Anatomy FEMALE PELVIC THE PELVIS protective shield supports






")








 is")


- Slides: 31
Anatomy FEMALE PELVIC
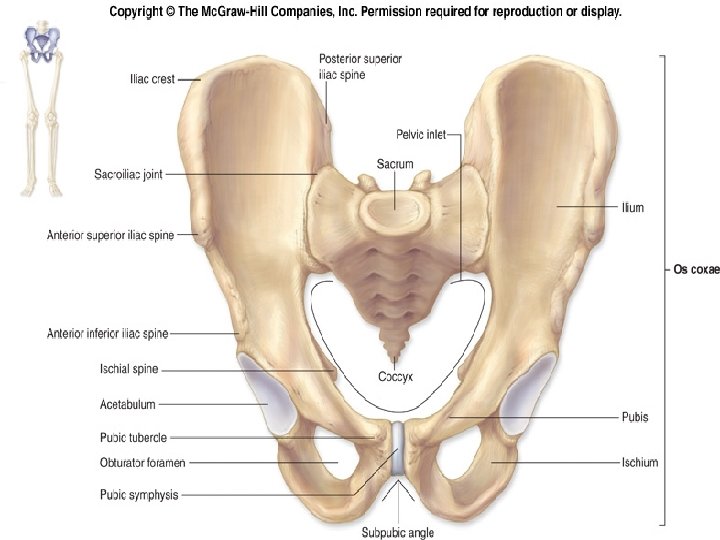
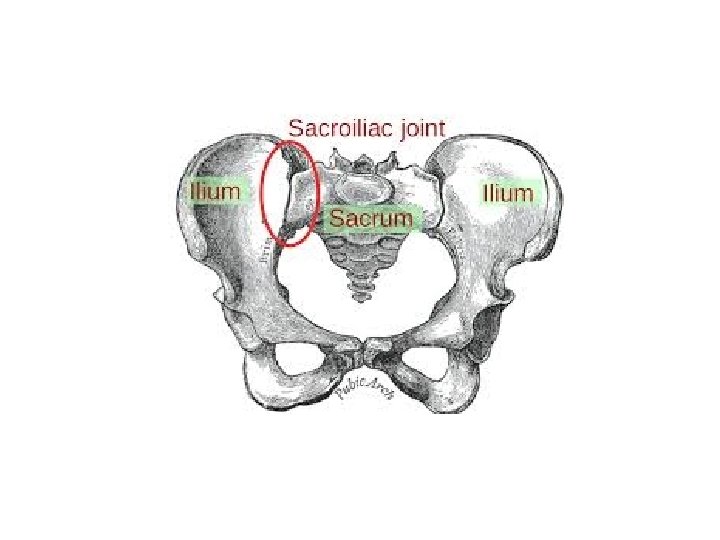
THE PELVIS • protective shield • supports the trunk pelvis consists of 1. the two innominate bones and the 2. sacrum to which 3. coccyx is attached • The Right and left Innominate bones anteriorly articulate at Symphysis Pubis, innominate and the sacrum articulate at the sacroiliac joints, to form a firm bony ring.
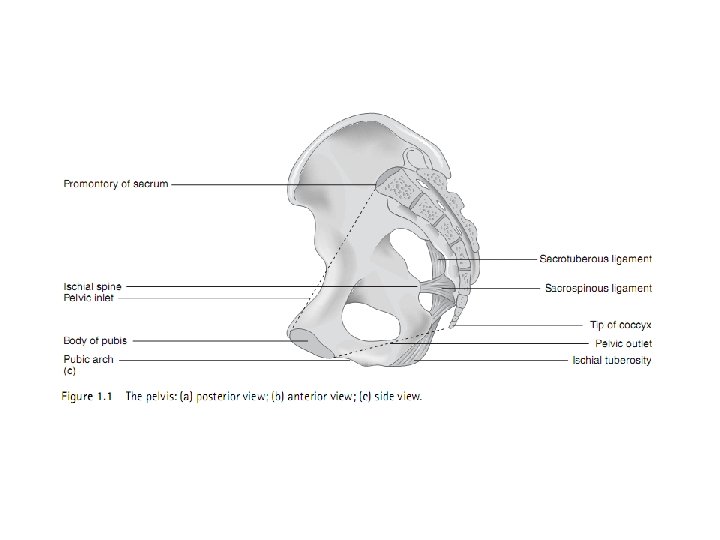
• The ring of bone is deeper posteriorly than anteriorly and forms a curved canal. • The inlet to this canal is at the level of the sacral promontory and superior aspect of the pubic bones
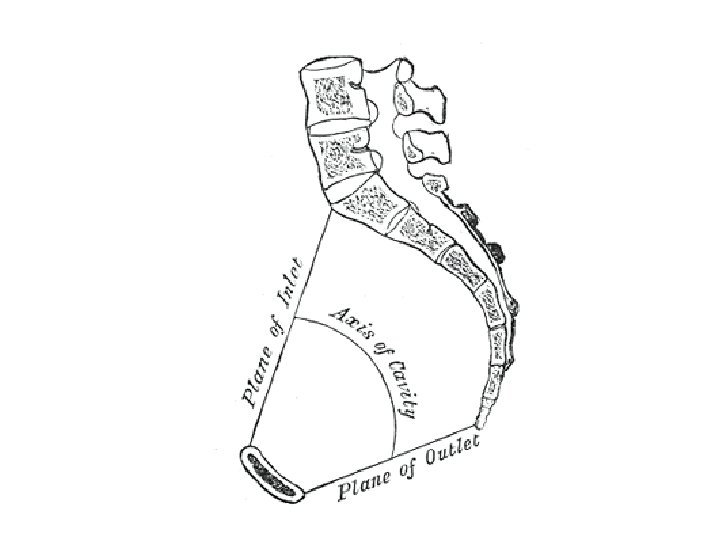
• The outlet is formed by the pubic arch, ischial spines, sacrotuberous ligaments and the coccyx. • The enclosed space between the inlet and outlet is called the true pelvis, with the plane of the inlet being at right angles to the plane of the outlet.
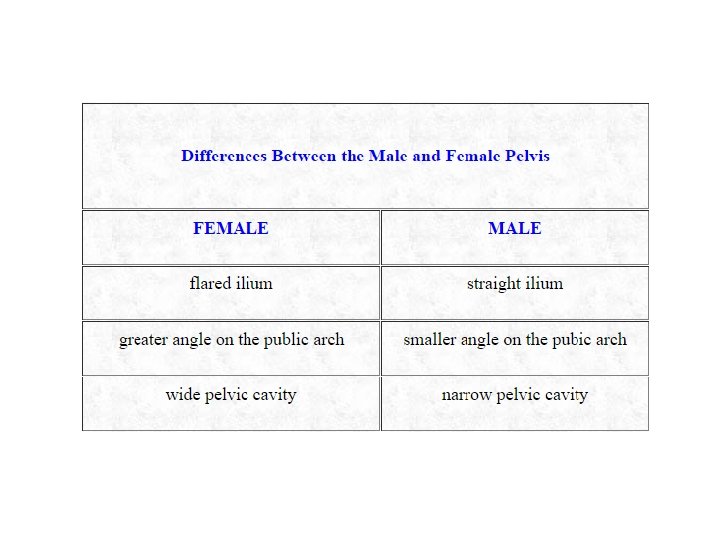
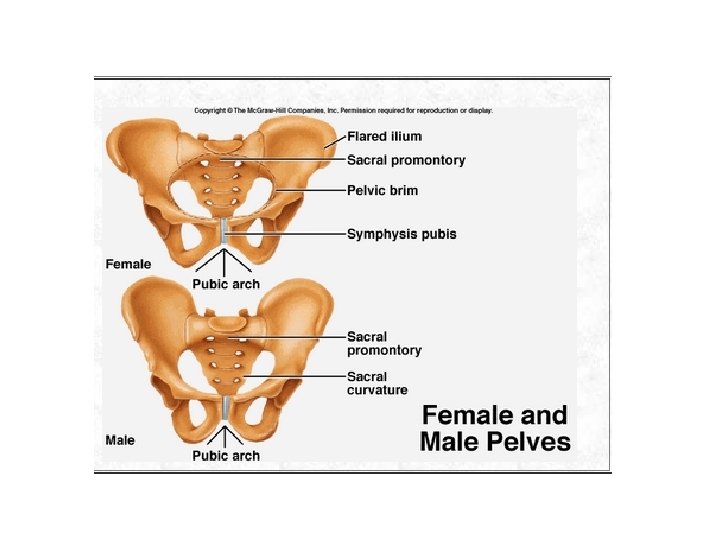
Difference from Male Pelvis The female true pelvis differs from the male in being • shallower, • having straighter sides (Flared Ileum) • wider angle between the pubic rami at the symphysis (More angle of Pubic Arch) • proportionately larger pelvic outlet. • Pelvic Inlet is oval in Female, Heart shape of male • Wide pelvic Cavity
Female Pelvic Inlet Pelvic Outlet Pelvic Cavity Pelvic Arch Male
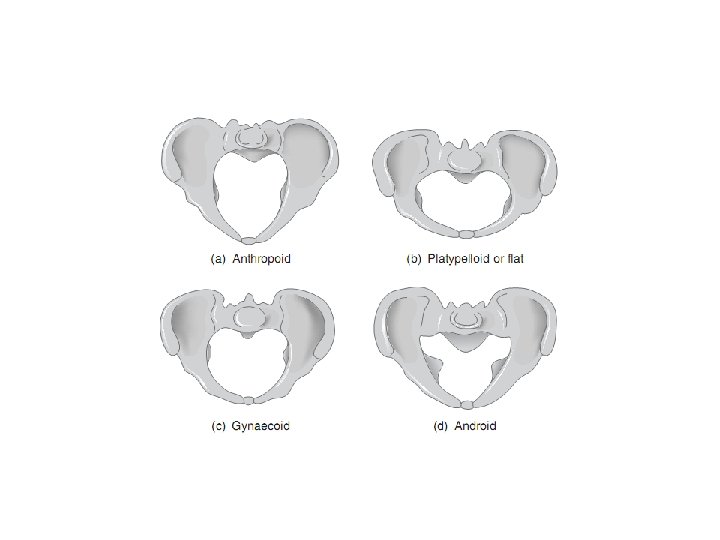
Types of Pelvis • • Gynaecoid Anthropoid Android Platypelloid (Flat)
• The ideal or Gynaecoid pelvis is recognized by its well-rounded oval inlet
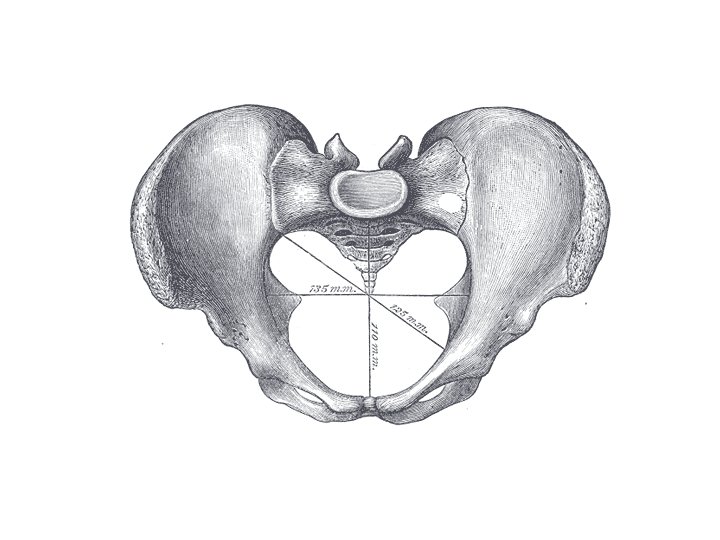
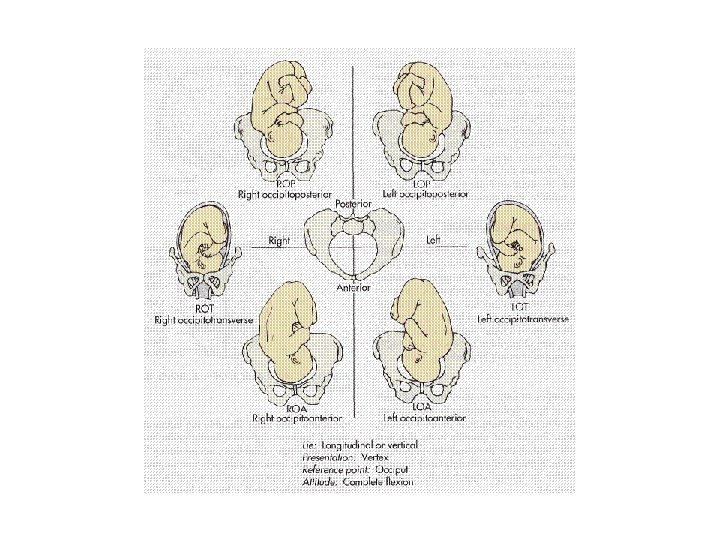
Dimensions of Inlet and Outlet • The inlet has its longest dimension from side to side (i. e. transverse 33 m), whereas at the outlet the longest dimension is anteroposteriorly (33 cm)
• The fetal skull is longest in its anteroposterior dimension. • Most commonly in labor the head enters the inlet of the maternal pelvis transversely placed (i. e. long axis to long axis), rotates in mid-cavity and leaves by the outlet with its longest dimension lying anteroposteriorly.
Different shapes of pelvic
Difficulties in Child Birth • Difficulties can be experienced in childbirth from such adverse features as 1. Protuberant ischial spines, 2. A heart-shaped inlet produced by an invasive sacral prominence, or 3. An asymmetrical pelvis (e. g. as a result of rickets or trauma). 4. It is also possible for the inlet or outlet to be too small to allow the fetal head to pass through 5. It has recently been demonstrated that a narrow suprapubic arch is associated with a consequential prolonged labor and postpartum anal incontinence
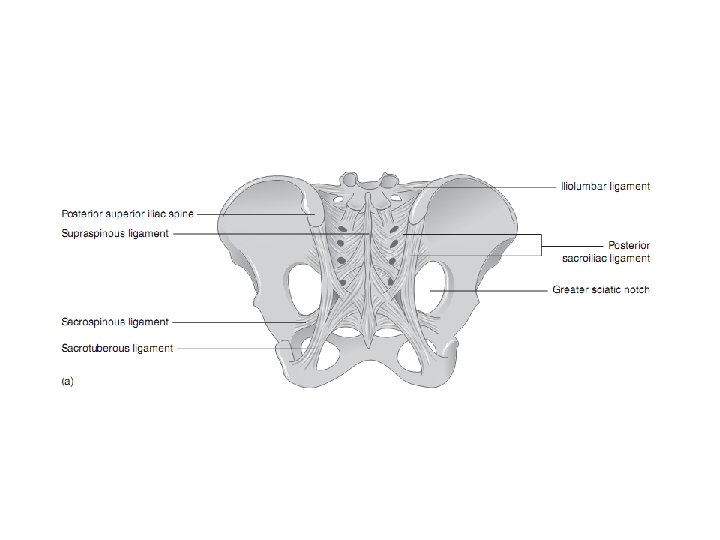
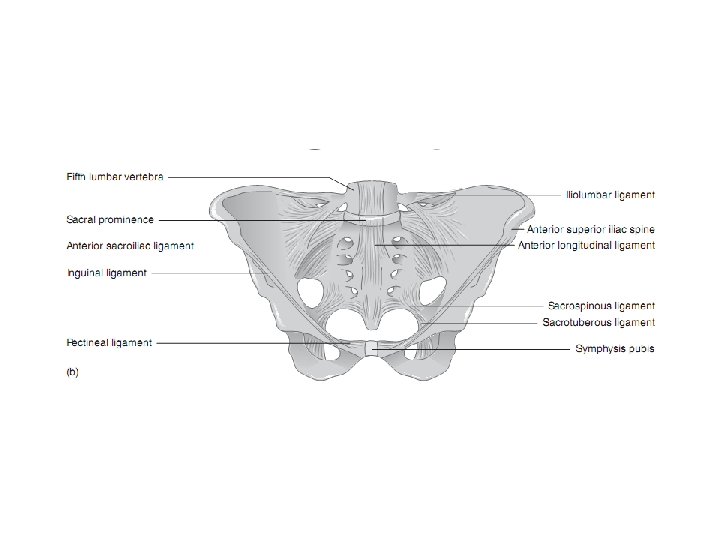
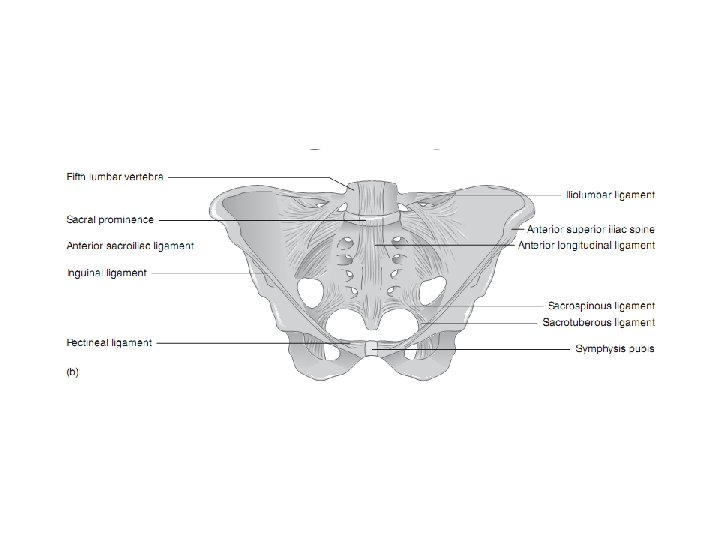
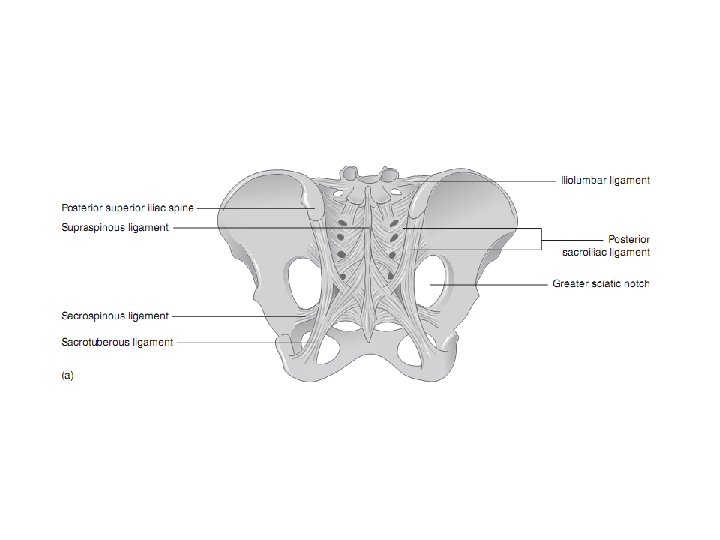
sacrum • The wedge-shaped sacrum is virtually suspended between the innominate by the exceptionally tough interosseous and posterior sacroiliac ligaments, • However, the ventral sacroiliac ligament is less substantial and is thought to tear during childbirth
• The upper sacrum is stabilized by the iliolumbar ligaments via its attachment to the fourth and fifth lumbar vertebra and the • Lower sacrum by the sacrospinous and sacrotuberous ligaments attachments to the posterior iliac spines and ischial tuberosities
Loading during pregnancy • Loading of the sacral prominence (e. g. in pregnancy) is often, but not invariably, accompanied by lumbar lordosis and its associated adaptations: 1. hip and knee flexion, 2. thoracic kyphosis and 3. cervical extension with a 4. forward-thrusting chin. • It should be noted that in this case it is the sacrum that moves on the ilia and that the pelvis as a whole does not tilt forward to produce the lumbar lordosis. The pelvic tilt may well remain constant. Sacrum Rotate down and forward.
Lumbar lordosis Sacrum rotation down and forward Anterior pelvic tilt
• The range of movement at the two sacroiliac joints and the symphysis pubis is normally small; however, movement at one joint can affect the other two joints in a variety of ways. • During pregnancy, the elevated levels of 1. oestrogen, 2. progesterone and 3. relaxin play a major role in increasing the laxity of the pelvic girdle joints. The hormonal levels do return to normal in the weeks following childbirth, but the time taken will also be affected by breastfeeding. • By 3 to 6 months postnatal, the pelvic girdle should return to its prepregnant state; it may need external stabilization during this period