Anatomy of female pelvic organs Presented by Dr

Anatomy of female pelvic organs Presented by : Dr. Sonu Lecturer

Female pelvic organs � Divided into--- External genitalia Internal genitalia

�Includes- External genitalia Mons pubis/veneris Labia majora Labia minora Clitoris Vestibule Perineum �Some gynecologists regard the perineum as part of vulva and many include under this term the perineal body (central tendon of perineum) as well as the overlying skin. �To Anatomist s , perineum means all structures within the bony outlet of the pelvis.


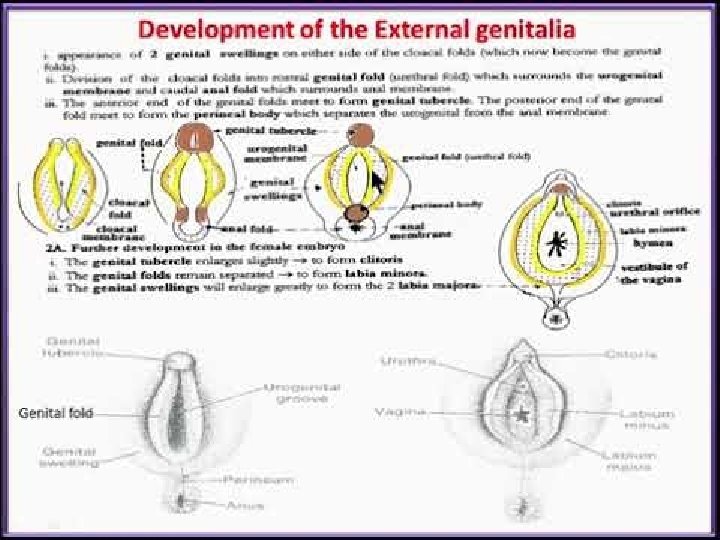
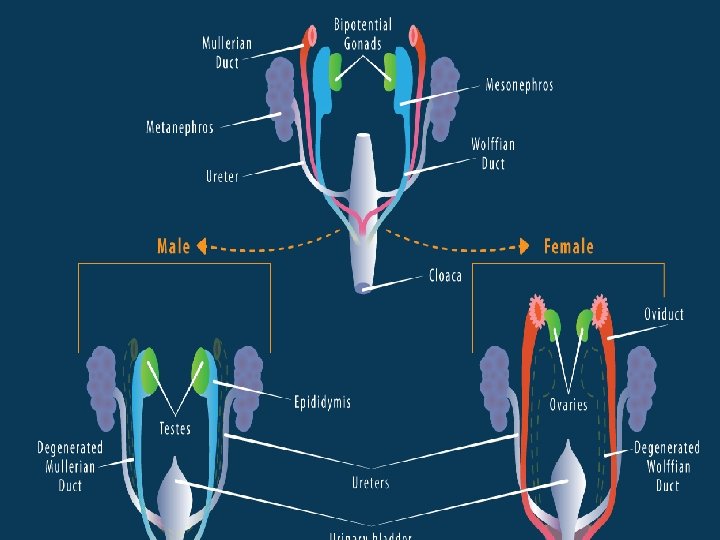
Development of Ext. Genitalia �Cloaca- the most caudal part of the hindgut. �Cloacal membrane seperates the cloaca from the proctodaeum or anal pit. �Cloaca – subdivision into broad ventral part Narrow dorsal part �These two parts –separated from each other by the formation of urorectal septum. �Later on ventral part forms- primitive urogenital sinus- form urogenital system. �Dorsal part- primitive rectum. �Urorectal septum grows towards the cloacal membrane and divides it also in ventral urogenital membrane and dorsal anal membrane.

Cont. �Urogenital system- derived from intermediate mesoderm and primitive urogenital sinus of cloaca. �P. U. S. divides-cranial vesicourethral canal and caudal definitive Urogenital sinus. �Definitive urogenital sinus- divides into cranial pelvic part and caudal phallic part. �Urogenital membrane becomes elongated in craniocaudal direction. �Mesoderm on either side soon heaped up to form two longitudinal elevations called primitive urethral folds. �Three more elevations are – genital tubercle , right and left genital swellings.

Contd. �Genital tubercle- forms clitoris. �Genital swellings- labia majora �Primitive urethral folds- labia minora. �urogenital membrane breaks down so that continuity establishes between urogenital sinus (which forms vestibule) and exterior.

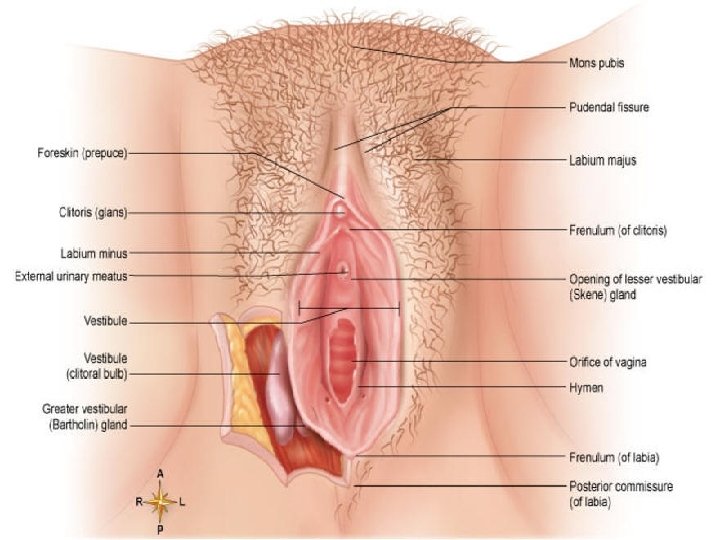
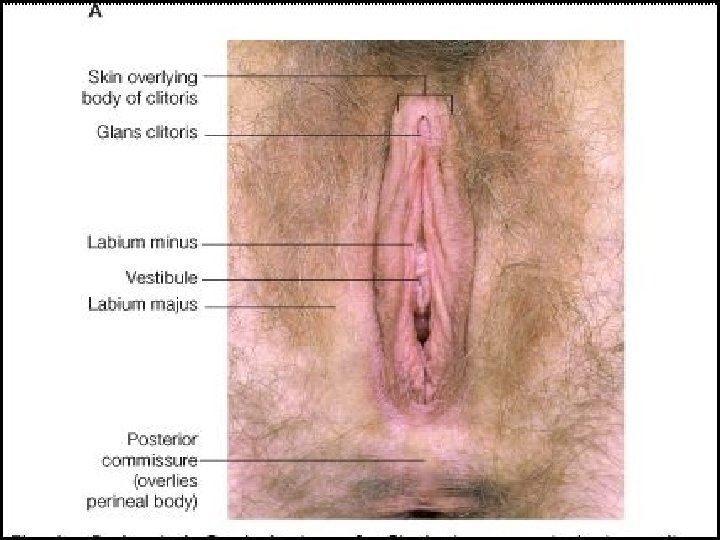
MONS PUBIS �Mons veneris/Mons venus �Mons means mountain/mound �Subcutaneous adipose connective tissue that overlies the pubic symphysis and lower abdominal muscles. �It protects the pubic symphysis �During adolescence sex hormones trigger the growth of pubic hair on the mons pubis (adrenarche) in triangular pattern. �Sexual sensation arises here. (Dawn) �Hair varies in coarseness, curliness, amount, color and thickness 13

LABIA MAJORA �Referred to as the large/outer lips (7 -9 cm long, 2. 4 cm wide, 1 -1. 5 cm thick) on each side of pudendal cleft. �formed of skin, subcutaneous adipose connective tissue. �Adipose tissue richly supplied with venous plexus-hematoma �Join medially to form posterior commissure (covers the perineal body) �Lateral boundary of vulva �Round ligaments insert at its anterior third • Protect the introitus and urethral openings • Covered with hair, sweat glands, sebaceous glands • Some of the sweat glands are large, coiled and specialised k/as apocrine glands…found in axilla, vulva and their secretion when modified by bacteria gives rise to specific odour which is of sexual significance. • Inner surface hairless • Homologus with scrotum in male (labioscrotal or genital swellings) 14

Contd. �The skin over the mons and L. majora contains hair and has a subcutaneous layer similar to that of abdominal wall. �The subcutaneous layer consists of a superficial fatty layer similar to Camper fascia and a deeper membranous layer called Colles fascia/Superficial perineal fascia (Scarpa Fascia of ant. Abdominal wall) �Clinical correlation- Colles fascia attaches firmly to the ischiopubic rami laterally and the perineal membrane posteriorly. These attachments prevent the spread of fluid, blood or infection from the superficial perineal space to the thighs or posterior perineal triangle. �Anteriorly Colles fascia has no attachments to the pubic rami and it is therefore continuous with the lower anterior abd wall, so spread of infection, fluid, blood between these compartments.

Contd. �The round ligament and the obliterated processus vaginalis also termed the canal of Nuck, exit the inguinal canal and attach to the adipose tissue or skin of the labia majora. �Thus the D/d of a mass in the l. majora should include a leiomyoma arising from the round ligament or persistent processus vaginalis. �A congenital inguinal hernia also may reach the labium majus. �Mons and l. m. are exposed to ordinary diseases of skin like psoriasis, sebaceous cysts, boils and caruncles and new growths. �

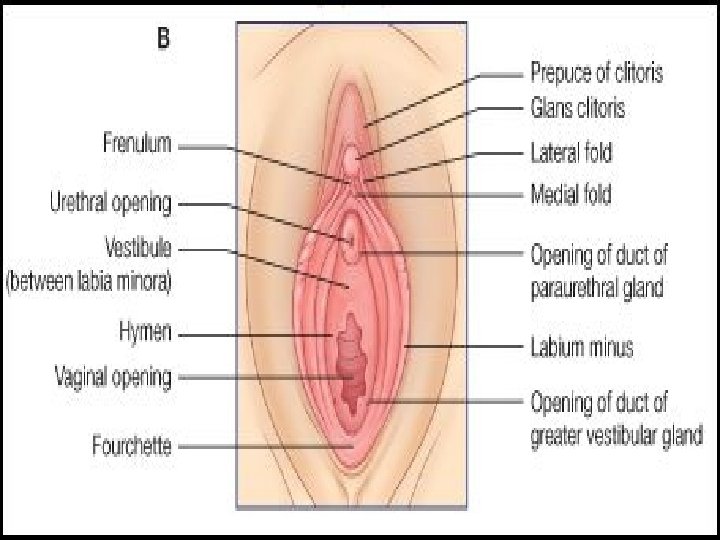
LABIA MINORA �Referred to as the “inner lips”/small lips (5 cm long and 0. 51 cm thick) �Made up of 2 thick folds of skin just within labia majora. �Ant. Divide to enclose clitoris& form prepuce, frenulum �Lower portion meets to form fourchette. �Do not contain hair follicle, sweat glands, fat. �Contain loose connective tissues (allow mobility of skin during intercourse and accounts for the ease of dissection with vulvectomy), sebaceous glands, erectile mm fibres, vessels, nr endings �Fossa navicularis the depression b/w fourchette and hymen. 18
 and can be")
Clinical correlation �Labia minora in some cases become pendulous (>5 cm) and can be drawn into the vagina during coitus. If associated with dyspareunia in this setting, the labia can be reduced surgically (V shaped wedge excision). �Chronic dermatologic diseases such as lichen sclerosus (involved anogenital skin) may lead to significant atrophy or disappearance of the l. minora. �The main hallmark of this disease is vulvar pruritus. �On physical examination, typical white atrophic papules may coalesce into porcelain white plaques and lead to labia minora regression, clitoral concealment, urethral obstruction and introital stenosis. Over time a lesion may spread to the perineum and anus form a figure 8 or hourglass shape.

CLITORIS �Highly sensitive organ composed of nerves, blood vessels, and erectile tissue. �Located under the prepuce. �It is made up of a body (2 cm), glans (0. 5 cm) , 2 crura. � 2 crura which attach it to pubic bones. �Becomes engorged with blood during sexual stimulation. �Key to sexual pleasure for most women. �Analogus to penis in the male. �Vessels of clitoris are connected with vestibular bulb �Attached to pubic symphysis by suspensory ligament. �Smegma is secreted beneath the prepuce. 21
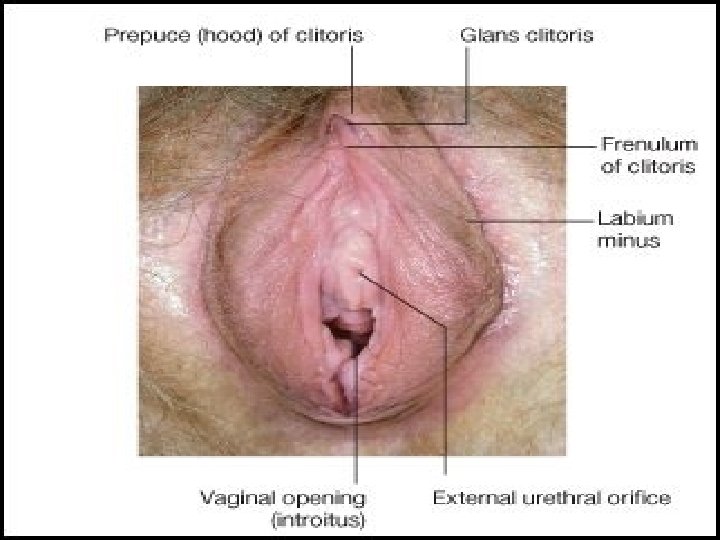
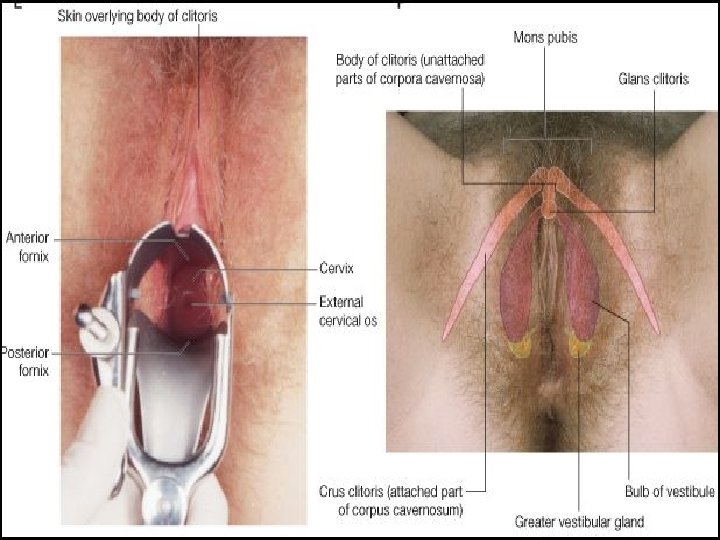

Vestibule �Meaning a forecourt or a hall next to entrance. �Bounded laterally by Hart line (demarcates changes in epithelium) and medially by hymenal ring. �Beyond Hart line the startified sqamous epithelium has a thin keratin layer. �Inside hart line, the epithelium is non keratinized. �Clinical correlation- important for choosing incision sites for Bartholin gland duct drainage or marsupialization ( inside the Hart line good) �Triangular space � 4 openings- (1) urethral opening � (2) vaginal orifice and hymen � (3) bartholin’s gland Urethral opening �Situated in midline �In front of vaginal orifice �Paraurethral ducts open here

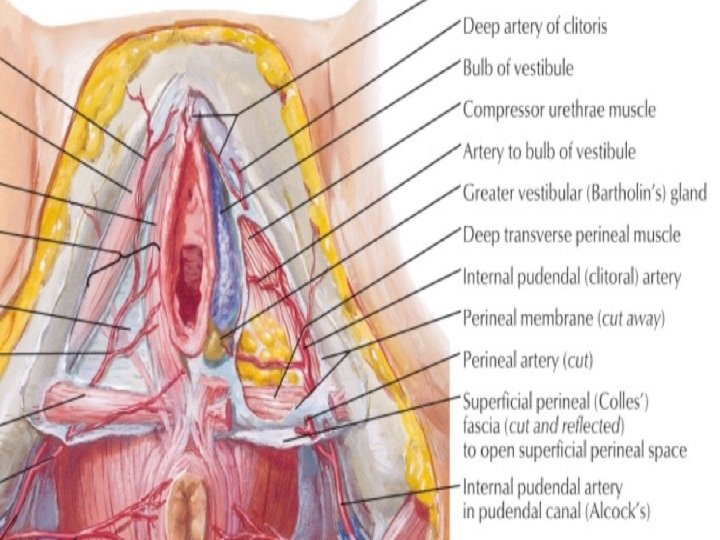
Vaginal orifice and hymen �Lies in post. end of vestibule �Incompletely closed by a septum of mucous membrane called hymen �It is one of the signs of loss of virginity. �Hymen is relatively avascular so its tearing usually causes only a slightly loss of blood. �during childbirth hymen is extremely lacerated& form carunculae myrtiformis �Bartholin’s gland/greater vestibular glands �Pea sized 0. 5 cm �Yellowish white colour �Situated in superficial perineal pouch � during sexual excitement, it secretes abundant alkaline mucus which helps in lubrication

Contd. Contraction of bulbocavernous helps to squeeze the secretion. �Lined by columnar epithelium �Duct 2 cm & opens into the vestibule at 5 and 7 o clock position. v Bulb of the vestibule • Two elongated (3 cm long)vascular erectile masses. • Anterior ends are joined to one another and to clitoris. • Posterior ends in contact with Bartholin glands. • Their superficial surfaces partially covered with Bulbocavernosus muscles. • Deep surfaces in contact with perineal membrane. • Becomes engorged with blood during sexual arousal, narrowing the vaginal orifice & placing pressure on the penis during intercourse.

Clinical correlation �The proximity of the Bartholin glands to the vestibular bulb accouts for the significant bleeding sometimes encountered with Bartholin gland excision.

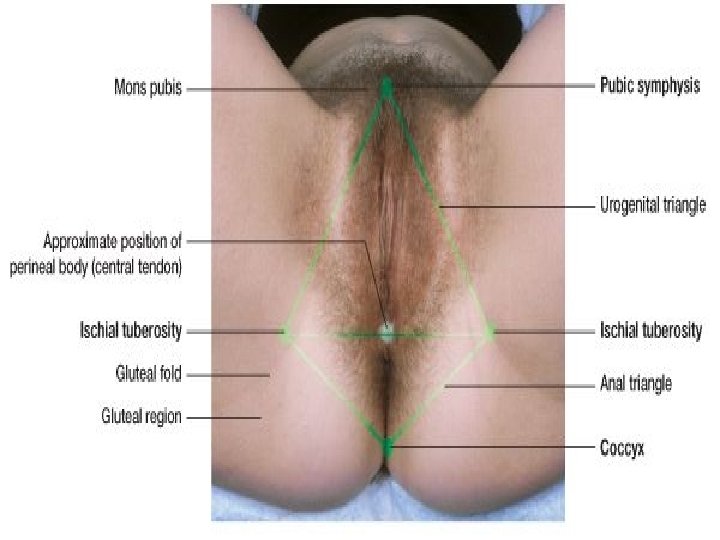
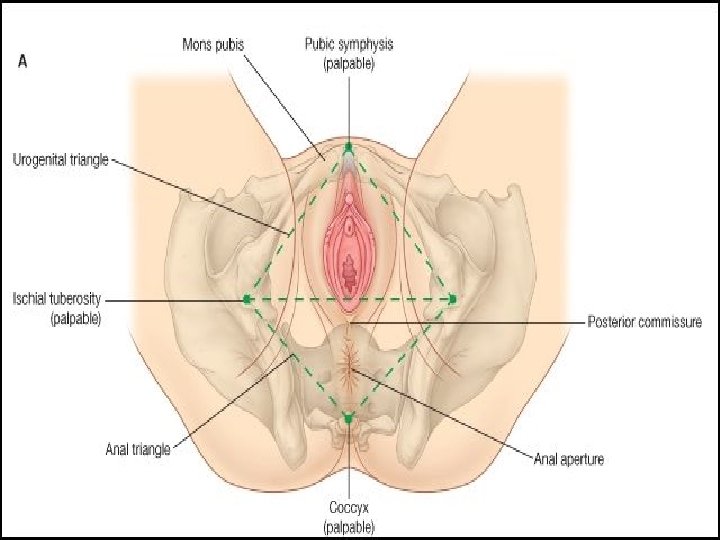
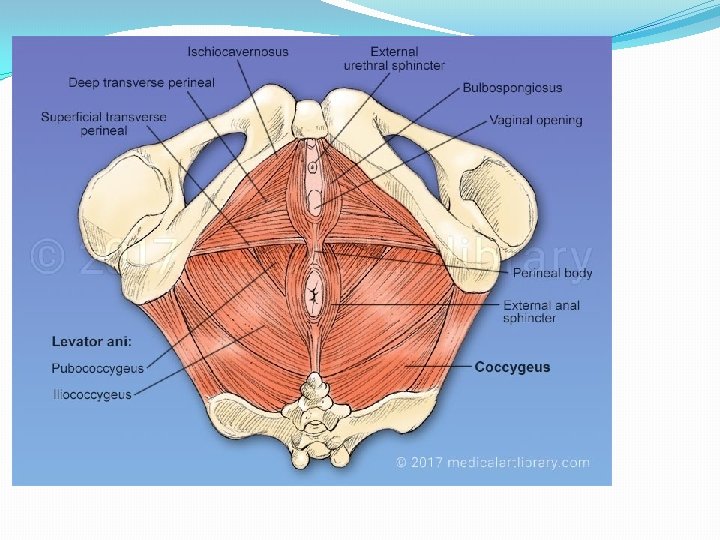
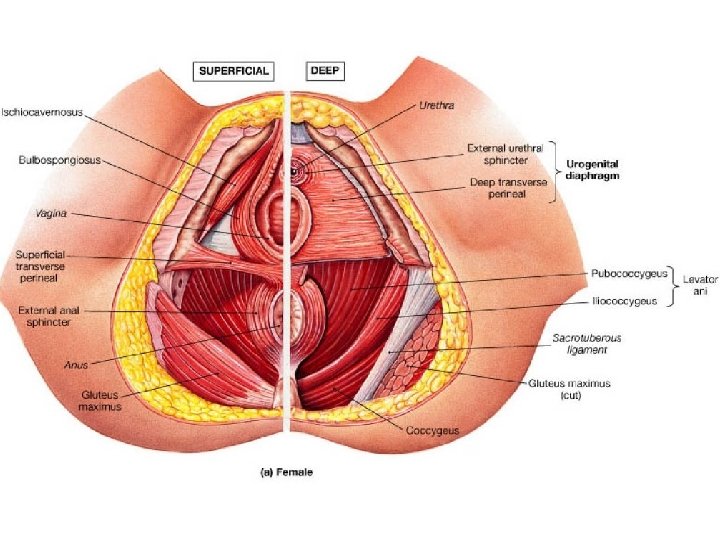
PERINEUM �The muscle and tissue located between the vaginal opening and anal canal �Unlike the rest of vulva, it has very little sub-cutaneous fat so the skin is close to the underlying muscles. �It supports and surrounds the lower parts of the urinary and digestive tracts �The perineum contains an abundance of nerve endings that make it sensitive to touch. �An episiotomy is an incision of the perineum used during childbirth for widening the vaginal opening �Diamond shaped area that includes urogenital triangle & anal triangle. �Boundaries same as that of pelvic outlet. 28

Urogenital triangle �Pierced by terminal part of vagina and urethra � 2 compartments-superficial and deep perineal pouch �S. P. P. - formed by deep layer of colles fascia and inferior layer of urogenital diaphragm(perineal membrane). �Contents- superficial transverse perinei, bulbocavernosus, ischiocavernosus and Bartholin gland. �D. P. P-formed by inferior and superior layer of urogenital diaphragm/triangular ligament. �Contents are- Deep transverse perinei, sphincter urethrae membranaceae. �Both pouches contain vessels and nerves.

Anal triangle �No obstetric importance. �Terminal part of anal canal with sphincter ani externus, anococcygeal body, ischiorectal fossa, blood vessels, nerves, lymphatics.

Obstetrical perineum �The interval between post. Commissure and anus constitutes the perineum (4 cm*4 cm) �Also called perineal body, central point of perineum. �Contains fascia- camper, colles, urogenital diaphragm layers. �Muscles- superficial and deep transverse perinei, bulbosongiosus, levator ani, sphincter ani externus. �Importance�Helps to support the levator ani �Support the post. Vaginal wall. �Vulnerable to injury during childbirth �Episiotomy.


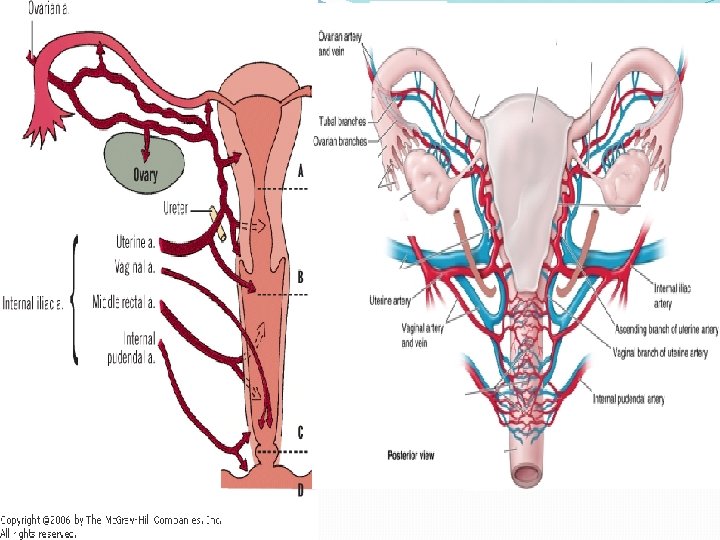
Blood supply of Vulva Arteries Veins �Internal pudendal artery branches- Labial, transverse perineal, vestibular bulb, deep and dorsal branches of clitoris. �Femoral artery- superficial and deep pudendal. �Internal pudendal vein �Vesical or vaginal venous plexus �Long saphenous vein
")
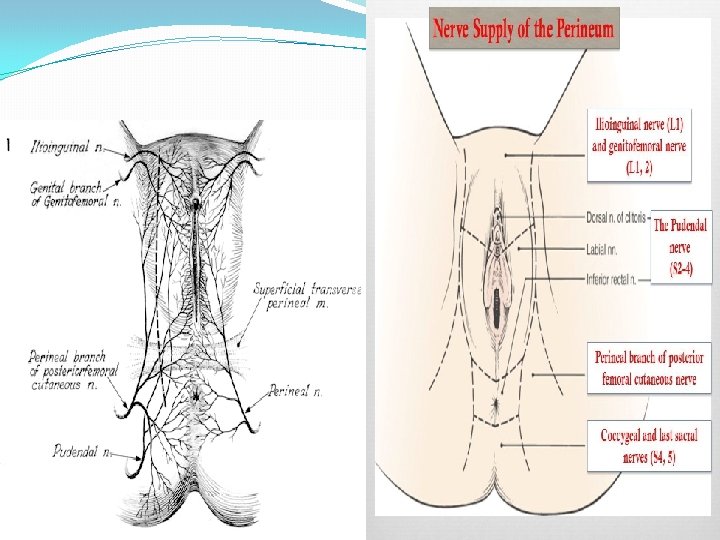
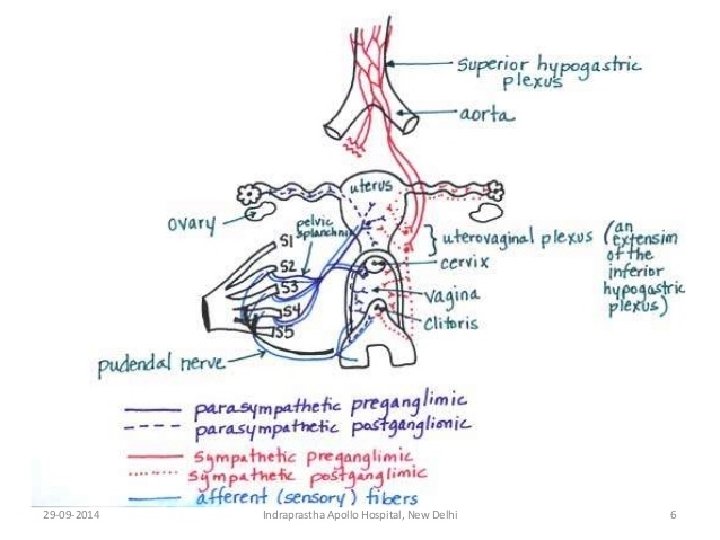
Nerve supply of Vulva �Anterosuperior part-Ilioinguinal and genitofemoral nerve (L 1 and L 2) �Posteroinferior part- Post. Cutaneous nerve of thigh (S 234) �In b/w- pudendal nerve- labial and perineal branches (S 234)
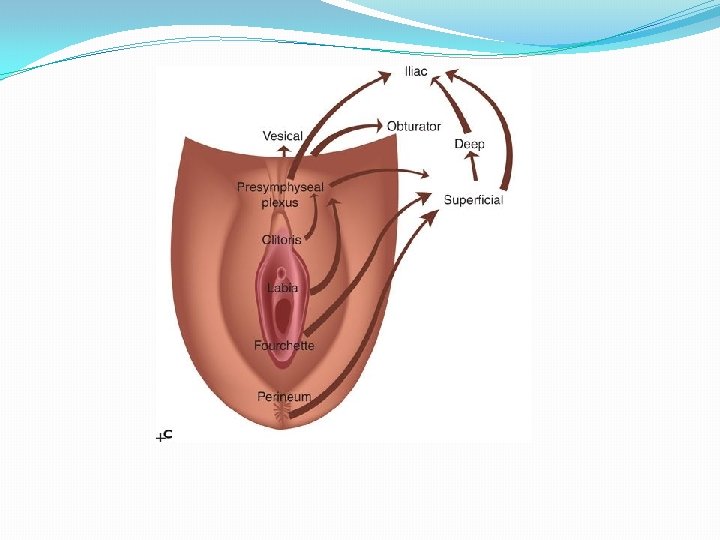

Lymphatics of vulva �Dense lymphatic plexus in the dermis of vulva �Ipsilateral free communication and also contralateral �Hardly cross beyond labiocrural fold �Also anastomose with lower third of vagina lym. �Superficial inguinal lymph nodes are the primary sentinel nodes of vulva. �Deep inguinal lymph nodes are secondarily involved. �It is unusual to find positive pelvic glands without metastatic disease in the inguinal nodes. �Pattern- Lym. Of vulva- S. I. L. N. - D. I. L. N. -P. N. �Responsible for spread of vulvar carcinoma. �Incidence of lymph node involvement directly related to site, size of lesion and depth of stromal invasion. �Regional lymph nodes are assessed clinically and By MRI, USG, PET, sentinal node lymphoscintigraphy using technetium 99.

Applied part �Secondary sexual characters- Pubic hair growth �Vulval defence �Round ligament fibroid �Bartholin cyst/abscess-marsupilisation �Clitoromegaly �Congenital anomalies-cryptomenorrhoea �Episiotomy �Clitoris may be absent, may be bifid or may be double. It may be enlarged in hermaphroditism (adrenogenital syndrome/CAH) �Labia minora may show partial fusion. �Urethra may open on the anterior wall of vagina, this is the female equivalent of male hypospadias.

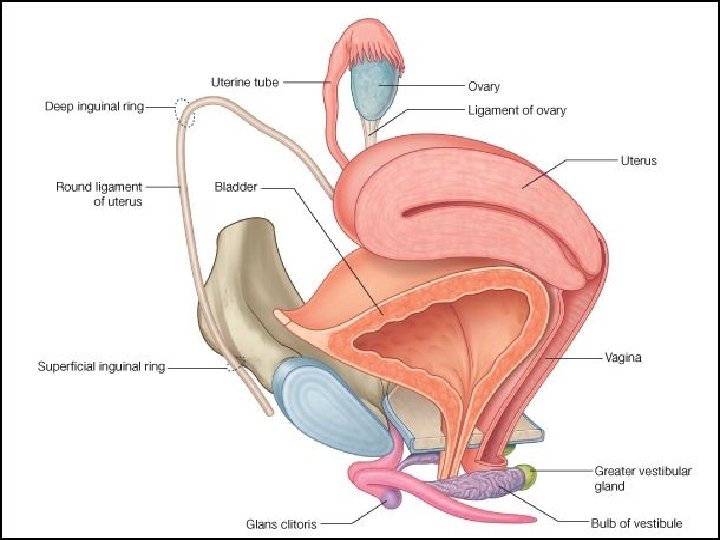
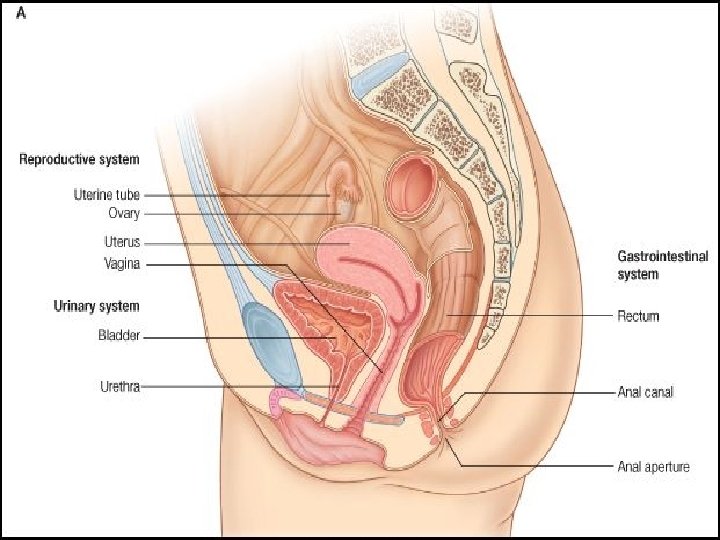
INTERNAL GENITALIA �The internal genitalia consists of the: Ø Vagina �Cervix �Uterus �Fallopian Tubes �Ovaries 43


Avartha of Yoni �Yoni is that organ whose structure is compared with Shankha Nabhi i. e. Narrow below and broad above and also this structure is placed in such a manner i. e. it is seen like Concentric Circle that is called as Avartha. �These three Avartha of Yoni should be � 1. First Avartha should be Vagina: - It Starts from Vestibule to External Os. � 2. Second Avartha should be Cervix: - It starts from External Os to Internal Os. � 3. Third Avartha should be Uterus: - It starts from Inernal Os to Fundus of Uterus (Alpa. Muka and Anta Sushria) �Avarta also means rugae as told by Acharya Ghanekar.

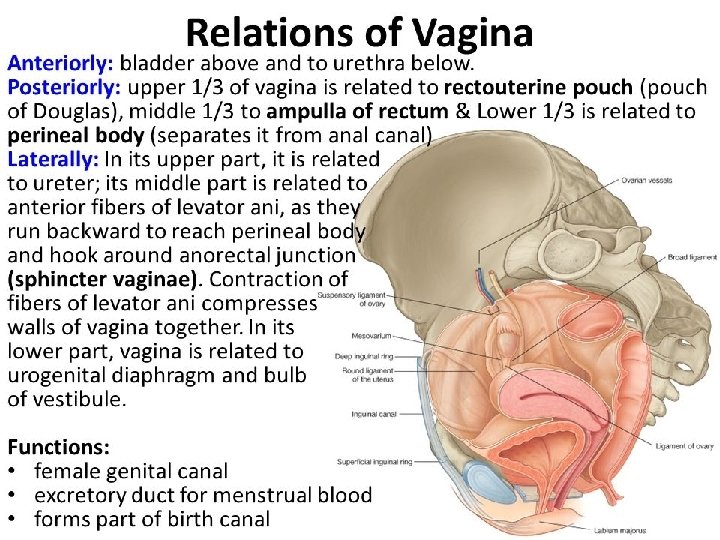
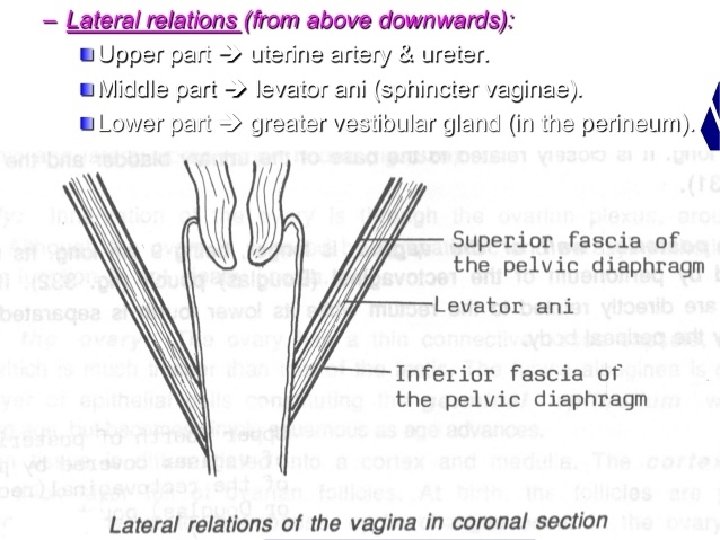
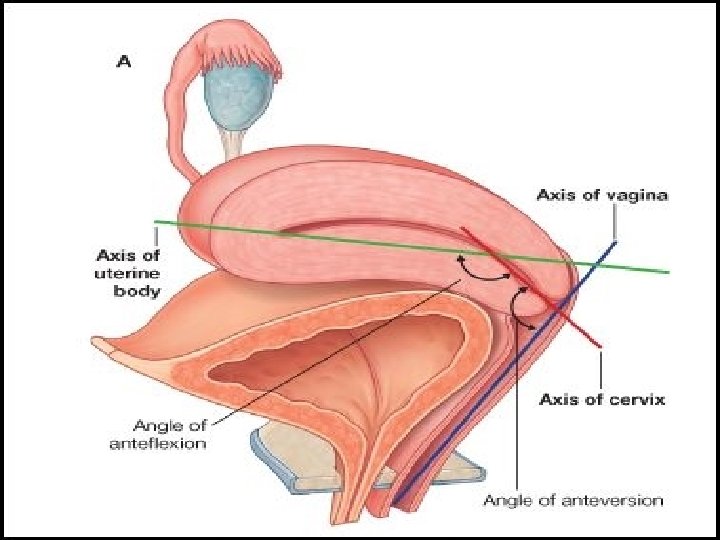
VAGINA �Means sheath, fibromusculomembranous sheath. �Hollow viscus, Communicating the uterine cavity with exterior at vulva. �Excretory channel �Organ of copulation �Forms the birth canal �Forming an angle of 45* with the horizontal �Long axis of vagina parallel to the plane of inlet �Canal diameter-2. 5 cm, distensibility power due to rugae.
 anterior : 7 cm � (ii) posterior: 9")
Contd. v. Walls- 4 � (i) anterior : 7 cm � (ii) posterior: 9 cm � (iii) 2 lateral walls v. Fornices- 4 � (i) anterior: shallow one � (ii) posterior: deeper one � (iii) 2 lateral v. Histology of vagina� (i) Mucosa-stratified sq. epi. , rugae � (ii) Submucosa-loose areolar vascular tissues � (iii)Muscular layer-inner circular and outer long � (iv) Serosa –tough and highly vascular
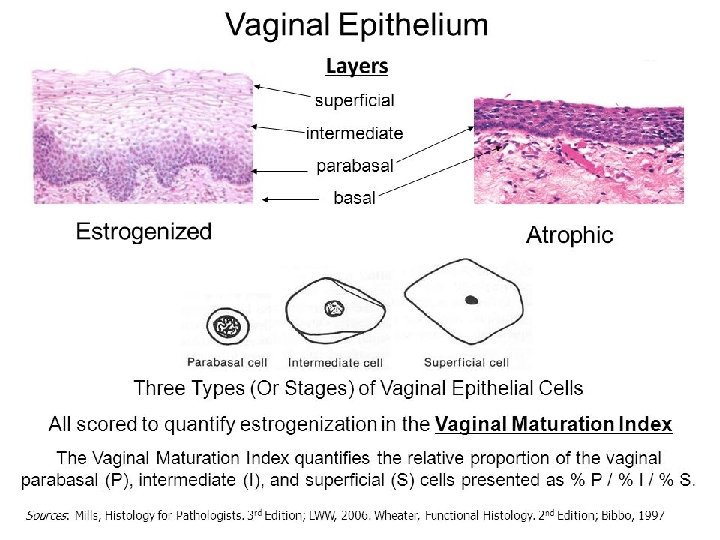
 para Basal cells/Basal cells (2) Intermediate")
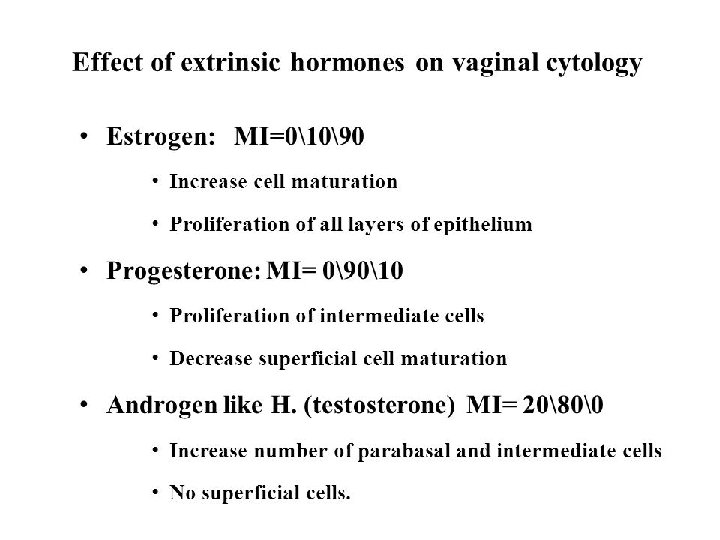
Contd. � 3 distinct layers are defined: (1) para Basal cells/Basal cells (2) Intermediate cells (3) Superficial cells contain glycogen under estrogen influence lactic acid �Glycogen {Doderlein’s bacilli} maintain vaginal p. H [4 - 5. 5]

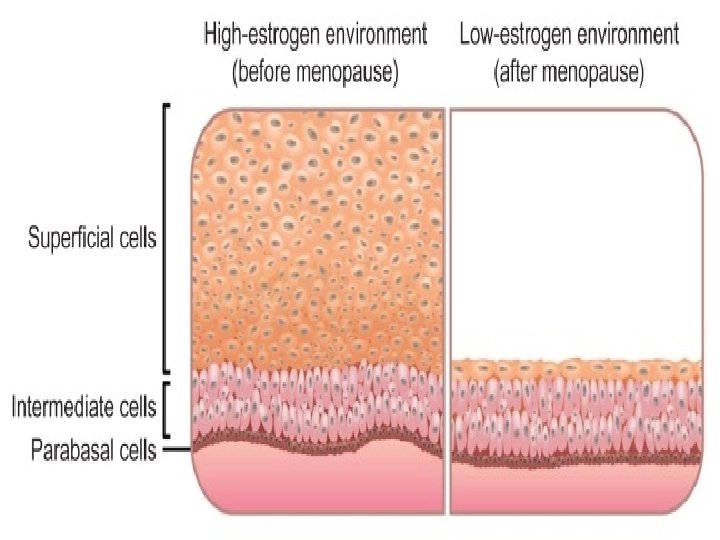
Contd. �Birthto 2 wks: maternal estrogen present, thick sq epithelium � 2 wks to prepuberty: no estrogen , thin epithelium �Puberty: estrogen appears , thick epithelium �Reproductive period: estrogen present, �Post menopause: again estrogen amount decreased, atrophy

Contd. �Secretion: � very small � little excess in mid menstrual , just prior to menses, during pregnancy, during sexual excitement. �Derived from: cervical glands endometrial glands transudate of vaginal epithelium Bartholin’s glands �Note- dendritic cells in its mucosa are antigen presenting cells, so unfortunately they participate in transmission of viruses for e. g. HIV
 Fibro-muscular (Garbhachidrasamshrita 3 peshi; three muscles of myometrium) organ")
UTERUS �Hollow Pyriform (pear shaped) Fibro-muscular (Garbhachidrasamshrita 3 peshi; three muscles of myometrium) organ (kshetra). �Situated in pelvis �In b/w bladder & rectum �Measures about 7. 5 cm long, 5 cm wide, 2. 5 cm thick (during pregnancy 35 cm) �Wt - 50 -80 gm �Shape, wt, and dimensions vary a/c to parity and estrogen stimulation. �Capacity-5 -10 ml �Position-AVAF normal �In 15 -20%, RVRF position
 body/corpus (muscular)- fundus � Fundus � body proper � cornua of")
Contd. �Parts: (1) body/corpus (muscular)- fundus � Fundus � body proper � cornua of uterus �(2) isthmus- importance �(3) cervix- fibrous

Uterine cavity �Total length- 6 -7 cm �Cavity/body- triangular-3. 5 cm �No cavity in fundus �Cavity/cervix- fusiform-2. 5 cm
- body: cervix=5:")
Changes of uterus with age and parity �In intrauterine life (28 wk)- body: cervix=5: 1 �At birth- cervix much longer> body =2: 1 �Childhood (before menarche)- cervix: body= 1: 1 �Puberty- body: cervix=2: 1 (estrogens) �Childbirth- body: cervix=3: 1 �After menopause- body: cervix=1: 1 (atrophy, less muscular more fibrous)

Contd. v. Fundus: �Lies above the openings of the uterine tubes �No cavity v. Body proper: �Triangular �Lies b/w uterine tubes & isthmus v. Cornua: �Uterine tube, round lig. , lig. of ovary attached here

contd. �Cervix: �Extends from histological int. os to ext. os. �Cylindrical shape, � 2. 5 cm length and diameter � 2 parts (1) supravaginal part-1. 25 cm �(2) vaginal part-1. 25 cm �In nulliparous- conical cervix � circular ext os �In multiparous- cylindrical cervix � ext os having slits
 perimetrium b) myometrium c) endometrium")
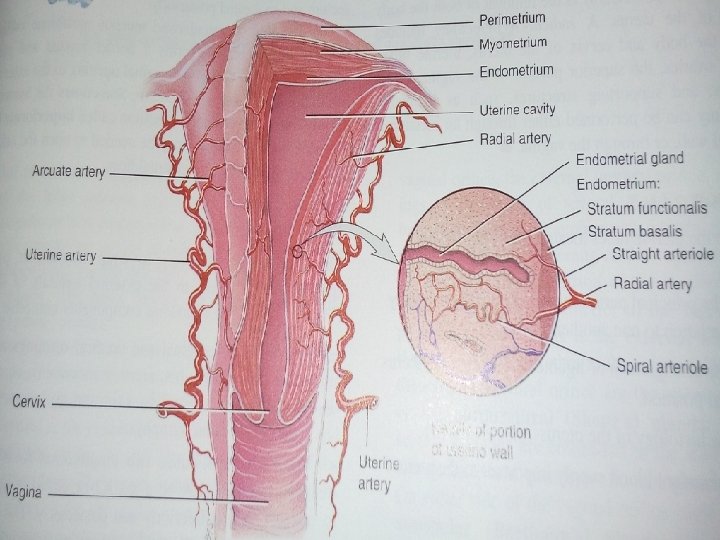
Uterus �Strutures�Body� 3 layers– a) perimetrium b) myometrium c) endometrium

Endometrium �Mucous lining of the cavity, no submucosa �Thickness varies: 1 -10 mm a/c to phase of menstrual cycle. �Basal zone and functional zone. �Consists of lamina propria & surface epithelium �surface epithelium- single layered ciliated Columnar epithelium �LP contains stromal cells, endometrial glands (tubular or spiral), vessels, nerves �Glands lined by non ciliated but secretory columnar epithelium �Changed to decidua during pregnancy
 �Post. Wall as low")
Perimetrium/Peritoneum �Present on�Whole fundus �Anterior wall upto isthmus (not cervix) �Post. Wall as low as the attachment of vagina to the cervix �It is intimately connected with the underlying muscle that it cannot be stripped away. �Absent on�Sides of uterus b/w the attachment of 2 leaves of broad ligament. �Lower ant. Uterine wall �Whole cervix except posteriorly

Myometrium �During pregnancy 3 layers�Outer longitudinal- continuity with outer muscles of tube and vagina. �Middle interlacing/oblique- main mass- smooth/involuntary muscle-crisscross fashion �Inner circular Ø Fibrous and elastic tissues are mixed with muscle in varying amounts. Ø Repeated childbearing and advancing years –fibrous tissue increase and increased risk of spont. rupture of uterus during labor.

Cervix �Composed mainly of fibrous connective tissues �Smooth mm fibres 10 -15% �Endocervix: � Arbor vitae uteri-the mucosa lining the canal thrown into folds which consist of ant. And post. Columns from which radiate circumferential folds to give apperance of tree trunk and branches. � columnar epithelium � basal/reserve cells underneath the columnar epi (these cells may undergo sq. metaplasia or may replace the superficial cells) � glands complex racemose type-secretary columar epi. �No stroma �Ectocervix/Portio vaginalis: � stratified sq. epithelium � this epithelium extends upto ext. os where there is abrupt change to columnar type.

Contd. �Transformation zone: � 1 -10 mm width �Not static but changes with hormone level of estrogen, infection, trauma �More chance of severe dysplasia, carcinoma in situ, invasive carcinoma �Secretion: � endometrial secretion- scanty &watery �Cervical secretion changes with cycle and pregnancy. �Cervical glands- secrete alkaline mucus 7. 8 p. H �Mucus plug-functionally closes the cervical canal and bacteriolytic property.

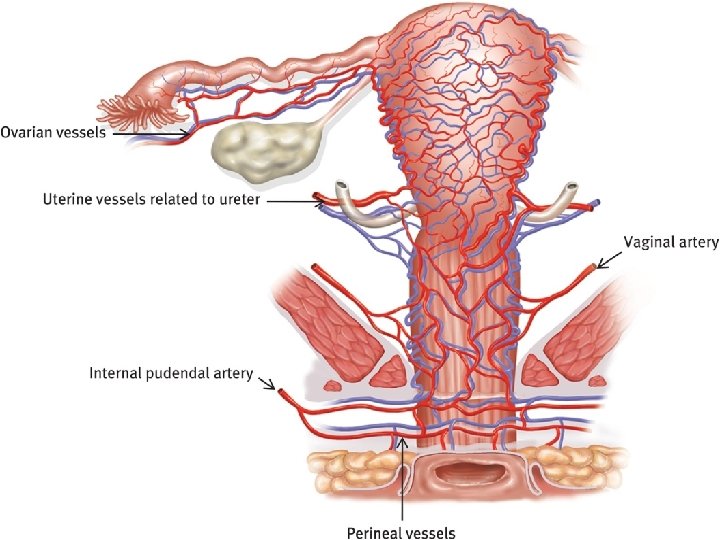
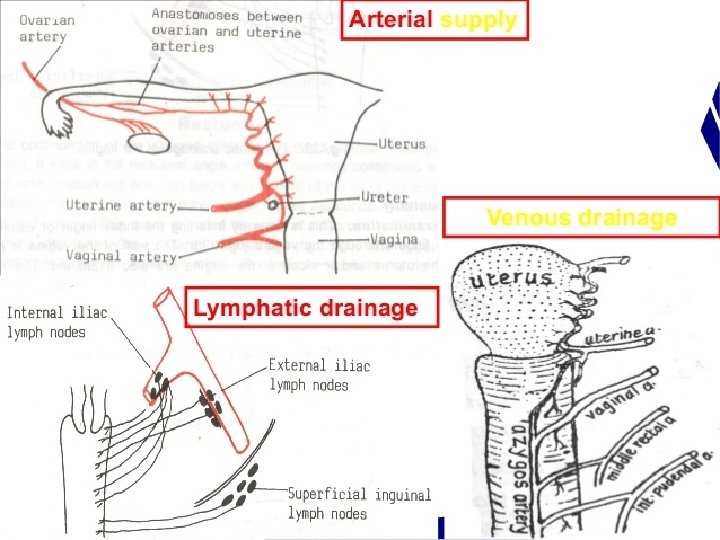
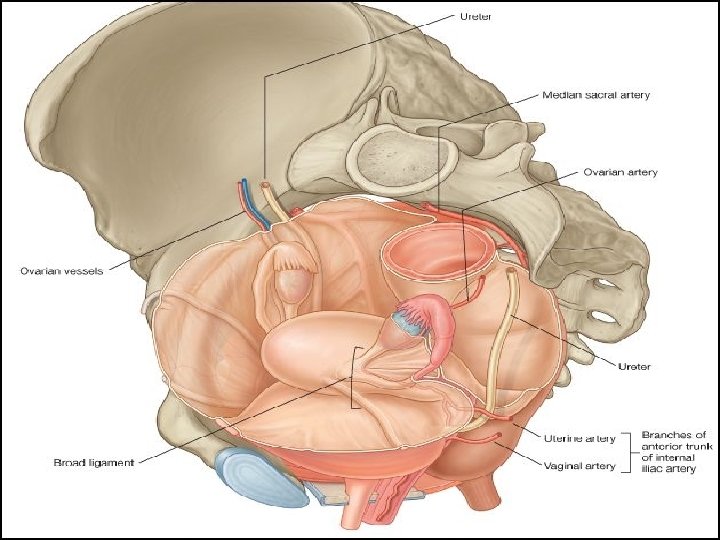
Contd. �Mucus is rich in fructose, glycoprotein, mucopolysaccharides, Na. Cl �Position: � anteversion&anteflexion �Uterus usually inclines to the right(dextrorotation) �Cervix is directed to left(levorotation) �In about 15 -20%uterus remains in retroverted position � Blood supply: � uterine artery (paired)- branch of int. iliac artery arcuate arteries

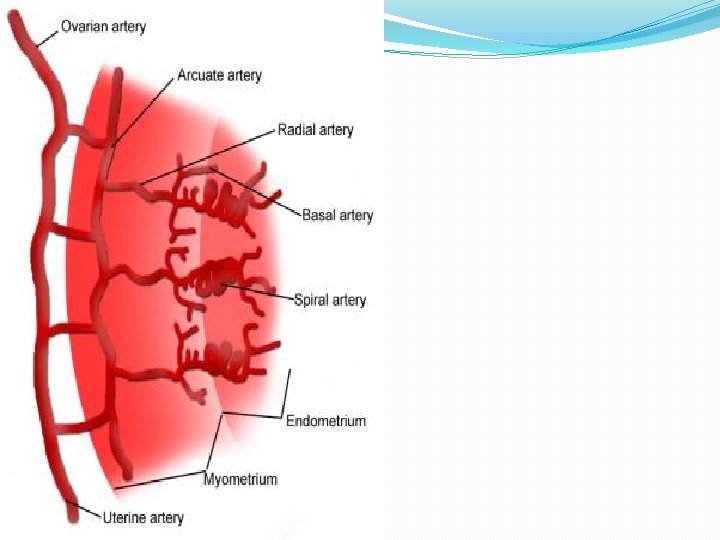
Contd. �Arcuate arteries arranged in a circular fashion in myometrium � � radial arteries(deep penetrate in myometrium) Straight arterioles spiral arteries � supply stratum basalis supply stratum functionalis in endometrium �Veins: - uterine veins drain into int. iliac veins

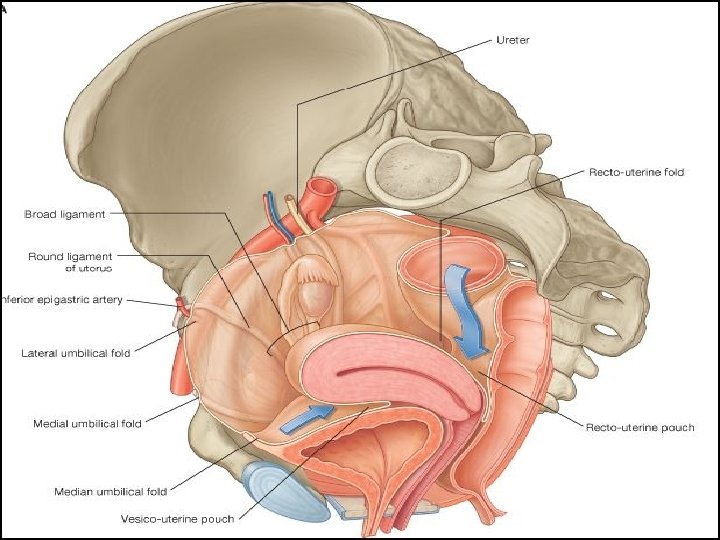
Relations �Ant. - Above the internal os- uterovesical pouch Below the internal os- separated from base of bladder by loose areolar tissue. Post. - POD Laterally- Broad ligament- in which uterine artery ascends Mackenrodt’s ligament- extends from internal os, supravaginal cervix, lateral vaginal wall. About 1. 5 -2 cm away at the level of internal os, a little nearer to left side is the crossing of uterine artery and ureter (bridge over water).

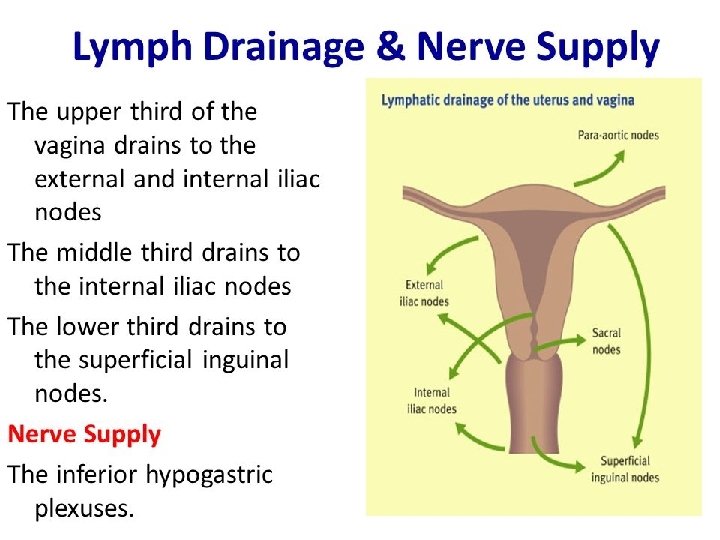
Lymphatics of Corpus �Extrinsic drainage� 1. from fundus and adjoining part of body------Para aortic lymph nodes � 2. From cornua----superficial inguinal � 3. rest of body---external iliac group � 4. adjacent to cervix----cervical lymphatics �Intrinsic plexus� 2 plexuses— 1. Basal layer/endometrium � 2. subserosal layer �The lymphatics from basal layer run through myometrium in close relation to blood vessels to reach subserosal plexus.
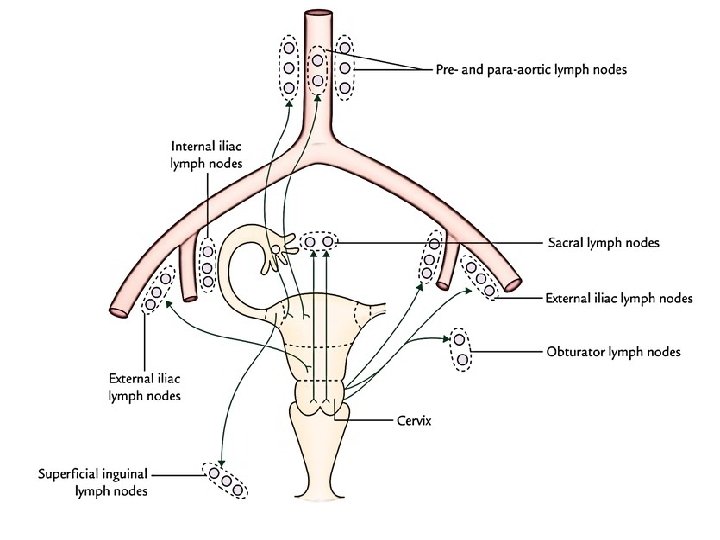

Lymphatics of cervix �Primary group� 1. sacral nodes � 2. external iliac � 3. internal iliac � 4. obturator � 5. parametrial �Secondary Group- the lymphatics from all primary groups drain into common iliac and superior lumbar group.

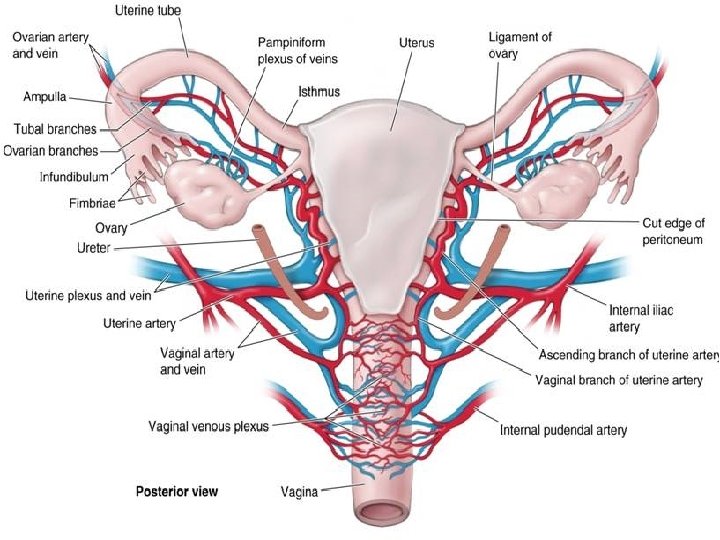
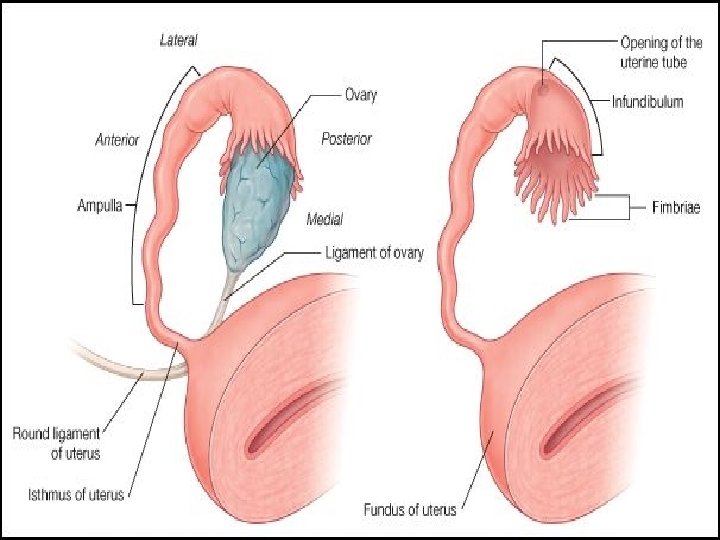
Fallopian tube � 10 cm long, Oviducts and ovary constitute adnexa. � 2 openings Uterine (1 mm) � 4 parts Pelvic opening (2 mm) Isthmus (2. 5 cm) Infundibulum (1. 25 cm) Ampulla (5 cm) Interstitial(1. 25)

Fallopian tube �Lies in upper free border of broad ligament. �It connects the peritoneal cavity to the uterine cavity. � 1. Infundibulum- bell shaped outer end surrounded by fimbriae, Abdominal ostium- 2 mm diameter. �It is devoid of broad ligament and can move freely to cover the ovary and catch the ovum. � 2. Ampulla- longest, widest tortous part, 6 mm diameter, fertilisation occurs here. � 3. Isthmus- straight part � 4. Interstitial/ Intramural- traverses the wall of uterus, devoid of peritoneum and longitudinal muscle fibres, uterine opening 1 mm diameter.
 serosa- cover whole tube except mesosalpinx")
Contd. �Histology of fallopian tube� 3 layers: (i) serosa- cover whole tube except mesosalpinx attachment and intramural part. � (ii) muscular-outer long. and inner circular, thickest at isthmus-acts as sphincter and thin in ampulla, peristalsis of f. tube is due to muscular layer. � (iii) endosalpinx(mucosa)- lined by columnar epithelium � partly ciliated secretory non ciliated � Peg cells v No submucous layer nor any glands. v Functions: - (1) transport of gametes (2)facilitate fertilisation (3)survival of zygote through its secretion. �Peristalsis and production of secretions from the endosalpinx are under the influence of ovarian hormones, undergo cyclical changes.

Contd. �Blood supply�Artery-uterine Vein-ovarian veins ovarian �Nerve supply- uterine & ovarian nerves. v. Note- Tube is very much sensitive to handling.
, wt 5 -10")
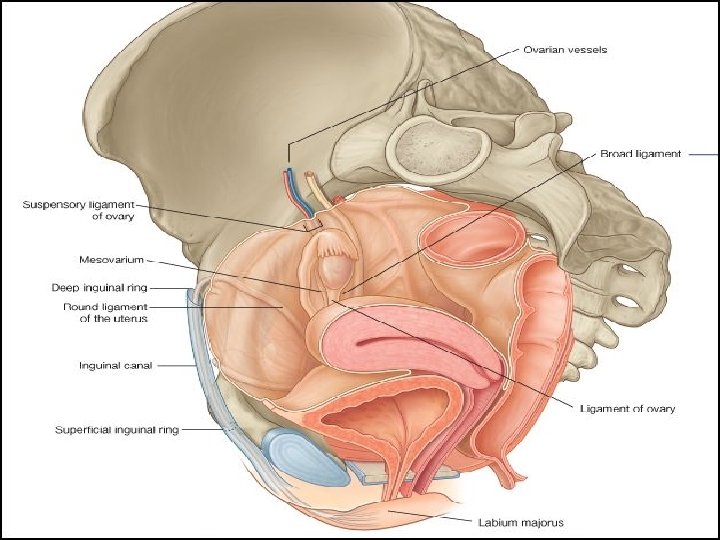
OVARY �Egg receptacles �Female gonads or paired sex glands (3*2*1 cm), wt 5 -10 gms average 7 gm �Intraperitoneal gland without peritoneal covering. �Shape& size- unshelled almonds �Homologus to testes �Concerned with- (i) production of gametes (ii)hormones- estrogen, progestrone, relaxin, inhibin v Note- ovary descend to the brim of superior portion of the pelvic cavity during 3 rd month of development. v contains a Hilum, the point of entrance & exit for blood vessels, nerves.

Contd. �Position- in nulliparous: vertical � in multiparous: horizontal �External features- before onset of ovulation: smooth surface � after puberty: puckered surface � 2 ends/poles- upper/tubal pole � lower/uterine pole � 2 borders- Ant. /mesovarian border � Post. /free border � 2 surfaces- medial & lateral
 mesovarium (ii)ovarian ligament (iii)infundibulopelvic/suspensory ligament � �Histology")
Contd. �Ligaments which hold them in position(i) mesovarium (ii)ovarian ligament (iii)infundibulopelvic/suspensory ligament � �Histology of ovary�(1)Germinal epithelium- covers the surface of ovary except at hilum. �Note- it is a misnomer bcz it does not give rise to ova. The progenitors of ova arise from the yolk sac and migrate to the ovaries during embryonic development. �(2)Tunica albuginea �(3)Cortex- contains primordial follicles, maturing follicles, Graafian follicles, corpus luteum, corpus albicans
Medulla- loose connective tissue, vessels, nerves, few unstriped muscles � Blood supply- ovarian")
Contd. �(4)Medulla- loose connective tissue, vessels, nerves, few unstriped muscles � Blood supply- ovarian artey � ovarian vein �Nerve supply- sympathetic supply from T 10 segment.

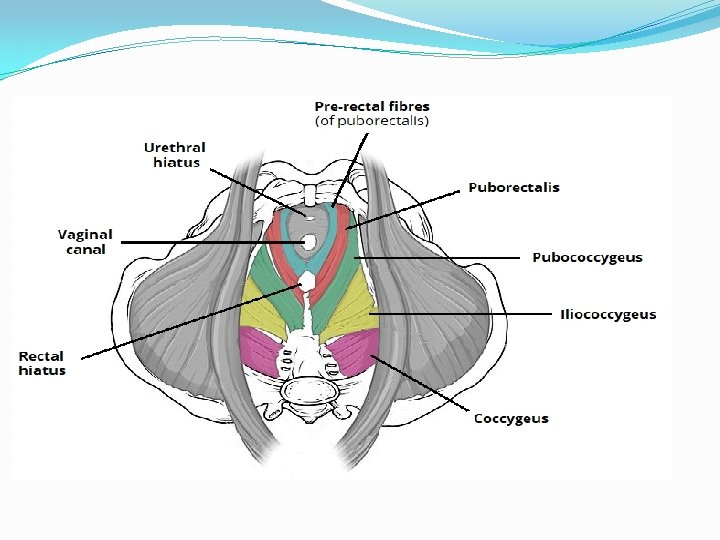
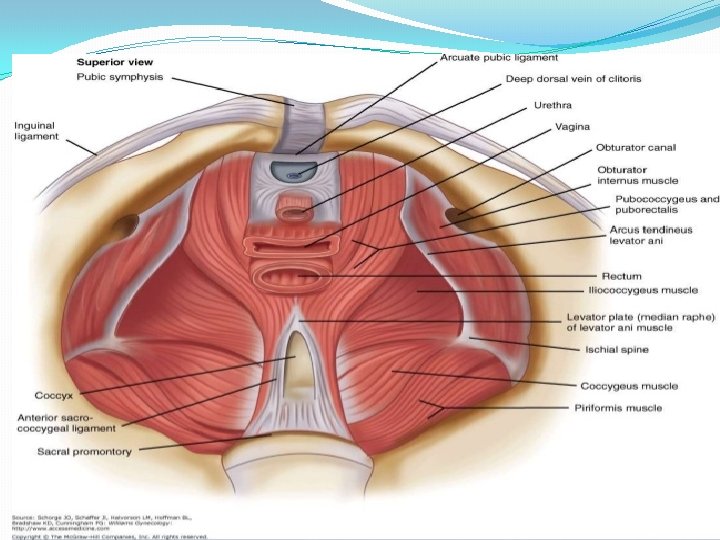
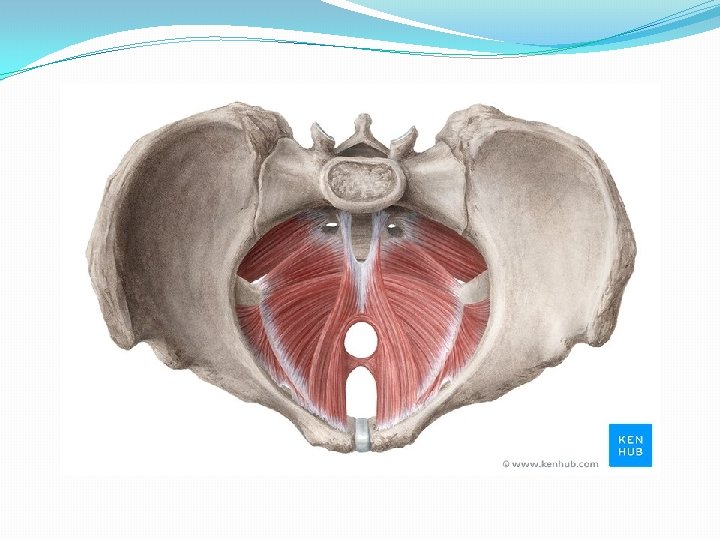
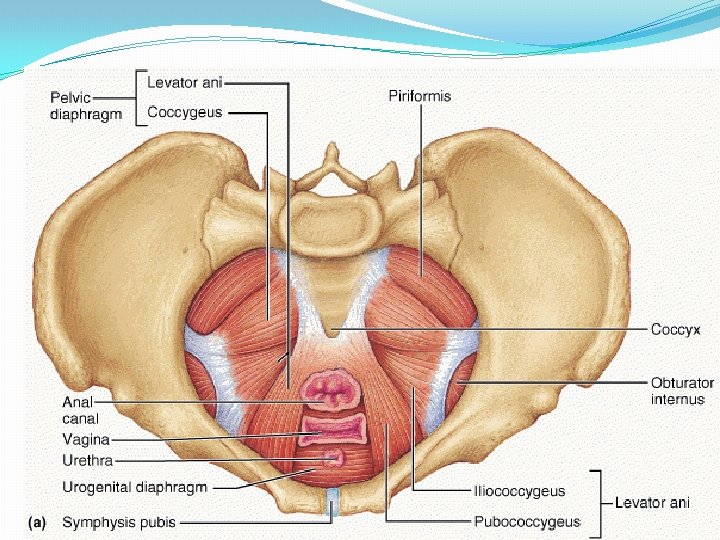
Pelvic floor/ Pelvic Diaphragm �Consists of all tissues lying in b/w pelvic cavity and surface of vulva and perineum. �Includes the pelvic peritoneum, extraperitoneal fat and cellular tissue, l. ani and its fascia, urogenital diaphragm, muscles of perineum, subcutaneous fascia and fat, the skin. (jeffcoate) �The muscle with its covering fascia- k/as Pelvic diaphragm. �Which muscle? ? �Levator Ani- physiologically maintain a constant state of contraction. (Williams) �Complex unit, Consists of three sets of muscles� 1. Pubococcygeus � 2. Iliococcygeus � 3. Ischiococcygeus/coccygeus �Two surfaces- Upper- concave…. covered by parietal layer of pelvic fascia (direction downwards, backwards, medially) � Inferior- Convex……. covered by anal fascia.
 � Relaxed during evacuation of")
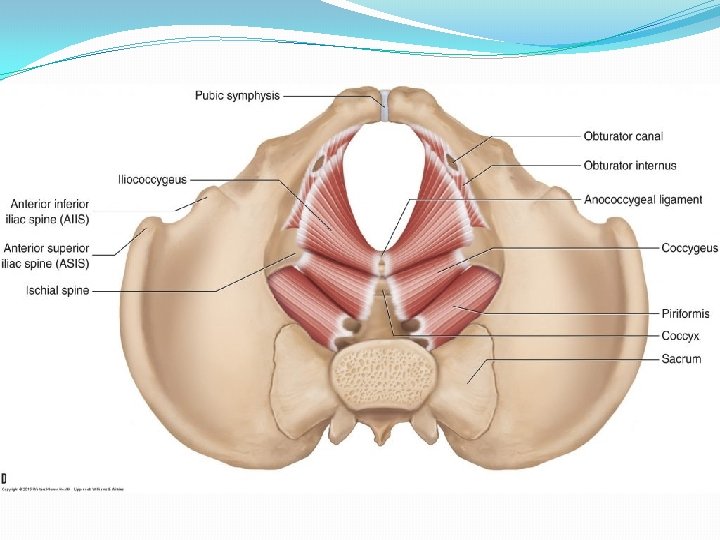
� Bilateral Strong muscle, fatigue resistant, striated muscle (voluntary) � Relaxed during evacuation of bowel and bladder (during bearing down effort) � Slug like hammock around pelvic organs. � Origin- from the back of pubic rami-pubococcygeus � from the condensed fascia covering obturator internus (white line)iliococcygeus � From the inner surface of ischial spine- Ischiococcygeus � Insertion. Pubococcygeus- post fibres into anococcygeal raphe (extends from anorectal junction to tip of coccyx)and tip of coccyx; puborectalisaround anorectal junction and form sling; puboanalis- run b/w sphincter ani externus and internus… inserted in wall of anal canal; pubovaginalis- form U shaped sling, ant fibres inserted into perineal body. Iliococcygeus- from white line, inserted into coccyx. Coccygeus- triangular in shape. Arises from apex of i. spine and sacrospinous ligament. Inserted into upper 2 pieces of coccyx and last piece of sacrum. Its fibres are not inserted into the bladder and urethra.

�Piriformis muscle-origin from sacrum and inserted into Greater trochanter of femur. �Gaps- 2 �Hiatus urogenitalis-transmitting urethra and vagina Bridged by muscles and fascia of urogenital triangle. �Hiatus rectalis-transmitting rectum. �Relations�Sup. Surface- Pelvic organs, pelvic cellular tissues, ureter, nerves �Inf. Surface-anatomical perineum. �Nerve supply- 3 rd and 4 th sacral nerve, inferior rectal nerve, perineal branch of pudendal nerve. �Blood supply- inferior gluteal artey of anterior division of internal iliac artery.

Functions �Support the pelvic organs specially pubovaginalis…. . weakness or tear causes prolpase �Counteracts the downward thrust of increased intrabdominal pressure during coughing, sneezing, straining by its contraction. �Guards the hiatus urogenitalis �Facilitates anterior internal rotation �Ischiococcygeus stabilises the sacroiliac and sacrococcygeal joints. �Steady the perineal body.

Thanks
- Slides: 113