Antiseizure drugs and agents used in neurodegenerative diseases




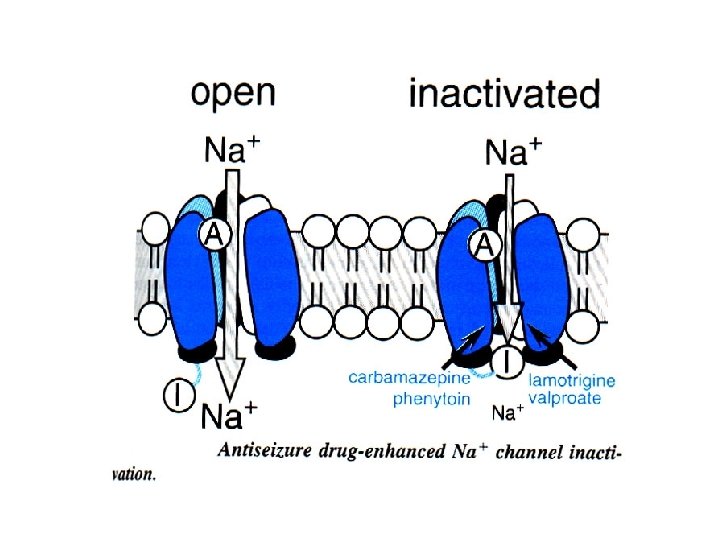
 synapse: - Presynaptic targets: • voltage gated Na⁺ channels: phenitoin, carbamazepine, lamotrigine")
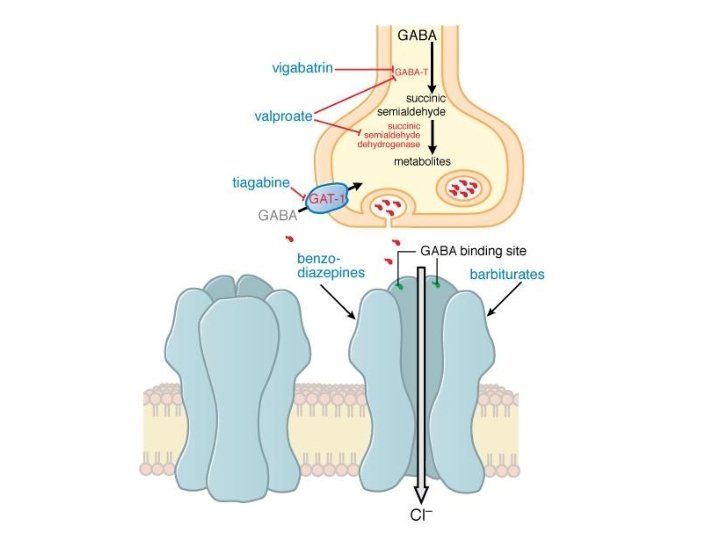
 synapse: 1. “specific”: -GABA transporters (GAT-1) -GABA - transaminase(GABA-T): vigabatrin -GABA A")







 •")




 are")



- Slides: 47
Antiseizure drugs and agents used in neurodegenerative diseases School of Medicine Split Department of Pharmacology
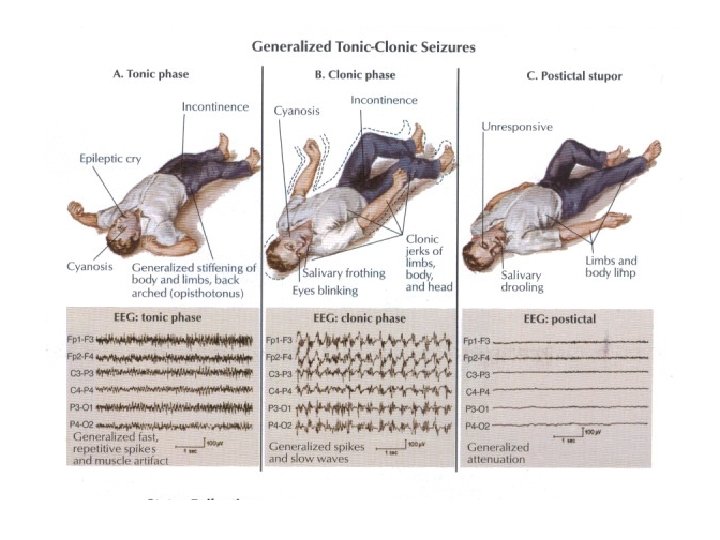
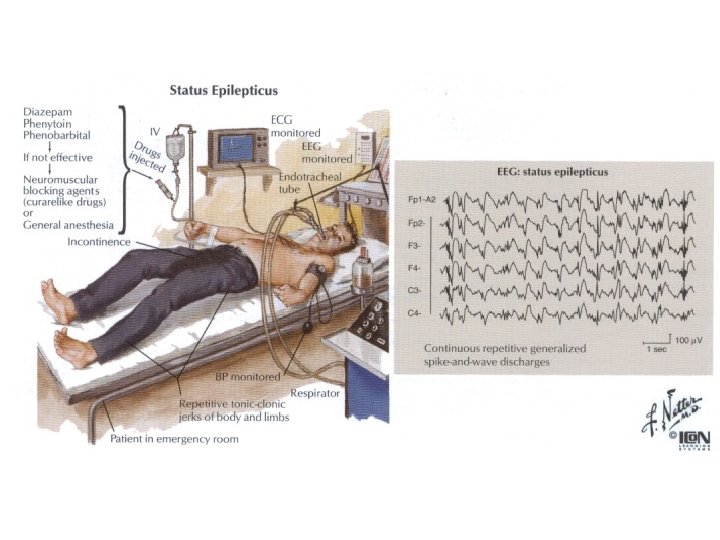
Antiseizure drugs Epilepsy = a chronic disorder characterized by reccurent seizures Seizure = finate episode of brain dysfunction resulting from abnormal discharge of cerebral neurons
MAXIMAL ELECTROSHOCK PENTYLENETETRAZOL In exp. animals the types of seizures can be induced by MES or PT. There is not a single antiepileptic drug.
http: //www. youtube. com/watch? v=r. TWGEf. Hr WNE http: //www. youtube. com/watch? v=N 20 bxt. C 0 RAo
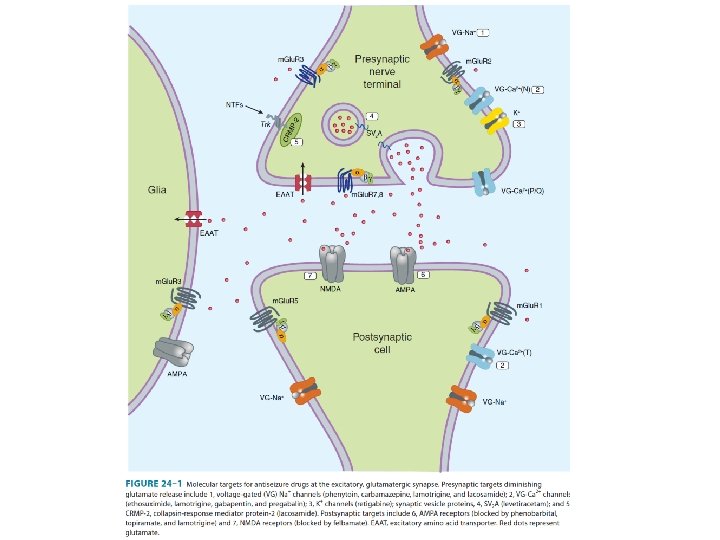
Excitatory (glutamatergic) synapse: - Presynaptic targets: • voltage gated Na⁺ channels: phenitoin, carbamazepine, lamotrigine • voltage gated Ca²⁺ channels: lamotrigine, ethosuximide • K⁺ channels, synaptic vesicle proteins, collapsin-response mediated protein-2 - Postsynaptic targets: • AMPA receptors: lamotrigine, phenobarbital • NMDA receptors
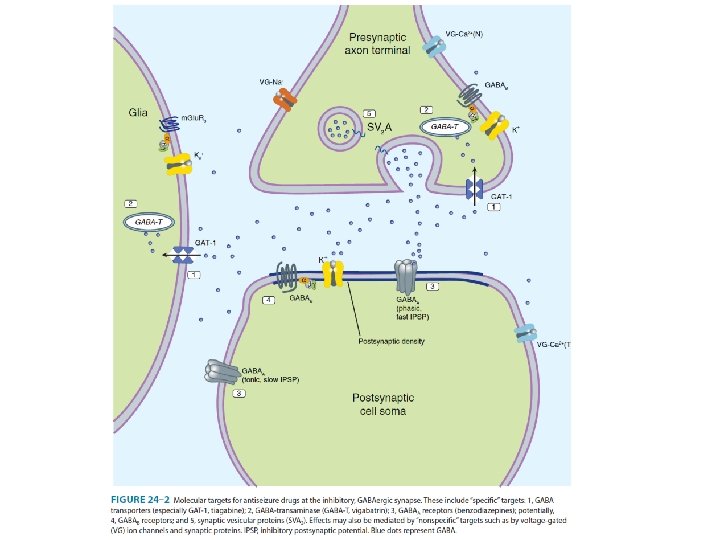
Inhibitory (GABA-ergic) synapse: 1. “specific”: -GABA transporters (GAT-1) -GABA - transaminase(GABA-T): vigabatrin -GABA A receptors: • benzodiazepines: diazepam, clonazepam, lorazepam • barbiturates: phenobarbital -GABA B receptors? ? , synaptic vesicular proteins 2. “nonspecific”: -voltage gated ion channels and synaptic proteins
1. 2. 3. 4. 5. BARBITURATES: X=C-N HYDANTOINS: X=N OXAZOLIDINEDIONES: X=O SUCCINIMIDES: X=C ACETYLUREAS: X=NH 2 The substituents determine the pharmacologic class, either anti-MES or anti-pentylenetetrazol
diphenylhydantoin Phenytoin: -partial and generalized clonic-tonic seizures-effective -generalized absence seizure-non-effective -Mechanisms of action: action the major action is to block Na⁺channels and inhibit the generation of rapidly repetitive action potentials; alters K⁺ and Ca²⁺ conductance; decreases the synaptic secretion of glutamate and enhances the release of GABA -Pharmacokinetics: -Pharmacokinetics route of administration: per os im. fosphenytoin (a more soluble prodrug) binding for plasma proteins: 90% distribution: accumulation in brain, liver, muscle and fat
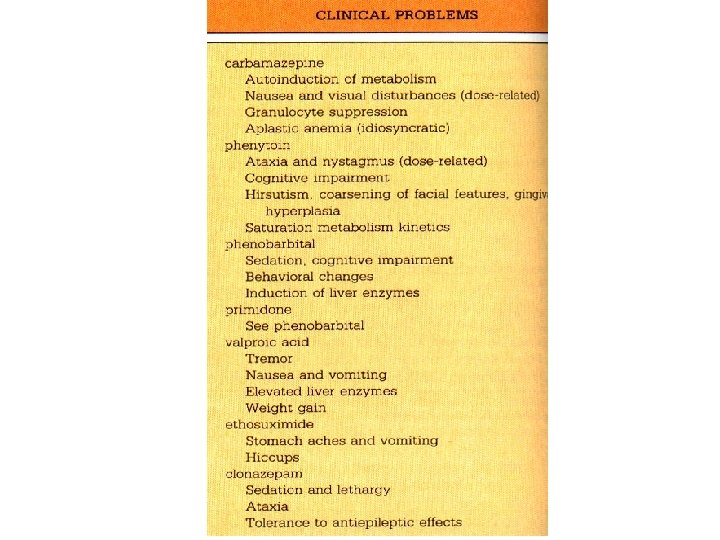
Phenytoin: -DOSAGE: DOSAGE starting dose is 300 mg/day (increasing no more than 25 -30 mg) -DRUG INTARACTIONS: INTARACTIONS induces microsomal enzymes, protein binding -ADVERSE EFFECTS: EFFECTS nistagmus, diplopia, ataxia gingival hyperplasia, hirsutism, abnormalities in vitamin D metabolism and osteomalacia, coarsening of facial feautures, peripheral neuropathy, skin rash The elimination of phenytoin is dose-dependent, follows 1 st order kinetics at small concentrations; as blood levels rise within therapeutic range, the maximum capacity of liver to metabolize phenytoin is approached
ureide moiety Carbamazepine: -partial and generalized clonic-tonic seizures-effective -generalized absence seizure-non-effective -trigeminal neuralgia; (mania in) bipolar depressioneffective -Mechanism of action: action the major action is to block Na⁺channels and inhibit the generation of rapidly repetitive action potentials, descreases synaptic transmission, potentiate volatage-gated K⁺ current
-DOSAGE: DOSAGE several times a day 1 -2 g - DRUG INTARACTIONS : induction of hepatic microsomal enzymes!!!! (CYP 3 -A 4) - ADVERSE EFFECTS diplopia and ataxia, gastrointestinal upsets, hyponatriemia with water intoxication, leukopenia, erythematous skin rash (idiosincratic)
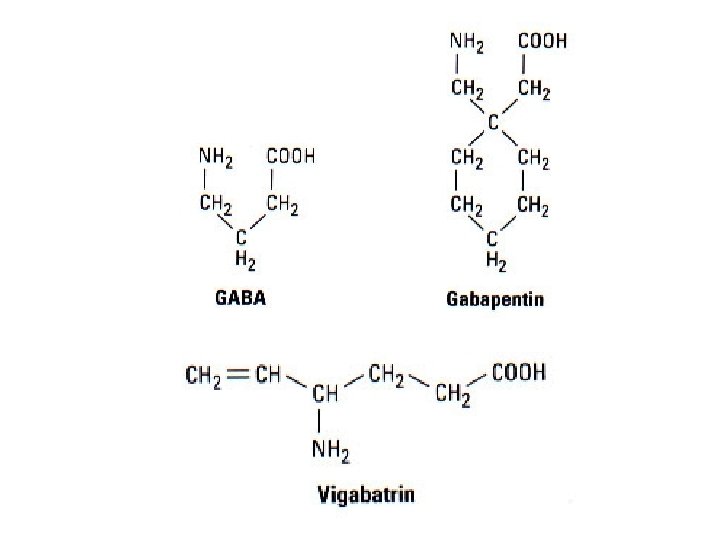
VIGABATRIN: -complex partial seizures, infantile spasmseffective -MECHANISMS OF ACTION: ACTION irreversible inhibition of GABA-aminotransferase -per os -DOSAGE: DOSAGE several times a day 2 -3 g -INTERACTIONS: -INTERACTIONS relative contraidication is psychosis -ADVERSE EFFECTS: EFFECTS drawsiness, dizziness, weight gain, agitation, confusion, psychosis, peripheral visual field defects
LAMOTRIGINE: -monotherapy for partial seizures; absence, myoclonic seizures, Lennox-Gastaut syndrome-effective -MECHANISMS OF ACTION: ACTION the major action is to block Na⁺channels and inhibit the generation of rapidly repetitive action potentials; Ca²⁺ conductance; decreases the synaptic secretion of glutamate -DOSAGE: DOSAGE 200 -300 mg/day -INTERACTIONS: -INTERACTIONS valproate couses a two-fold increase in the half-life of lamotrigine -ADVERSE EFFECTS: EFFECTS dizziness, headache, diplopia, somnolence, nausea and skin rush,
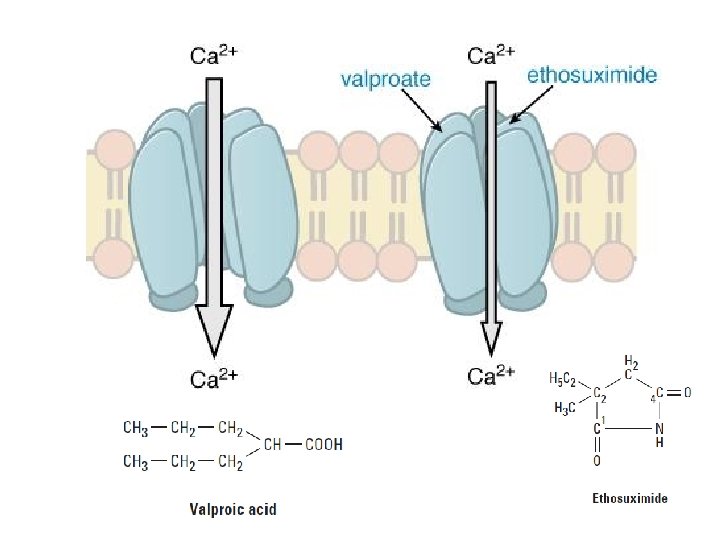
VALPROIC ACID AND SODIUM VALPROATE: • CHEMISTRY: CHEMISTRY monocarbocylic acid (8 C atoms) • Clinical uses: absence and clonic-tonic seizures • Mechanisms of actions: Na⁺ and Ca ²⁺- channels inhibition and decreased GABA degradation • Adverse effects: - hair loss, anorexia, nausea, vomiting - hepatotoxicity (children) - teratogenicity Inhibition of drugs that are metabolized by CYP 2 C 9 (phenitoin, phenobarbital)!
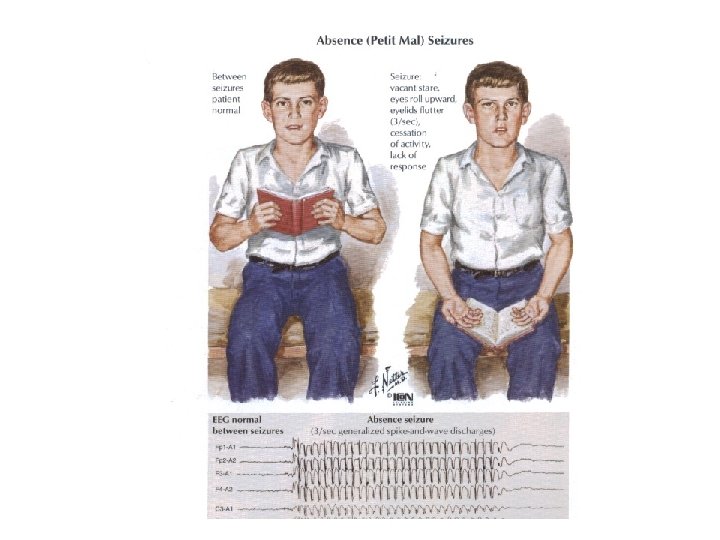
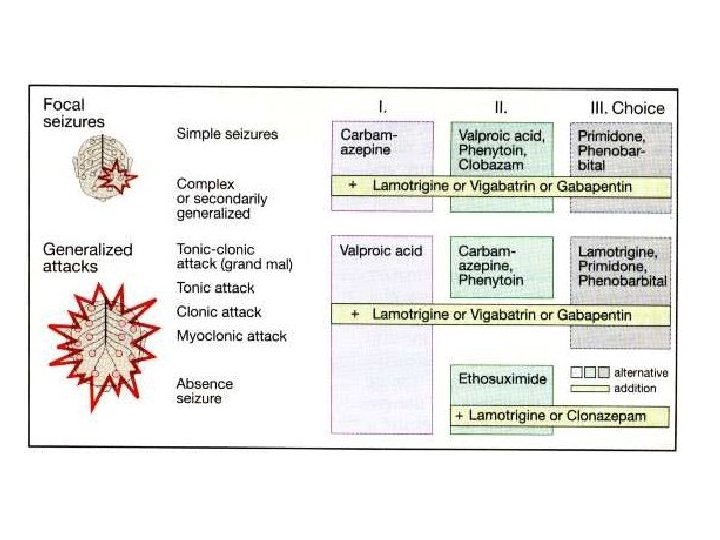
Parcial seizures with or without secondary generalization: 1. carbamazepine 2. Na valproate 3. phenytoin GENERALIZED SEIZURES: Tonic-clonic seizures (grand mal): 1. carbamazepine 2. phenytoin 3. Na valproate 4. barbiturates Absence seizures (petit mal): 1. ethosuximide 2. Na valproate
SEIZURES AND PREGNANCY 0, 5 -1% Pregnancy planning Follic acid PHENYTOIN PHENOBARBITAL CARBAMAZEPINE ETHOSUXIMIDE VALPROIC ACID D LAMOTRIGINE C
AGENTS USED IN NEURODEGENERATIVE DISEASES 1. Drugs used in Parkinson’s disease 2. Drugs used in Alzheimer’s disease (Rivastigmine)
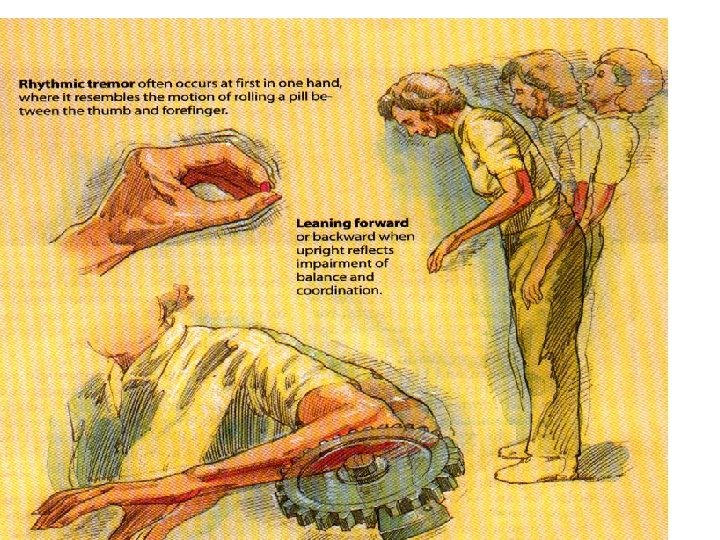
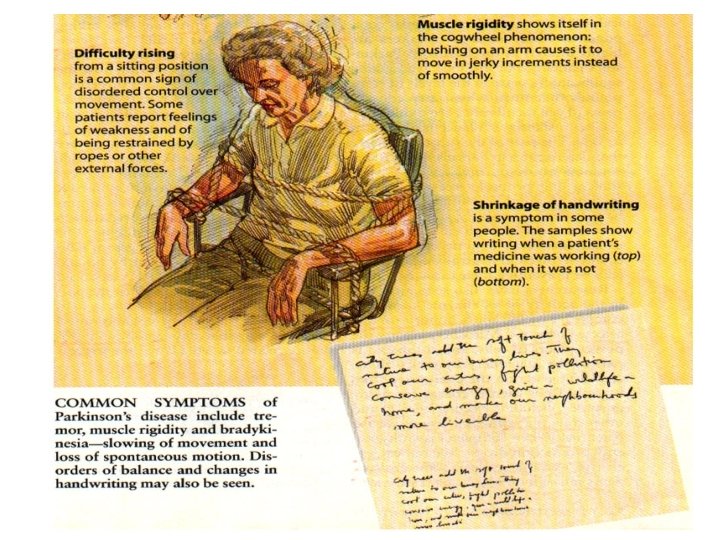
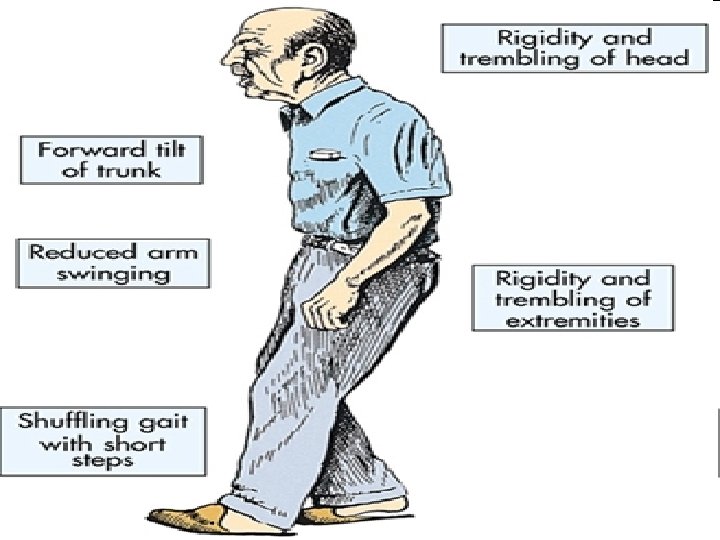
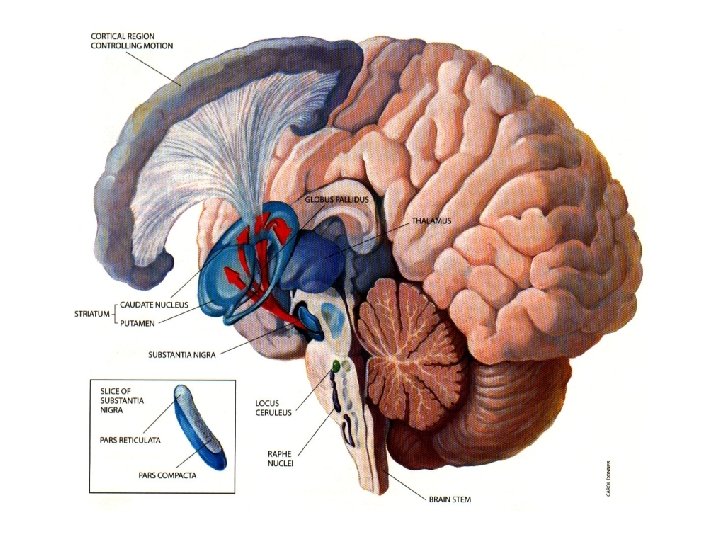
Parkinson’s disease • Definition: - Progressive neurodegenerative diseaseof the basal ganglia causing: - tremor at rest - hipokinesia - muscle rigidity -often with dementia and autonomic dysfunction
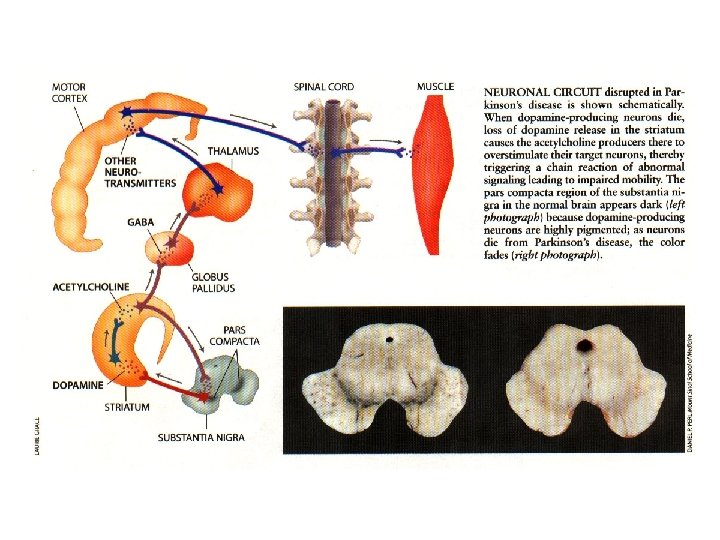
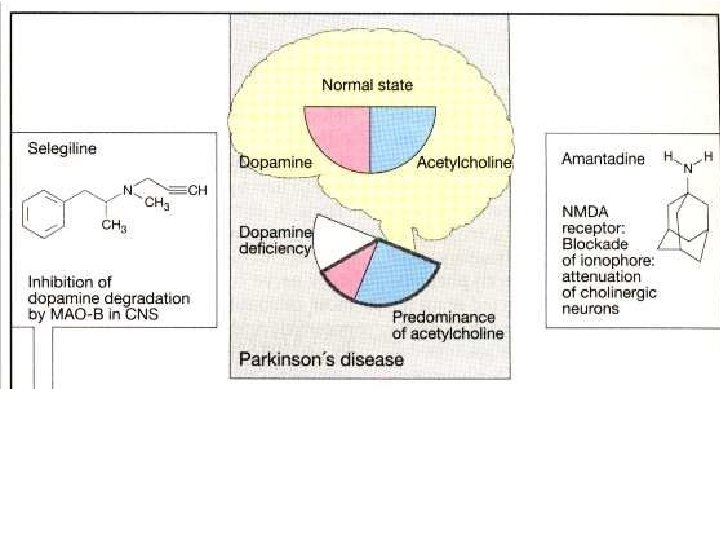
NEUROCHEMICAL CHANGES: • Low level of dopamine • Other monoamines (noradrenaline and serotonine) are much less affected • Gradual loss of dopamnine occurs over several years with symtoms of PD appearing only when the striatal dopamine content has fallen to 20 -40 % of normal • The symtom most clearly related to dopamine defficiency is hypokinesiawhich occurs immediately • Hyperreactivity of cholinergic neurons contributes significantly to the symtoms of PD
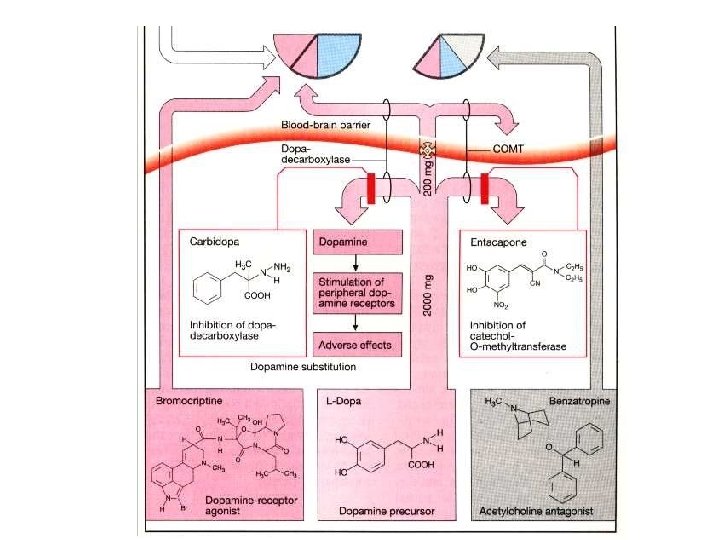
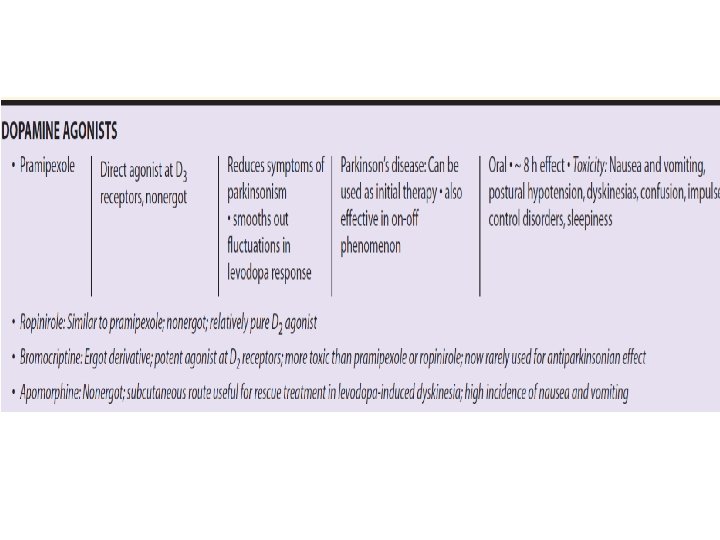
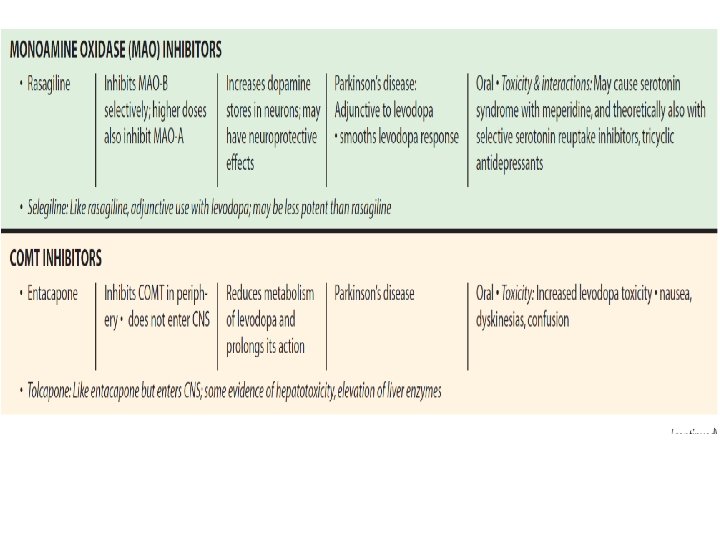
DRUGS: None of the drugs affects the progression of the disease! - drugs that replays dopamine(Levodopa; Levodopa + Carbidopa) - inhibitors of catechol-O-methyl transferase (Entacapone) - drugs that act as dopamine, agonists of dopamine receptors (Bromocriptine, Pramipexole) - MAO-B inhibitors (Selegiline) - drugs that can increase dopamine release (Amantadine) - Acetylcholine antagonists (Benz(a)tropine, Biperiden)
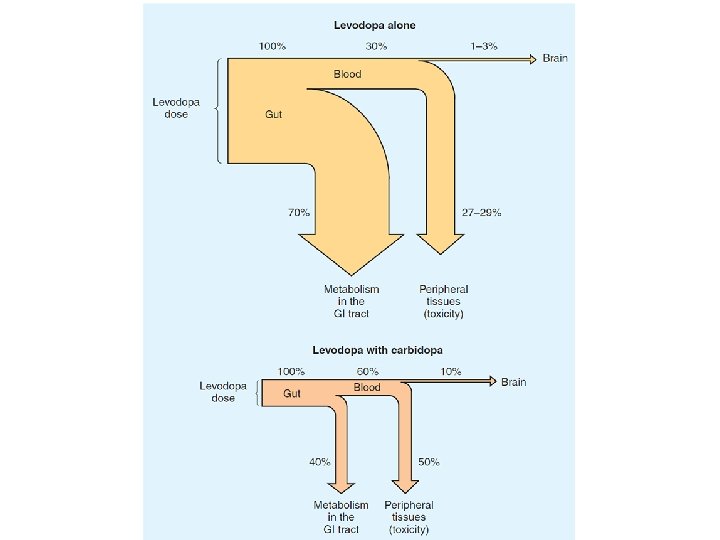
LEVODOPA • Dopamin does not penetrate the blood-braine barrier. The immediate precursor of dopamine LEVODOPA enters the brain where it is decarbocylated to dopamine • Only about 1 -3 % of administered levodopa actually enters the brain unaltered; the reminder is metabilized extracerebrally into dopamine • It is given in combination with a peripheral dopa decarboxilase inhibitor (carbidopa); peripheral metabolism is reduced, plasma levels are higher and half-life is longer
Therapeutic efficacy • Particulary effective in …. relieving bradykinesia Adverse effects • After 3 or 4 years of • Dyskinesias (choreoathetosis of treatment the benefits the face and distal extremities. begin to diminish • Fluctuation in clinical response: 1. wearing-off or and-of–doseakinesia 2. unrelated to the timing of dose, on-off phenomenon (off - periods of marked akinesia alternate over the course of few hours with on – peiods with improved mobility but marked dyskinesias