When IVUS When FFR Assessing Intermediate Lesions Itsik


















 % MT (n=441) P-Value 4. 3 12. 7 <0.")





 92 (53. 2%) (65. 7%) with")

 r= 0. 36,")










- Slides: 45
When IVUS? When FFR? Assessing Intermediate Lesions Itsik Ben-Dor, MD Washington Hospital Center
Itsik Ben-Dor, MD I/we have no real or apparent conflicts of interest to report.
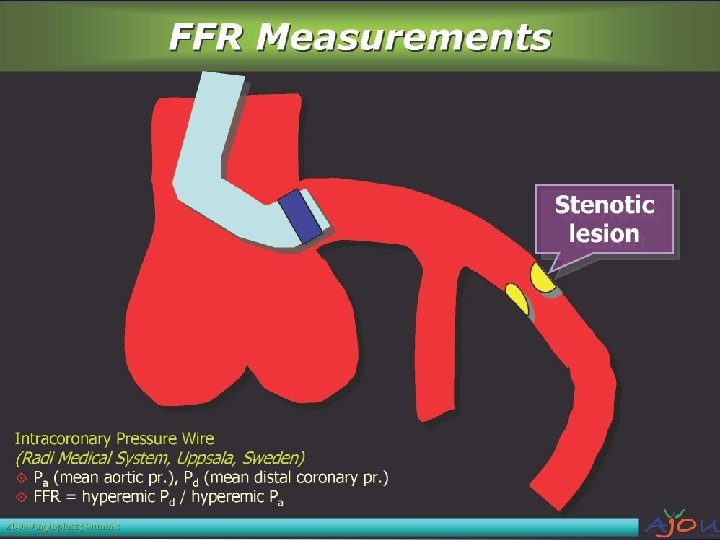
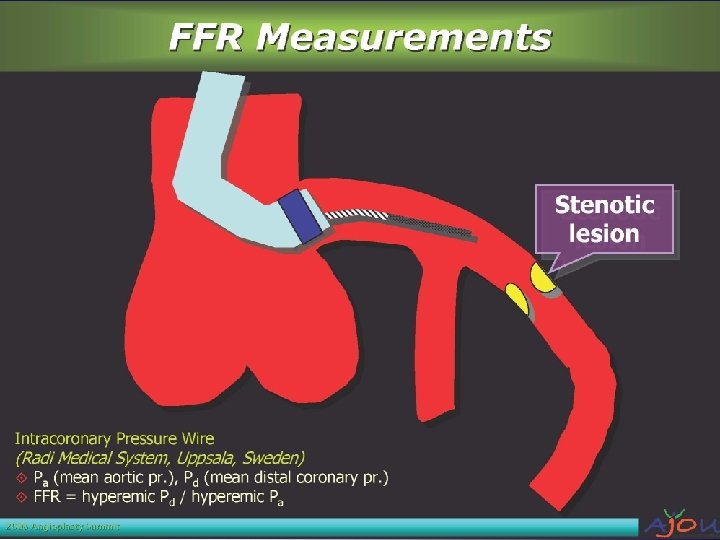
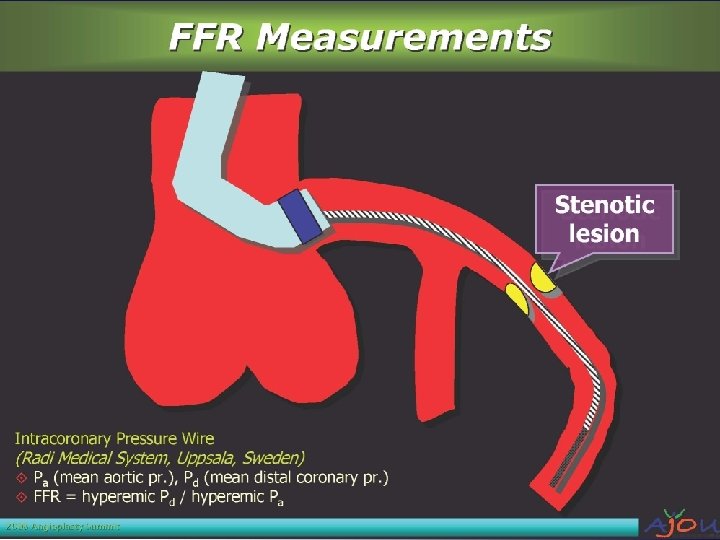
Case 58 -year-old male with new onset of chest pain with exercise Would you treat this lesion ? Need more information? IVUS? FFR?
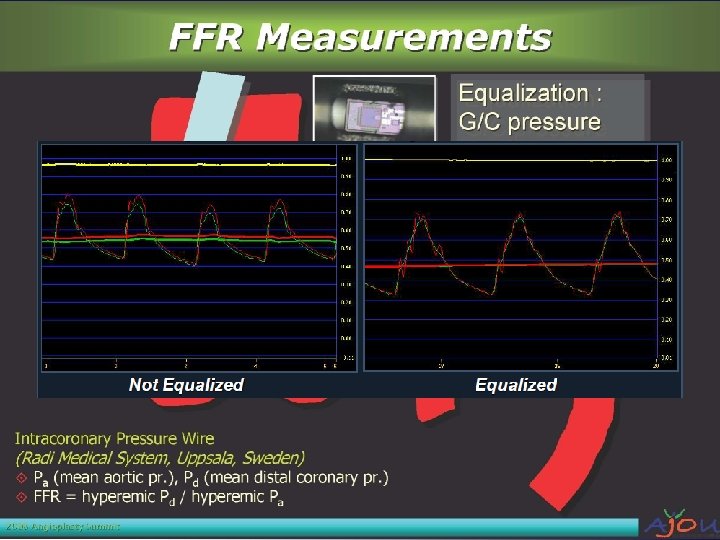
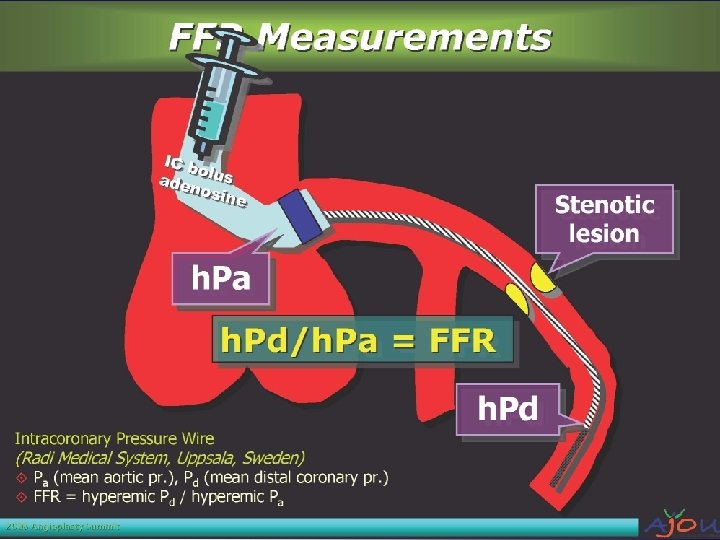
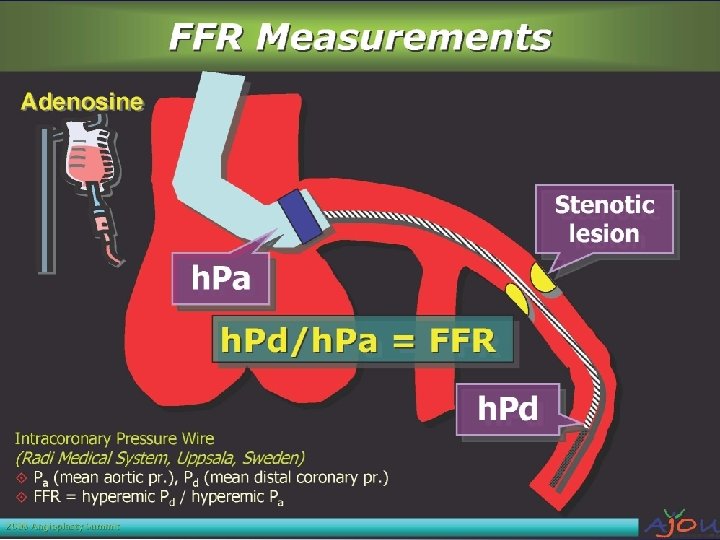
FFR
Intravascular Ultrasound IVUS
IVUS – Catheters Mechanical Transducer Solid State Transducer
1 slide s n te is s o e nc 2 slides e r e f e r R Lumen area (mm 2) Plaque burden (%) (total area-lumen)/total area Remodeling Index (total area/ref total area) e st n is s o S
MLA 2 2. 9 mm 2 4. 3 mm ?
Clinical data on outcome-based IVUS No prospective randomized study has ever shown better PCI outcome by using IVUS in DES era
IVUS final lumen area determines prognosis 2 Where did the number 4 mm Clinical follow up in 357 intermediate lesions in 300 patients deferred intervention IVUS imaging comeafterfrom? Death/MI/TLR DM no-DM 2 -3 3 -4 4 -5 IVUS MLA (mm 2) 5 2 -3 3 -4 4 -5 ≥ 5 IVUS MLA (mm 2) Death/MI/TLR at mean 13 months = 8% Death/MI/TLR at mean 13 months = 4. 4% in lesion with MLA >4 mm 2 Only independent predictor of death/MI/TLR was IVUS MLA WHC: Abizaid et al. Circ 1999; 100: 256 -261
PROSPECT Study
PROSPECT Study Stone et al. N Engl J Med 2011; 361: 226 -35
PROSPECT: Predictors of Non Culprit Lesion Events Stone et al. N Engl J Med 2011; 361: 226 -35
Clinical data on outcome-based FFR
DEFER 5 -Year Results Event-Free Survival Cardiac Death and MI N=325 (Pijls et al. J am Coll Cardiol 2007; 49: 2105 -11)
Fractional Flow Reserve Versus Angiography for Guiding Percutaneous Coronary Intervention in Patients With Multivessel Coronary Artery Disease (FAME I) FFR-Guided PCI performed on indicated lesions only if FFR <0. 80 Lesions warranting PCI identified Randomized Primary Endpoint Composite of death, MI and repeat revasc. (MACE) at 1 year Key Secondary Endpoints Individual rates of death, MI, and repeat revasc. , MACE, and functional status at 2 years Pijls N. et al. J Am Coll Cardiol 2010; 56: 177– 84 Angio-Guided PCI performed on indicated lesions
Fractional Flow Reserve Versus Angiography for Guiding Percutaneous Coronary Intervention in Patients With Multivessel Coronary Artery Disease (FAME 2 years) Absolute Difference in MACE-Free Survival 2 -Year Follow-Up of the FAME , , Fractional Flow Reserve Versus Angio guided Angiography for Multivessel Evaluation’’ FFR guided 1 month 2. 9% 6 months 4. 9% 12 months 5. 1% 24 months 4. 7% Conclusion: In pts with multivessel CAD undergoing PCI, routine measurement of FFR as compared with PCI guided by angiography alone results in a significant reduction of Pijls N. et al. J Am Coll Cardiol 2010; 56: 177– 84 the rate of mortality and myocardial infarction
FAME II Trial Design Stable patients with 1, 2, or 3 vessel CAD evaluated for PCI with DES n=1220 FFR in all target lesions Registry Randomized Trial At least 1 stenosis with FFR ≤ 0. 80 (n=888) All FFR > 0. 80 (n=322) Randomization 1: 1 PCI + MT MT MT 50% randomly assigned to follow-up Primary Endpoint: Death, MI, Urgent Revascularization at 2 years
Trial Results FFR-Guided PCI (n=447) % MT (n=441) P-Value 4. 3 12. 7 <0. 001 Death 0. 2 0. 7 0. 31 Myocardial Infarction 3. 4 3. 2 0. 89 Urgent Revascularization 1. 6 11. 1 <0. 001 Free from Angina (1 month) 71 48 <0. 001 Primary Endpoint De Bruyne, et al. New Engl J Med 2012; 367: 991 -1001.
Assessment of intermediate coronary lesions
QCA
FAME Study 1329 lesions in the FFR-guided arm 65% 4% 37% 20%FFR >0. 80 (44%) (37%) (18%) 50 -70% 71 -90% 91 -100% Angiographic Diameter Stenosis Tonino et al. , JACC 2009
Correlation of FFR with % QCA Diameter Stenosis left main coronary artery Inappropriate decision Based on angiography = 29% Hamilos M, et al. Circulation 2009; 120: 1505 -1512
Correlation between Fractional Flow Reserve and Intravascular Ultrasound Lumen Area in Intermediate Coronary Artery Stenosis • 205 intermediate lesions in 185 patients were studied consecutively by QCA, IVUS, and FFR during diagnostic coronary angiography between July 2007 and January 2011 • Intermediate coronary stenosis was defined by QCA as a stenosis 40 -70% • Excluded: Patients with acute myocardial infarction, lesions in small vessels <2. 5 mm reference vessel diameter, or with more than one lesion in the studied vessel Ben-Dor Euro. Intervention. 2011 Jun; 7(2): 225 -33.
IVUS vs. FFR 193 lesions (excluding 12 LM) 92 (53. 2%) (65. 7%) with MLA <3 <4 mm 41 mm 22 had non ischemic FFR ≥ 0. 8 2 2 had (12. 9%) with MLA >3 mm 315 (5. 6%) with MLA >4 mm had ischemic FFR <0. 8 Ben-Dor Euro. Intervention. 2011 Jun; 7(2): 225 -33.
IVUS cut-off for ischemic FFR<0. 8 C=0. 73 Percentage 3. 09 mm 2 (sensitivity 69. 2%, specificity 71. 5%) Ben-Dor Euro. Intervention. 2011 Jun; 7(2): 225 -33.
IVUS vs. FFR for intermediate coronary stenosis (n=205 lesions, 185 patients) r= 0. 36, p<0. 001 r= 0. 25, p<0. 001 r= -0. 43, p<0. 001 r= -0. 33, p<0. 001 Ben-Dor Euro. Intervention. 2011 Jun; 7(2): 225 -33.
Correlation of FFR with MLA by reference vessel diameter r= 0. 2, p=0. 11 MLA r= 0. 44, p<0. 001 FFR N=76 FFR r= 0. 43, p<0. 001 MLA N=50 N=79 FFR Ben-Dor Euro. Intervention. 2011 Jun; 7(2): 225 -33.
IVUS cut-off for ischemic FFR <0. 8 by reference vessel diameter 2. 7 mm 2 C=0. 74 C=0. 77 Percentage 2. 4 mm 2 C=0. 70 Percentage 3. 6 mm 2 Ben-Dor Euro. Intervention. 2011 Jun; 7(2): 225 -33.
All lesion with MLA<3 mm 2 FFR <0. 8 N=38 FFR >0. 8 N=39 P value 22(57. 9%) 14(35. 9%) 0. 05 3(7. 9%) 4(10. 3%) 0. 9 10(26. 3%) 11(28. 2%) 0. 85 3(7. 9%) 10(25. 6%) 0. 03 Proximal 19(50. 0%) 25(64. 1%) 0. 21 Mild 17(44. 7%) 10(25. 6%) 0. 07 Distal 2(5. 3%) 4(10. 3%) 0. 67 Lesion length (mm) 19. 2± 8. 5 12. 5± 6. 4 0. 01 57. 8± 15. 6 0. 01 6. 6± 2. 5 0. 17 18(46. 2%) 0. 4 Lesion characteristics LAD Circumflex RCA Diagonal/Ramus/Marginal Pressure drops across stenosis: 65. 6± 7. 8 Luminal area MLA Reference diameter (mm) 7. 5± 1. 9 Lesion length Length Reference diameter 2. 5 -3 mm 14(36. 8%) Flow Reference vessel Area stenosis (%) Reference diameter 3 -3. 5 mm 19(50. 0%) 16(41. 0%) 0. 42 Reference diameter >3. 5 mm 5(13. 2%) 5(12. 8%) 0. 9 Ben-Dor Euro. Intervention. 2011 Jun; 7(2): 225 -33.
THE F 1 RST TRIAL Results Study participating Sites Site Name City, State Country Principal Investigators # Enrolled Washington Hospital Center Washington, DC USA Ron Waksman, MD 91 University Hospital Krakow, Poland Jacek Legutko, MD 59 Barnes Jewish Hospital St. Louis, MO USA Jasvindar Singh, MD 49 Hamot Medical Center Erie, PA USA Quentin Orlando, MD 33 St. Luke’s Health Center Kansas City, MO USA Steven Marso, MD 27 Patients First Washington, MO USA Timothy Schloss, MD 26 Ohio Heart Research Columbus, OH USA John Tugaoen, MD 7 Dartmouth Medical Center Lebanon, NH USA James De. Vries, MD 6 Liverpool Heart and Chest Liverpool, United Kingdom Nicholas Palmer, MD 5 Städtische Kliniken Neuss, Germany Michael Haude, MD 1 350 patients with 369
F 1 RST Overall Population Analyses 1. 2 1 Probability 0. 8 0. 6 MLA: 3. 07 mm 2 Sensitivity 0. 64 Specificity 0. 65 C= 0. 65 0. 4 0. 2 specifity _SENSIT_ 0 0 2 4 6 MLA 8 10 12
RVD < 3. 0 mm RVD 3. 0 to 3. 5 mm RVD > 3. 5 mm MLA
F 1 RST Optimal MLA Cut-off Values N MLA Cut-off mm 2 C-Statistic Accuracy RVD <3. 0 mm 175 2. 68 0. 64 65. 7% RVD 3. 0 -3. 5 mm 92 3. 16 0. 69 70. 7% RVD >3. 5 mm 62 3. 74 0. 64 67. 7% 245 2. 92 0. 66 67. 8% 85 3. 07 0. 64 68. 2% Vessel Size LV Functional Status Normal LV Reduced LV (<50% / Prior MI)
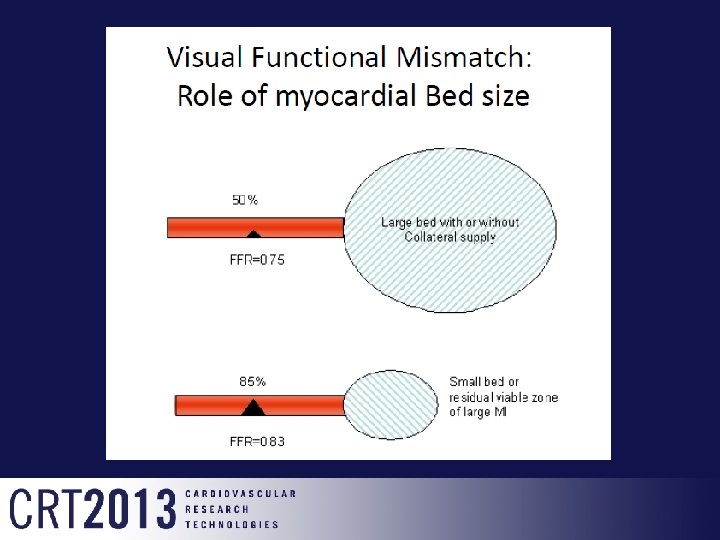
Reference vessel size ? Reference diameter Area % stenosis for 4 mm 2 2. 5 mm 4. 9 mm 2 18% 3 mm 7. 1 mm 2 44% 3. 5 mm 9. 6 mm 2 58% 4 mm 12. 5 mm 2 68% Area stenosis >70% Diameter stenosis >50%
Reference vessel size ?
Conclusions • Anatomic measure of intermediate coronary lesion obtained by IVUS show only a moderate correlation to FFR values. • The MLA is vessel size dependent and better correlated in large diameter vessels. • The optimal MLA cutoff that corresponds with an FFR < 0. 8 is ~3. 0 mm 2 • The optimal MLA cutoff varied with regards to vessel location, vessel size and, lesion severity • However, the utility of IVUS MLA as an alternative to FFR for guidance of intervention of intermediate lesions may be limited and should be tested clinically