Alterations of Hormonal Regulation Copyright 2014 2010 2006







")

 secretion Levels of")












 Adrenocorticotropic hormone (ACTH) deficiency")









- Slides: 38
Alterations of Hormonal Regulation Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc.
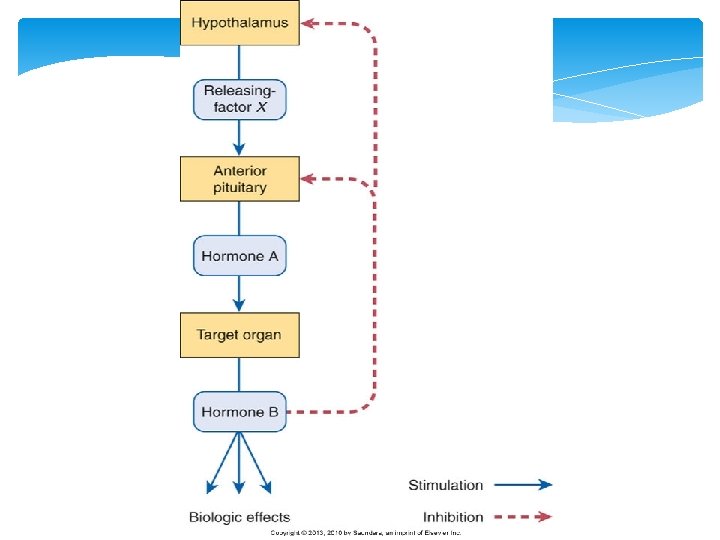
Mechanisms of Hormonal Alterations Too Much or Too Little Hormone Failure of feedback systems May fail to function properly May respond to inappropriate signals Dysfunction of an endocrine gland Inability to produce or obtain an adequate quantity of required hormone precursors Inability to convert precursors to the active hormone Excessive or inadequate hormone production Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 3
Mechanisms of Hormonal Alterations Too Much or Too Little Hormone or degradation Ectopic hormone release Nonendocrine sites Autonomous production; no feedback mechanisms Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 4
Mechanisms of Hormonal Alterations Target Cell Dysfunction Failure of target cell to respond to its hormone (hormone insensitivity) Receptor-associated disorders Decrease in the number of receptors Impaired receptor function Presence of antibodies against specific receptors Antibodies that mimic hormone action Unusual expression of receptor function Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 5
Mechanisms of Hormonal Alterations Target Cell Dysfunction Intracellular disorders Inadequate synthesis of a second messenger Cyclic adenosine monophosphate (c. AMP) Failure of the target cell to produce anticipated hormonal response Faulty response to hormone-receptor binding Failure to generate required second messenger Abnormal response to the second messenger Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 6
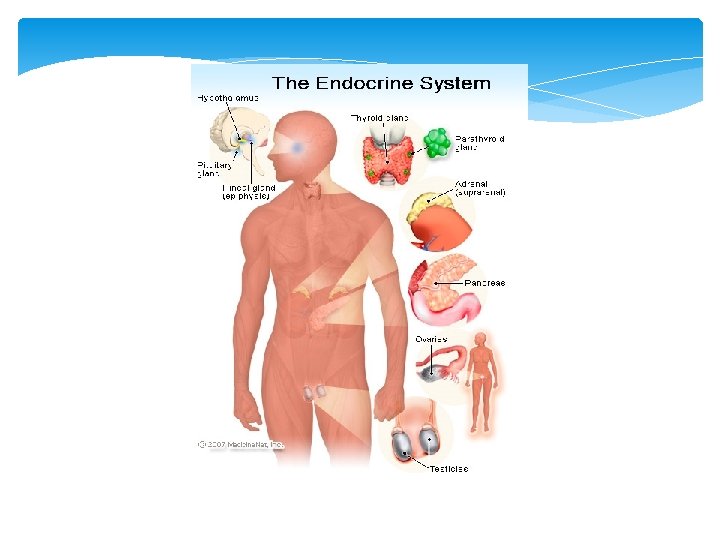
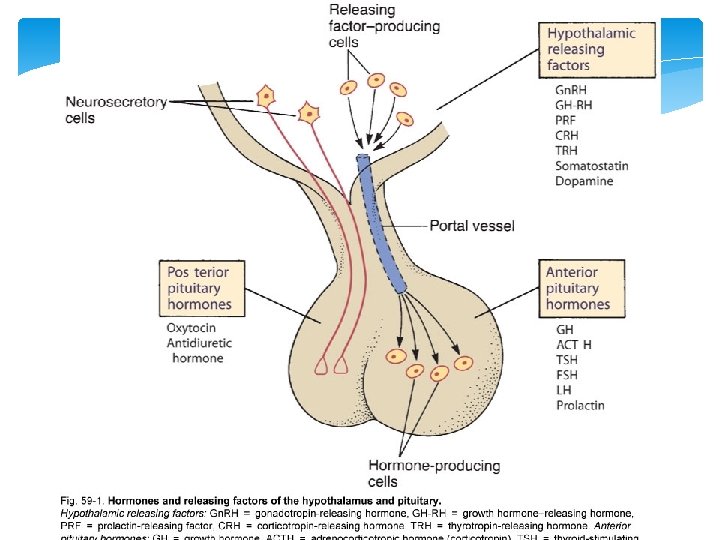
Pituitary Gland Located below the hypothalamus Under hypothalamic control Anterior and Posterior Pituitary Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 7
Hormones of the Anterior Pituitary Growth Hormone Stimulates growth in tissues and organs Promotes synthesis of adrenal hormones (cortisol & aldosterone) Promotes release/synthesis of thyroid hormones (TSH) Acts on the ovaries and testes Promote follicular growth Promote spermatogenesis Corticotropin Thyrotropin Follicle-Stimulating Hormone (Gonadotropins) Luteinizing Hormone (Gonadotropins) Acts on ovaries and testes Promote ovulation Promote androgen production Prolactin Stimulates milk production Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 10
Hormones of the Posterior Pituitary Oxytocin Facilitates uterine contractions at term Antidiuretic Hormone (ADH) Promotes renal conservation of water Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 11
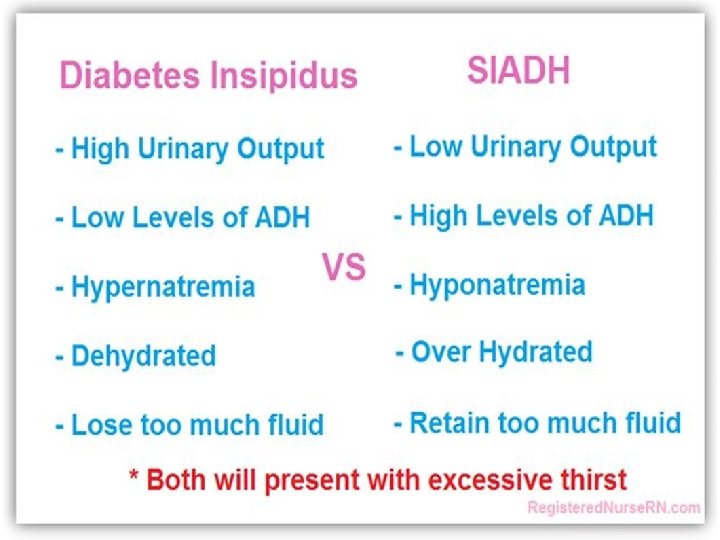
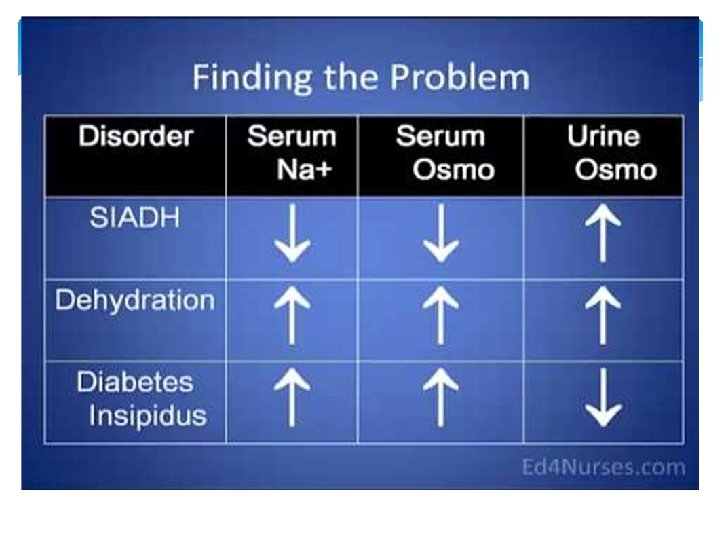
Diseases of the Posterior Pituitary Functioning Antidiuretic Hormone Effects Examples of Diseases Hyperfunction Too much Syndrome of inappropriate antidiuretic hormone (SIADH) secretion Hypofunction Too little Diabetes insipidus Neurogenic Nephrogenic Dipsogenic Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 12
Diseases of the Posterior Pituitary Syndrome of inappropriate antidiuretic hormone (SIADH) secretion Levels of antidiuretic hormone (ADH) are abnormally high. Ectopic secretion of ADH is the most common cause; is also common after surgery and some cancers. Water retention: Action of ADH on renal collecting ducts increases their permeability to water, thus increasing water reabsorption by the kidneys. For diagnosis, normal renal, adrenal, and thyroid function must exist. Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 13
Diseases of the Posterior Pituitary SIADH secretion Clinical manifestations Hyponatremia: Sodium <135 m. Eq/L Hypoosmolality: <280 m. Osm/kg Urine hyperosmolality: Higher than serum osmolality Hypervolemia Weight gain Serum sodium levels below 110 to 115 m. Eq/L: Can cause severe and sometimes irreversible neurologic damage Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 14
Diseases of the Posterior Pituitary SIADH secretion Treatment Correction of underlying causal problems Emergency correction of severe hyponatremia by the administration of hypertonic saline Conivaptan Most important: Fluid restriction between 800 and 1000 m. L/day Resistant or chronic SIADH: Demeclocycline Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 15
Vasopressin Antagonists Conivaptan Administration: IV infusion over 20 minutes IV infusion over 24 hours Hyponatremia due to high levels of ADH Blocks vasopressin receptors in kidneys Promotes excretion of water and retention of sodium for reabsorption Osmotic demyelination Infusion site reactions Hypotension hypokalemia CYP 34 A inhibitors Itraconazole, clarithromycin, ritonavir Indication: Mechanism: Adverse Effects: Drug Interactions: Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 16
Democycline Unique properties of Tetracyclines Democycline Indication: SIADH Toxic accumulation for pt. w/ renal impairment Tooth discoloration GI irritation Suprainfection Excessive urination Thirst Fatigue Adverse Effects: Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 17
Diseases of the Posterior Pituitary Diabetes insipidus Insufficiency of ADH Polyuria and polydipsia Partial or total inability to concentrate the urine Neurogenic Insufficient amounts of ADH Nephrogenic Insensitivity of the renal collecting tubules to ADH Dipsogenic Excessive fluid intake, lowering plasma osmolarity to the point that it falls below the threshold for ADH secretion Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 19
Diseases of the Posterior Pituitary Diabetes insipidus Is characterized by the inability of the kidney to increase permeability to water. Excretion of large volumes of dilute urine Increase in plasma osmolality: 300 m. Osm or more, depending on adequate water intake Urine output: 8 to 12 L/day; normal output: 1 to 2 L/day Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 20
Diseases of the Posterior Pituitary Diabetes insipidus Clinical manifestations Polyuria, nocturia, continual thirst Low urine-specific gravity: <1. 010 Low urine osmolality (<200 m. Osml/kg) Hypernatremia Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 21
Diseases of the Posterior Pituitary Diabetes insipidus Treatment Neurogenic: Administration of the synthetic vasopressin analog desmopressin acetate (DDAVP) Nephrogenic: Treatment of any reversible underlying disorders, discontinuation of etiologic medications, and correction of associated electrolyte disorders; administration of thiazide diuretic agents Dipsogenic: Effective management of water ingestion Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 22
Antidiuretic Hormone Desmospressin Rapid onset Long duration of action No vasoconstriction Indication: Replacement of ADH DI Nocturnal enuresis Hemophilia Structural analog of natural ADH Increased renal permeability to water Renal conservation of water Intranasal, IV, Sub Q, PO Water intoxication Mechanism: Administration: Adverse Effects: Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 23
Diseases of the Anterior Pituitary Functioning Hyperfunction Hypofunction Examples of Diseases Hormone Effects Hyperpituitarism Hypersecretion of growth hormone Hypersecretion of prolactin Primary adenoma Acromegaly Hypopituitarism Panhypopituitarism Adrenocorticotropic hormone (ACTH) deficiency Thyroid-stimulating hormone (TSH) deficiency Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) deficiency Growth hormone (GH) deficiency Prolactinoma Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 26
Diseases of the Anterior Pituitary Hypopituitarism Is characterized by the absence of selective pituitary hormones or the complete failure of all pituitary hormone functions. Pituitary is vascular and therefore vulnerable to ischemia and infarction. Causes Inadequate supply of hypothalamic-releasing hormones Damage to the pituitary stalk Inability of the gland to produce hormones Pituitary infarction Tumor or surgical removal Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 27
Diseases of the Anterior Pituitary Hypopituitarism Panhypopituitarism (all hormones affected) Adrenocorticotropic hormone (ACTH) deficiency Cortisol deficiency Thyroid-stimulating hormone (TSH) deficiency Altered metabolism Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) deficiency Lack of secondary sex characteristics Growth hormone (GH) deficiency Lack of growth in children Treatment Replacement of deficient hormone(s) Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 28
Diseases of the Anterior Pituitary Hyperpituitarism Commonly from benign, slow-growing pituitary adenoma Clinical manifestations Headache and fatigue Visual changes Hypersecretion of pituitary from tumor Hyposecretion of neighboring anterior pituitary hormones Specific medications to suppress tumor growth Transsphenoidal tumor resection Radiation therapy Hormone regulation: Control hypersecretion or replace deficient hormones Treatment Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 29
Diseases of the Anterior Pituitary Hypersecretion of GH Acromegaly Hypersecretion of GH during adulthood Slowly progressive pituitary adenoma Mortality: Cardiac hypertrophy; hypertension; atherosclerosis; type 2 diabetes mellitus, leading to coronary artery disease Other malignancies: Common Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 30
Diseases of the Anterior Pituitary Hypersecretion of GH Acromegaly Connective tissue proliferation Enlarged tongue, interstitial edema, increase in size and function of sebaceous and sweat glands, coarse skin and body hair Bony proliferation Large joint arthropathy, kyphosis, enlargement of facial bones and hands and feet, protrusion of the lower jaw and forehead, need for increasingly larger sized shoes, hats, rings, and gloves Symptoms of diabetes Polyuria and polydipsia Central nervous system (CNS) symptoms Headache, seizure activity, visual disturbances, papilledema Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 33
Diseases of the Anterior Pituitary Hypersecretion of GH Acromegaly Treatment Primary treatment: Transsphenoidal surgery or endonasal endoscopic surgery for the removal of the GH-secreting adenoma Radiation therapy Octreotide, octreotide long-acting, and lanreotide (somatostatin analogs) to lower GH levels Cabergoline (dopaminergic agonists) to lower prolactin levels Pegvisomant to block GH receptor Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 34
Somatostatin Analogs Mimic natural occuring somatostatin Suppress pituitary function Octreotide Adverse Effects: Gallstones GI distress IR and SR formulations Sub q inj. TID or IM inj. monthly Lanreotide Adverse Effects: Diarrhea Bradycardia Sub q inj. monthly Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 35
Growth Hormone Receptor Antagonist Pegvisomant Most effective drug for acromegaly Goal: Increase IGF-1 levels Side effects: well-tolerated Monitor Liver Enzymes Flu-like symptoms Administration: Indefinite administration Subcutaneous injection daily Costly Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 36
Diseases of the Anterior Pituitary Hypersecretion of prolactin Caused by prolactinomas Most common hormonally active pituitary tumor In women: Amenorrhea, galactorrhea, hirsutism, and osteoporosis In men: Hypogonadism, erectile dysfunction Treatment Bromocriptine, cabergoline (dopaminergic agonists): Rapid reduction in the size of the tumor and a reversal of the gonadal effects Resistant or intolerant to medication: Transsphenoidal surgery, endonasal endoscopic surgery, and radiotherapy Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 37
Dopamine Agonists Cabergoline Immediate effects that last for up to 14 days Monitor monthly until levels are normal Pituitary Adenoma Induces tumor suppression Copyright © 2014, 2010, 2006 by Mosby, Inc. , an imprint of Elsevier Inc. 38