FFR i FR A Review of Their Differences


 Resting Gradients i. FR, Pd/Pa Flow Resistance")

")


 Own")

 Menon M, et al. . Euro. Intervention. 2015 Jul; 11(3):")





")

")
")

")


")
 of i. FR and Pd/Pa")
 provide biased")



")





")








- Slides: 45
FFR & i. FR: A Review of Their Differences and Emerging Available FFR Systems Edo Kaluski MD, FACC, FESC, FSCAI Cath Lab Director RPH & Guthrie Health System Professor of Medicine at Rutgers NJMS
Edo Kaluski MD, FACC, FESC, FSCAI I have no relevant financial relationships Speaker for : Amgen, Zoll, Astra. Zeneca, DSI, Janssen Research support grants: Janssen, Astra. Zeneca,
Physiologic Lesion Assessment FFR (adenosine, NTP, Contrast) Resting Gradients i. FR, Pd/Pa Flow Resistance CFVR, Peak Hyperemic flow IMR Anatomic Characteristics (OCT, IVUS)
I: Available Systems
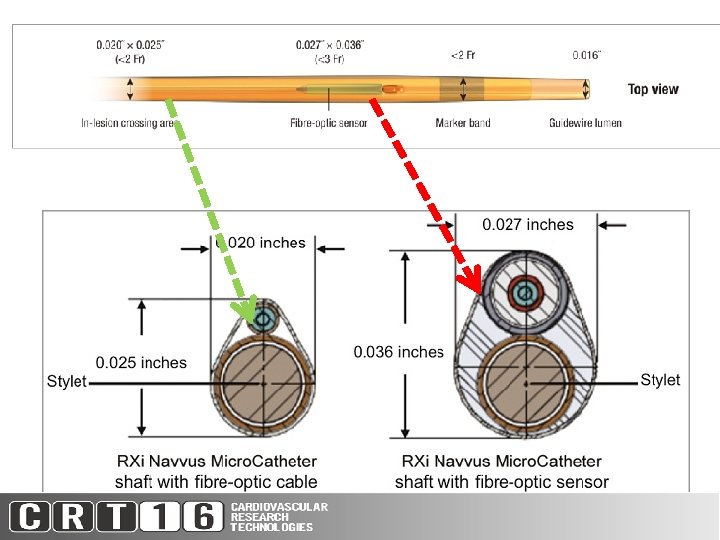
Systems for FFR i. FR CFR Measurements Company Console options Lengths Pressure wire (cm) Advant age Shortcoming St. Jude Medical Ilumen Optis FFR OCT 175/300 0. 014” Low profile ACIST RXi FFR 150 (335) VOLCANO Combo. Map 6800 Sync. Vision Core & Core mobile FFR, i. FR, CFR FFR, i. FR, IVUS Opsense FFR Opto. Monitor 175/300 FFR, i. FR, IVUS 175 Aeris 0. 014” Certus 0. 014” Navvus Fiber-optic (shaft 0. 20 X 0. 27”) Microcatheter Own wire Less drift Prime wire prestige Low 0. 014” profile Verrata 0. 014” Flo. Wire Combo High profile (0. 027 X 0. 036”) Cost of wire Fiber-optic wire 0. 014 Not FDA approved Low profile 1) If you want i. FR you must have Volcano 2) If you want CFR purchase the Volcano Combo. Map 6800 (with Flo. Wire or Combo. Wire) 3) To use your conventional PCI wire Use ACIST RXi (Navvus)
FFR Catheters
Catheter Technology: Quality Indicators Opsens Opto. Wire. TM Pressure Guidewire Acist Navvus. TM Pressure catheter St. Jude Medical Pressire. Wire. TM Pressure Guidewire Volcano Verrata. TM Pressure Guidewire Device Pressure guidewire Catheter Pressure guidewire Sensor technology Fiber optic Polarization interferometry Fiber optic Fabry. Pérot Piezo-resistive (Electrical) Pressure accuracy ± 1 mm. Hg plus ± 1% of reading (-30 to 50 mm. Hg) +/-3% of reading or +/-3 mm. Hg, whichever is greatest +/-1 mm. Hg plus +/ Not specified in -3% of reading IFU Pressure range -30 to 300 mm. Hg Zero thermal effect < 0. 3 mm. Hg / °C < 0. 4 mm. Hg/deg C < 0. 3 mm. Hg/deg C Not specified in IFU Zero drift < 1 mm. Hg / h < 7 mm. Hg/hour Courtesy: Mona Tiren (Opsense Medical) < 7 mm. Hg/hour -30 to 300 mm. Hg Not specified in IFU Per FDA approval: <5 mm. Hg/10 mi
ACIST Rxi & Navvus Microcatheter 150 cm Rapid Exchange (shaft 0. 020/0. 027”) Own wire Less drift High profile Fibre -optic sensor Menon M, Jaffe W, Watson T, Webster M. Assessment of coronary fractional flow reserve using a (length 335) (. 027 X. 036”) monorail pressure catheter: the first-in-human ACCESS-NZ trial. Euro. Intervention. 2015 Jul; 11(3): 257 -63. doi: 10. 4244/EIJV 11 I 3 A 51. Pub. Med PMID: 26196752.
Menon M, Jaffe W, Watson T, Webster M. Assessment of coronary fractional flow reserve using a monorail pressure catheter: the first-in-human ACCESS-NZ trial. Euro. Intervention. 2015 Jul; 11(3): 257 -63. doi: 10. 4244/EIJV 11 I 3 A 51. Pub. Med PMID: 26196752. Comparator SJM Certus Wire
ACCESS NZI Study (n=50) Menon M, et al. . Euro. Intervention. 2015 Jul; 11(3): 257 -63 * Certus SJM * +4% -4% 1) 95% limits of agreement-13 to + 10%) 2) Most excessive disagreement is between 0. 70 -0. 90
ACCESS NZI Study Menon M, Jaffe W, Watson T, Webster M. Assessment of coronary fractional flow reserve using a monorail pressure catheter: the first-in-human ACCESS-NZ trial. Euro. Intervention. 2015 Jul; 11(3): 257 -63. * * Certus SJM *
ACCESS NZI Study Menon M, Jaffe W, Watson T, Webster M. Assessment of coronary fractional flow reserve using a monorail pressure catheter: the first-in-human ACCESS-NZ trial. Euro. Intervention. 2015 Jul; 11(3): 257 -63. * Certus SJM
II: Summary of Research on FFR versus i. FR & resting gradients
1: FFR is not i. FR
Bland Antman Analysis FFR vs i. FR Jeremias et al JACC 2014 o i. FR exceeds FFR by average 10% (95% CI -6% to 26%) o Bidirectional scatter more pronounced <0. 85 (range 0. 52 -0. 85) Jeremias et al JACC 2014 THE i. FR-FFR Gradient is unpredictable!
Bland Antman Analysis FFR vs Pd/Pa exceeded FFR by +14% (95% CI -1%-+0. 29%) Scatter more pronounced <0. 85 (range 0. 54 -0. 90) Jeremias et al JACC 2014 Pd/Pa is consistently higher than FFR (∆ variable)
2. IFR is not independent of hyperemia
VERIFY: Effect of hyperaemia on i. FR (20% drop in i. FR during hyperemia) Berry et al. JACC 2013 (epub) 0. 84± 016 20% 0. 64± 018 0. 84± 0. 16 to 0. 64± 0. 18 Wait 30 s from last contrast injection. What else drops i. FR and reduces the i. FR-FFR gradient?
VERIFY: Effect of hyperaemia on i. FR (20% drop in i. FR during hyperaemia) Berry et al. JACC 2013 (epub) 0. 84± 016 A= Terazocin B= Norvasc C= Verapamil IA D=NTG IV E= IV Nitroprusside 20% 0. 64± 018 A B C D E 0. 84± 0. 16 to 0. 64± 0. 18
3. The resistance during the i. FR is not minimal (2. 5 fold that of FFR (VERIFY study)
Myocardial Resistance i. FR vs. FFR Myocardial Resistance (Pressure/Flow Velocity; R R == V/I) if. R Resistance 2. 46± 1 fold higher (Wider variance). 4. 84± 2. 55 Hg/cm/s 2. 06± 0. 83 Hg/cm/s WFP Johnson et al. JACC 2013 epub 9% of patients resistance drops by <10%
4. The reproducibility of FFR is superior i. FR
VERIFY: Reproducibility of FFR is superior to i. FR FFR i. FR 95% limits of agreement -4 to 4% 95% limits of agreement -7 to 8% Berry et al. JACC 2013 (epub) FFR significantly better reproducibility (p= 0. 0001) with the i. FR differences between measurements X 2. 5 -4. 4 larger variance than FFR
5. For guessing FFR, i. FR not better than Pd/Pa? (VERIFY & RESOLVE studies) The ROC cut-point correlating with FFR 0. 80: -0. 90 for i. FR -0. 92 for Pd/Pa i. FR Pd/Pa cutoff AUC (ROC) Accuracy Correlation Bias Precision 0. 90 0. 92 0. 81 80. 4% 0. 66 +10% (95% CI -6 -+26) ± 16% 0. 82 81. 5% 0. 69 +14% (95% CI -1 -29) ± 15% RESOLVE: Jeremias A. et al JACC 2014
6. The overall diagnostic accuracy (for appropriate lesion classification) of i. FR and Pd/Pa is 80%. cutoff AUC (ROC) Accuracy Correlation Bias Precision i. FR 0. 90 0. 81 80. 4% 0. 66 +10% (95% CI -6 -+26) ± 16% Pd/Pa 0. 92 0. 82 81. 5% 0. 69 +14% (95% CI -1 -29) ± 15% RESOLVE: Jeremias A. et al JACC 2014
7. Resting pressure derived indices of stenosis severity (i. FR & Pd/Pa) provide biased estimate of FFR on average, and an uncertain estimate of FFR in individual cases Cutoff AUC (ROC) Accuracy Correlation Bias Precision i. FR 0. 90 0. 81 80. 4% 0. 66 +10% (95% CI -6 -+26) ± 16% Pd/Pa 0. 92 0. 82 81. 5% 0. 69 +14% (95% CI -1 -29) ± 15% RESOLVE: Jeremias A. et al JACC 2014
III: The FFR Edge
What is the FFR Edge over i. FR ü Validated against non-invasive gold standard New Engl J Med 1996; 334; 1703 -8 ü Multiple large registries supporting its usefulness & reproducibility in a variety of clinical and anatomic settings. Circulation 2014; 129: 1860 -70. ü Large, multicenter RCTs & registries demonstrating clinical benefit (DEFER, FAME 1, FAME 2) & guideline supported Circulation 2001; 103: 2928 -34, J Am Coll Cardiol 2007; 49: 2105 -11, Eur Heart J 2015; in press N Engl J Med 2009; 360: 213 -24, J Am Coll Cardiol 2010; 56: 177 -84, Lancet 2015 Aug 28 N Engl J Med 2012; 367: 991 -1001, N Engl J Med 2014; 371: 1208 -17 ü Validated & implemented for cost-effective & cost-saving care Circulation 2010; 122: 2545 -50 Circulation 2013; 128: 1335 -40
IV: The i. FR Edge
i. FR Edge 1. Reduced need for vasodilator (reducing: cost, procedure time, side effects) 2. Repeated multi-lesion assessment before and after treatment
Workflow of i. FR 0. 89 -0. 90 0. 86 PCI 0. 91 0. 93 i. FR No PCI Pd/Pa No PCI Perform FFR measurement But Since i. FR-FFR gradient is 10% with 95% CI of -6 to +26% Vasodilator to i. FR≤ 0. 95
Jeremias et al JACC 2014 95% agreement with FFR require 65% of lesions receive adenosine
Multi-lesion Assessment & Rx without Adenosine infusion 1. Identify arteries causing ischemia 2. Identify lesions within the artery (pullback with co-registration) 3. Predict the likely improvement in CAD physiology prior to PCI 4. Optimize PCI & stenting
CP & Inferior Ischemia on Stress Echo i. FR & FFR for Dummies? 0 0. 8 3 0. 9 0. 75 0. 90 0. 71 0. 88 1 What’s the effect of proximal or distal lesions on the measured i. FR & FFR 2. What’s the hemodynamic consequence of PCI of any one of the lesions 3. Effect of residual gradient post PCI in a diffusely diseased vessel.
Dyspnea & Positive Stress Echo LAD Territory (do you understand what you measured? . . . implications? ) What are you going to stent? 0. 78 0. 91 A 0. 71 B 0. 85 C 0. 71 0. 83
V: Role of i. FR ? (validation studies)
Functional Lesion Assessment of Intermediate stenosis to guide Revascularisation Intermediate lesion requiring physiological assessment In ACS : intermediate non-culprit lesion N=2500, 1: 1 Randomisation FFR Guided PCI FFR>0. 8 Defer PCI FFR≤ 0. 8 Perform PCI i. FR Guided PCI i. FR≥ 0. 9 Defer PCI 30 day, 1, 2 and 5 yr follow-up i. FR<0. 9 Perform PCI
SYNTAX 2 Synergy stent No PCI
VI: Conclusions
1. FFR has considerably more clinically validated than i. FR
2: Until the prognostic value of i. FR and CFR are validated FFR should be the method of choice for physiologic lesion assessment.
3. i. FR advantages are: ü Time & vasodilator saving ü Assessment of sequential lesions without vasodilator before & after PCI
4. The interpretation of both FFR & i. FR pullbacks in the presence of diffuse disease is not straightforward !
THANK YOU FOR YOUR ATTENTION