Use of FFR in ACS Ganesh Manoharan Consultant





























 with intermediate leasion randomised to FFR or")

 with 50% stenosis (2/3 with ACS) who had intervention")




 - + STEMI (Late) + + NSTEMI +")

- Slides: 39
Use of FFR in ACS Ganesh Manoharan Consultant Cardiologist Regional Cardiology Department Royal Victoria Hospital Belfast, UK
Disclosures I am a consultant for: St. Jude Medical Medtronic Cardio. Vascular GDS Inc
Basic Principles of FFR Pa FFR = Pd Pd Pa Normal FFR = 1
Before Hyperaemia Conductance Arteries >500 µ Resistance Arteries <500 µ Microvasculature Pa Pd Pa 100 MACRO MICRO
With Maximal Hyperaemia Conductance Arteries >500 µ Resistance Arteries <500 µ Microvasculature Pa Pd Pa 100 MACRO MICRO
So, for Reliable and Reproducible FFR depends on: • Accurate calibration system • Accurate equalisation of catheter and pressure wire haemodynamics • Pressure wire in distal vessel • Maximum hyperaemia • Viable/non-stunned microvasculature
Factors Affecting FFR in ACS Clinical Syndrome: Unstable Angina Non-STEMI Assessment Time Point: Acute Subacute Late Artery Specific: Culprit vs Non Culprit STEMI
• 82 yrs old, male • Chronic renal failure • COPD • Acute STEMI • Primary PCI
Possible Options 1. Stent the LAD and the LCx in the same setting? 2. Bring the patient back to the cath lab in 4 to 8 days ? 3. Elective non-invasive assessment in the next coming days ? 4. Measure the FFR in the LAD and the LCx in the setting of primary PCI ?
What could happen to perfusion following revascularisation in STEMI: Acute Phase Epicardial segment: – Residual stenosis – Thrombus lining vessel wall – Diffuse spasm Impede flow Microvasculature: – Thrombus obstruction – No reflow – Necrosis – Stunning Impede Hyperaemia
What could happen to perfusion following revascularisation in STEMI: Late Phase Epicardial segment: – Residual stenosis True Physiological Lesion Microvasculature: – Cell death – Scarring Reduced perfusion territory / ‘ischaemic burden’ Impact of epicardial stenosis on perfusion is relative to perfused / viable area
DS=75% FFR=0. 50 Normal Myocardium Myocardial Infarction DS=75% FFR=0. 84 Scar Normal Myocardium
FFR=1. 0 CFR=2. 4 IMR=98
FFR could be higher/normal in infarct related artery post stent in acute phase FFR after PCI in 33 STEMI patients compared to 15 stable angina patients Cathet Cardiovasc Interven 2002; 57: 452 -459
FFR could be higher/normal in infarct related artery post stent in late phase Flow changes with and without microvascular dysfunction Cathet Cardiovasc Interven 2001; 54: 427 -434
FFR post recent MI • • • FFR and SPECT performed 3. 7 days post MI – 73%STEMI; Had to be >2 days for NSTEMI and >3 for STEMI 23 pts also had stress echo FU SPECT performed 11 weeks post to identify true positives and negatives Samady et al, J Am Coll Cardiol 2006; 47: 2187 -2193
Samady et al, J Am Coll Cardiol 2006; 47: 2187 -2193
FFR Cut-Off 0. 78 Samady et al, J Am Coll Cardiol 2006; 47: 2187 -2193
FFR in Patients with Previous MI Comparison of FFR in 57 pts >6 days post MI with SPECT pre and post PCI De Bruyne B et al. Circulation 2001; 104: 157 -162
FFR in Patients with Previous MI Sensitivity and specificity curves of FFR to detect flow maldistribution at MIBI perfusion scan in population as a whole. De Bruyne B et al. Circulation 2001; 104: 157 -162
FFR in Patients with Previous MI FFR depends on mass of viable myocardium De Bruyne B et al. Circulation 2001; 104: 157 -162
What about FFR in Non-Culprit Stenoses During the Acute Phase of a Myocardial Infarction Ntalianis A et al JACC interv 2010
FFR in Non-Culprit Stenoses During the Acute Phase of a Myocardial Infarction • 104 patients with acute MI • 112 non-culprit stenoses • FFR - acute phase and - 1 month later In 2/112 stenoses, the FFR value was >0. 80 at the acute phase but <0. 75 at follow-up VARIABILITY OF VARIATIONS: 5% Ntalianis A et al JACC interv 2010
Results VARIABILITY OF VARIATIONS: 12% Ntalianis A et al JACC interv 2010
FFR in Non-Culprit Stenoses During the Acute Phase of a Myocardial Infarction In patients with a high LVEDP the FFR measured at the acute phase is slightly overestimated as compared to the measurement performed 1 month later Ntalianis A et al JACC interv 2010
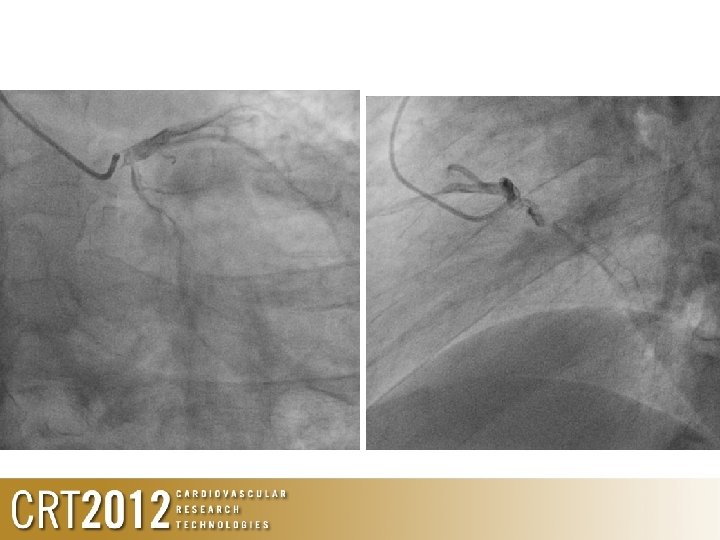
FFR=0. 88 FFR=0. 95
FFR in the STEMI: Culprit vs Non-Culprit Artery Culprit – Acute Phase: Not recommended – Late Phase: • Can be used, useful in tailoring therapy • Can be normal in setting of ‘severe’ angiographic stenosis but non-viable myocardium • Non-Culprit – Acute Phase: • Can be used • Caution in high LVEDP patients
What about NSTEMI patients? ACS Patients (N=70) with intermediate leasion randomised to FFR or stress perfusion scan Leesar et al. J Am Coll Cardiol 2003; 41: 1115 -1121
FFR in NSTEMI 1 year events Leesar et al. J Am Coll Cardiol 2003; 41: 1115 -1121
FFR in ACS Patients (N=201) with 50% stenosis (2/3 with ACS) who had intervention deferred based on FFR Potvin et al. Am J Cardiol 2006; 98: 289 -297
FFR in ACS New Engl J Med 2009; 360: 213 -24
Baseline Characteristics
FAME patients with and without ACS
FAME De Bruyne Onset Samady When could you assess the culprit artery post ACS? 4 5 6 Time (days)
In Summary Culprit Non-Culprit STEMI (Acute) - + STEMI (Late) + + NSTEMI + +
Conclusions • FFR of culprit artery in acute STEMI is not recommended • FFR of the non-culprit artery in acute ACS is reliable, but be cautious in setting of raised LVEDP • FFR assessment of the culprit artery in ACS is best assessed after a minimum of 7 days