniculus, and an ovarian mass can mimic ascites. should be readily apparent on percussion.

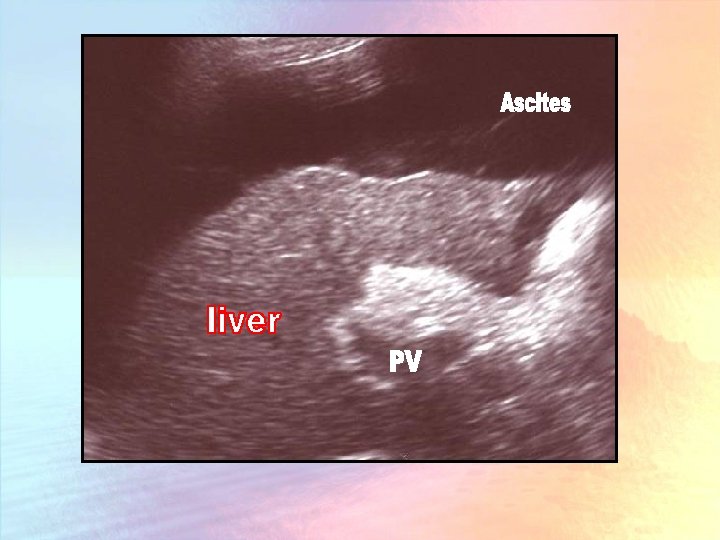
Ovarian masses usually cause tympanic flanks with central dullness. An obese abdomen may be diffusely dull to percussion, and abdominal ultrasonography may be required to determine if fluid is present.

Palmar erythema large abdominal wall collateral veins large pulsatile spider angiomata fetor hepaticus liver cirrhosis

Large veins on the patient's back suggests inferior vena cava blockage. An immobile mass in the umbilicus, the Sister Mary Joseph nodule, is suggestive of peritoneal carcinomatosis. Congested neck veins Constrictive pericarditis).

Determination of the cause of ascites is based on the results of the history, physical examination, and ascitic fluid analysis.

Indications: Ascitic fluid should be sampled in all inpatients and outpatients with the new onset of ascites and in all patients with ascites who are admitted to the hospital to exclude infection. Paracentesis should be repeated in patients with suspected infection. Contraindications: Coagulopathy

Gross Appearance 1 - If Neutrophil count >1000/mm 3 Fluid is clear If Neutrophil count <5000/mm 3 Fluid is cloudy If Neutrophil count < 50, 000/mm 3 Fluid resembles mayonnaise

2. RBC, S count < 10, 000 /mm 3, the ascitic fluid looks pink. But more than 20, 000/mm 3 it will be distinctly red. Traumatic: Ascitic fluid will clot. HCC Tuberculous Ascites Rupture lymphatics in liver cirrhosis. Peritoneal carcinomatosis

3. Chylous Ascites: Due to increase in Triglyceride level above 200 mg/d. L. 4. Dark brown colored Ascites indicates biliary perforation. 5. Hemorrhagic Black Ascites pancreatitis Malignant Melanoma

Ascitic Fluid Tests The WBC count in uncomplicated cirrhosis is less than 500 cells/mm 3. The absolute polymorphonuclear leukocyte count in uncomplicated cirrhosis is less than 250/mm 3.
")
is seen in Spontaneous bacterial peritonitis. Tuberculous peritonitis. Peritoneal carcinomatosis lymphocytes are mainly elevated)

Before the 1980 s, the ascitic fluid total protein concentration was used to classify ascites into exudates (>2. 5 g/d. L [25 g/L]) and transudates (<2. 5 g/d. L [25 g/L]). Unfortunately, this classification does not work well in ascitic fluid.
 ze either the total protein concentration or")
Serum albumin – Ascitic fluid albumin. AG) ze either the total protein concentration or other parameters do.
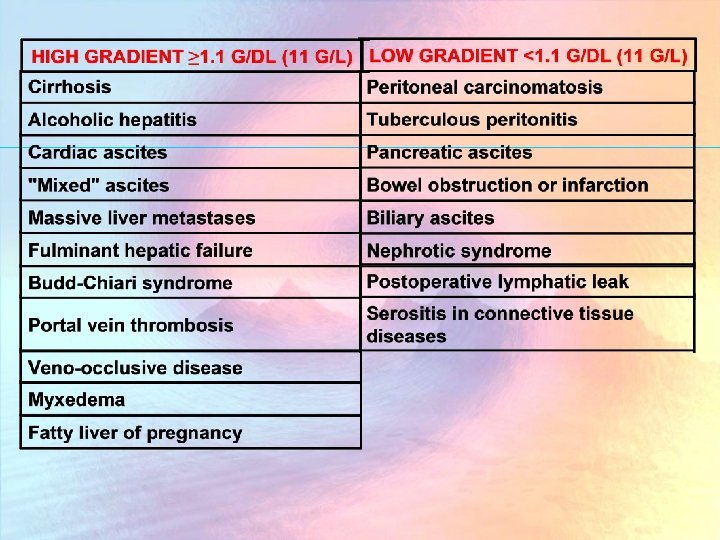

Blood culture is sensitive in detecting monomicrobial infection which is a feature of Spontaneous Bacterial Peritonitis. SAAG ratio is more sensitive in differentiating type evaluating total protein. of ascites than

In SBP and in the setting of gut perforation into ascitic fluid, the ascitic glucose concentration usually drops to 0 mg/d. L (0 mmol/L) because of large numbers of stimulated neutrophils and bacteria.

LDH enters ascitic fluid by diffusion from blood and by release from disintegrating ascitic fluid WBCs. In SBP, the ascitic fluid LDH level rises because of the release of LDH from neutrophils.

In patients with acute pancreatitis or gut perforation the ascitic fluid amylase concentration is elevated markedly, usually greater than 2000 U/L Bacteria are present only when there is an overwhelming infection, as in advanced SBP or asplenic pneumococcal sepsis.

The direct smear of ascitic fluid to detect mycobacteria is almost never positive because of the rarity of tuberculous peritonitis and the low concentration of mycobacteria in ascitic tuberculous peritonitis. fluid in

In contrast to a sensitivity rate of approximately 50% for mycobacterial culture ascitic with fluid optimal processing, laparoscopy with histology and culture of peritoneal biopsies has a sensitivity rate of approximately 100% in detecting tuberculous peritonitis.

To detect Malignant cells. Chylous ascites has a triglyceride concentration greater than 200 mg/d. L (2. 26 mmol/L) and greater than the serum level; usually the level is greater than 1000 mg/d. L (11. 30 mmol/L).
 and greater than")
Ascitic fluid bilirubin level greater than 6 mg/d. L (102 μmol/L) and greater than the serum level of bilirubin suggests biliary or upper gut perforation into ascites.

1 - Infection 1. SBP Positive ascitic fluid culture. . v *Elevated ascitic fluid absolute PMN count (i. e. , at least 250 cells/mm 3 [0. 25 × 109/L]). v No evidence of an intraabdominal surgically treatable source of infection. v 2. Polymicrobial bacterascites is diagnosed when Polymicrobial bacterascites is essentially diagnostic of gut perforation by the paracentesis needle.

Symptoms and Signs of Ascitic Fluid Infection Fever Abdominal pain Tender abdomen Rebound Altered mental status
, and Klebsiella. Polymicrobial bacterascites is by definition polymicrobial")
SBP Escherichia coli, streptococci (mostly pneumococci), and Klebsiella. Polymicrobial bacterascites is by definition polymicrobial

1. Low ascitic fluid total protein concentrations 2. Paracentesis Needle-induced ascitic fluid infections does not occur unless the bowel is penetrated by the paracentesis needle. 3. Gastrointestinal hemorrhage. 4. Urinary tract infections are also an underrecognized risk factor for SBP.

Patient with ascites who develop; Clinical deterioration Fever , abdominal pain, elevated PMN count.

Indications for Empirical Antibiotic Therapy of Suspected Spontaneous Ascitic Fluid Infection Ascitic fluid neutrophil count ≥ 250/mm 3 (0. 25 × 109/L) Convincing symptoms or signs of infection Intravenous Albumin Plus Antibiotic Intravenous albumin (1. 5 g/kg body weight at the time the infection is detected and 1. 0 g/kg on day 3) in combination with cefotaxime reduce the risk of renal failure and improve survival.

Treatment of Subtypes of Ascitic Fluid Infection Diagnosis Treatment Spontaneous bacterial peritonitis Five days of intravenous antibiotic to which the organism is highly susceptible (e. g. , cefotaxime 2 g every 8 hours empirically followed by more narrow spectrum therapy after susceptibility results are available) Polymicrobial bacterascites Intravenous third-generation cephalosporin (e. g. , cefotaxime 2 g q 8 h) plus an antianaerobic drug such as metronidazole. Duration is determined by clinical response and serial ascitic fluid PMN counts and cultures

Narrowing the Spectrum of Coverage After the results of susceptibility testing are available. Duration of Treatment 10 - 14 days of antibiotic therapy for lifethreatening infections. Follow-Up Paracentesis in Spontaneous Bacterial Peritonitis Not needed except after 48 hours if the course is a typical.

Prognosis v In the past, 48% - 95% of patients with a spontaneous ascitic fluid infection died. Now less than 5% of patients die. v Paracentesis should be performed at the time of hospital admission so that infection can be detected and treated promptly. v Paracentesis should be repeated during the hospitalization if any clinical deterioration occurs.

Prevention Norfloxacin 400 mg/day twice daily for 7 days. During hospital stay with discontinuation of the drug at the time the patient is discharged from the hospital.

Tense Ascites Tense ascites requires urgent therapeutic paracentesis. "Total paracentesis, " even more than 20 L, has recently been safe.

Pleural Effusions Unilateral and right-sided but occasionally may be bilateral. A unilateral left-sided effusion suggests tuberculosis. A large effusion in a patient with cirrhotic ascites is referred to as hepatic hydrothorax. It is due to small defects small defect in the right hemidiaphragm.

Symptoms Shortness of breath. Infection may complicate in case of SBP. Treatment 1 -Sodium restriction + Diuretics 2 -TIPS.

Abdominal Wall Hernias Umbilical, incisional or inguinal. Complications v Incarcerate or perforation. v Elective surgical treatment should be considered in all patients with hernias and ascites.

1. Nonovarian peritoneal carcinomatosis is treated by outpatient therapeutic paracentesis. 2. Ovarian malignancy have a good response to surgical debulking and chemotherapy. 3. Tuberculous peritonitis (without cirrhosis) is cured by antituberculous therapy. Diuretics do not speed weight loss unless the patient has underlying portal hypertension from cirrhosis.

5. A postoperative lymphatic leak from a distal splenorenal shunt or radical lymphadenectomy also may resolve spontaneously but on occasion may require surgical intervention or peritoneovenous shunting. 6. Chlamydia peritonitis is cured by tetracycline. 7. Ascites caused by lupus serositis may respond to glucocorticoids. 8. Dialysis-related ascites aggressive dialysis. may respond to

High Albumin-Gradient Ascites Treat the underlying liver disease eg drinking alcohol. stop Patients with other forms of treatable liver disease (e. g. , autoimmune hepatitis, hemochromatosis, or Wilson disease) should receive specific therapy for these diseases. Hospitalization For Patients with large-volume ascites and those who are resistant to outpatient treatment usually require hospitalization for definitive diagnosis and management of the fluid overload.
 per")
Diet Education Sodium restriction for inpatients and outpatients is 2 grams (88 mmol) per day. Fluid Restriction Not required No Bed Rest Urine Sodium/Potassium Ratio A random urine sodium/ potassium concentration ratio greater than 1 predicts that the patient should lose weight if the sodiumrestricted diet is followed.

Diuretics Spironolactone 100 mg + furosemide 40 mg. If the combination of spironolactone is ineffective in increasing urinary sodium or decreasing body weight, the doses of both drugs should be increased simultaneously as needed (e. g. , spironolactone 200 mg plus furosemide 80 mg, then 300 mg plus 120 mg, and finally 400 mg plus 160 mg).

Intravenous diuretics cause acute decreases in the glomerular filtration rate in cirrhotic patients with ascites and should be avoided. Once the reasonable edema maximum probably 0. 5 kg/day. has resolved, weight loss a is

Stop diuretics and reasse the situation if: A. Encephalopathy develops. B. Serum sodium concentration less than 120 mmol/L. C. Serum creatinine level greater than 2. 0 mg/d. L. (180 μmol/L). Reducing the quantity of fluid in the abdomen A. Improve the patient's comfort and prevent hepatic hydrothorax and hernias. B- Concentrating the ascitic fluid, diuresis increases the opsonic activity of fluid 10 -fold, and theoretically, may be of value in preventing spontaneous ascitic fluid infection.

Definition Ascites unresponsive to a sodium-restriction diet and high-dose diuretic treatment. Refractoriness is manifested by No weight loss or the development of complications of diuretics. Treatment; therapeutic liver transplantation, paracenteses, peritoneovenous shunts. TIPS, serial and
. v Paris pump: ultrafilterates ascitic fluid and")
Abandoned procedures: v Portacaval shunts: (for encephalopathy). v Paris pump: ultrafilterates ascitic fluid and reinfuse it intravenously. Unfortunately leads disseminated intravascular coagulation.
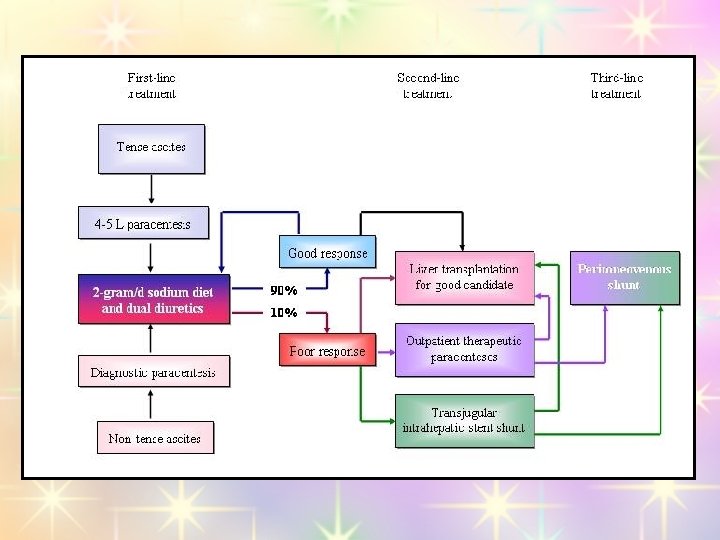

Liver Transplantation Orthotopic liver transplantation should be considered among the treatment options of patients with cirrhosis and ascites Serial Paracenteses Therapeutic paracentesis now appears to be first-line therapy for patients with tense ascites and second-line therapy for cirrhotic patients who are refractory to diuretics.

Colloid Replacement v Recent consensus statements and systematic reviews have pointed out some of the hazards of albumin infusion. 1. Avoid serial large-volume paracenteses in patients with diuretic-sensitive ascites. 2. Withhold albumin after taps of 5 L or less. 3. Consider albumin infusion optional after taps of larger volume in patients with diureticresistant ascites.
 For diuretic-resistant ascites. Peritoneovenous Shunt Patients who are")
Transjugular Intrahepatic Portosystemic Stent Shunt (TIPS) For diuretic-resistant ascites. Peritoneovenous Shunt Patients who are not candidates for liver transplantation and who have a scarred abdomen that is not amenable to repeated paracenteses or who have failed an attempt at TIPS make up this small subset of patients.
- Slides: 66