Atopic Dermatitis Immunology and management Dr Amal Kokandi
")



, SASSAD,")















 n Mild – “hydrocortisone” n Moderate – “eumovate” n Potent")
 n Class 1 (superpotent) n Class 2 (potent) n Class")






- Slides: 30
Atopic Dermatitis: Immunology and management Dr Amal Kokandi (MBBCh, DDSc, MD)
ECZEMA n Synonymous with dermatitis n Large proportion of skin disease in developed world n 10% of population at any one time n 40% of population at some time
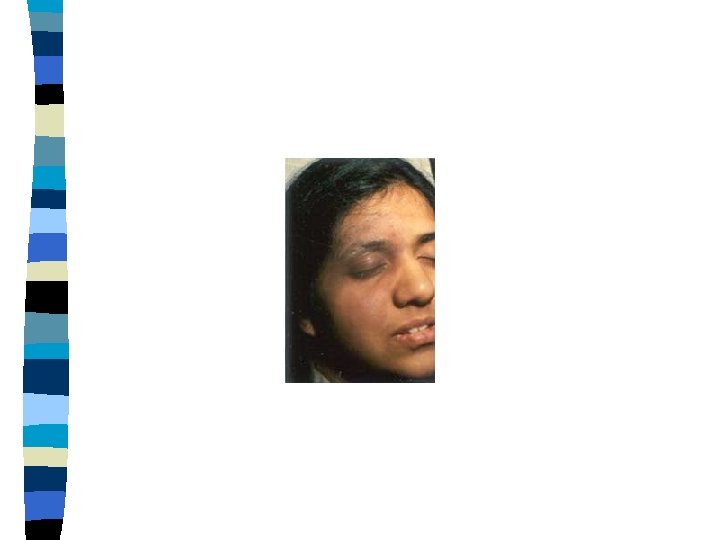
Features of eczema n n n n Itchy Erythematous Dry Flaky Oedematous Crusted Vesicles lichenified
Diagnosis n Clinical n No specific laboratory test n Family history of atopy is helpful n Criteria for research studies: Hanifin & Rajka (1980), United Kingdom Party Criteria (1994)
Severity n Clinical: Extent, sleep disturbance, Itching, Quality of life. – ADASI (diagramatic), SASSAD, SIS (intensity scoring), etc n Biophysical methods: – Eosinophils – Ig. E (80%) – Immunological markers (s. IL-2 R, ECP, s. CD 23, s. ICAM-1, s. ELAM-1, s. VCAM-1, E selectin, MBP…. . )
Atopic eczema n Endogenous n Atopic i. e asthma, hay fever n 5% of population n 10 -15% of all children affected at some time
Exacerbating factors n Detergents n Infection n Teething n Stress n Cat and dog fur n ? ? House dust mite n ? ? Food allergen
Clinical features n Itchy erythematous scaly patches n Flexures of knees and elbows n Neck n Face in infants n Exaggerated skin markings n Lichenification n Nail – pitted ridged
complications n Bacterial infection n Viral infections – warts, molluscum, herpes n Keratoconjunctivitis n Retarded growth
Pathogenesis n n n n Not fully understood Genetics Environmental factors: Irritants, aeroallergens, seasonal, hormonal and stress Microbial organisms (Staph Aureus, Malassezia, skin fungi. ) and superantigens Modified skin barrier function Deficiency in innate immune system and toll like receptors Specific immunity (biphasic Th 1 & Th 2)
Genetics of atopic eczema n 77% & 15% concordance in mono- & dizygotic twins. n significant linkage on chromosomes 1 q 21, 3 q 21 , 3 q 24 -22 , 3 p 26 -24 &17 q 25 n polymorphisms in genes important for epidermal differentiation, inflammation (IL-4, IL-12, Fillagrin…. )
investigations n Clinical n ? ? Ig. E n ? ? RAST
Prognosis n Most grow out of it! n 15% may come back – often very mildly
Treatment n n n n Patient education Emollients Avoid triggering factors: irritants especially soap Topical steroids Treat infections Sedating antihistamines Second line agents: Calcineurin inhibitors, UV therapy and systemic therapy Immunotherapy: Desensitization
creams n Cosmetically n Water more acceptable based n Contain preservatives n Soap substitutes
ointments n Oil based n Don’t contain preservative n Feel greasy n Good for hydrating
Topical steroids potency (European) n Mild – “hydrocortisone” n Moderate – “eumovate” n Potent – “betnovate” n Very potent – “dermovate”
Topical steroid potency (American) n Class 1 (superpotent) n Class 2 (potent) n Class 3 (potent) n Class 4 (midstrength) n Class 5 (midstrength) n Class 6 (mild) n Class 7 (least potent)
FTU n Finger tip unit n Helps to give estimation of topical steroid amount used n To avoid over and under use of steroid
FTU
Finger tip unit 2 FTU = nearly 1 gram n Enough for twice size of adult hand n – – – – A hand fingers (front and back) = 1 FTU A foot (all over) + 2 FTU Front of chest and abdomen = 7 FTU Back and buttocks = 7 FTU Face and neck = 2. 5 FTU An entire arm and hand = 4 FTU An entire leg and foot = 8 FTU
Special considerations n Face n Intertriginous areas n Children n Effect of occlusion n infections and combination formulas (with antibiotics and antifungals)
Topical steroid side effects n Perioral dermatitis and rosacea n Tachyphylaxis & steroid addiction n Infections (tinea incognito, herpes simplex, pityriasis versicolor, scabies……) n Adrenal suppression n Glucoma and cataract n Angina bullosa purpura (hard palate)
Topical steroid side effects § § § § Telangiectasia, purpura, epidermal, dermal and subcutaneous atrophy, striae, psuedoscars…… Folliculitis Allergic reactions Hypopigmentation Hypertrichosis Delayed wound healing Alteration in skin elasticity & mechanical properties tinea incognito