FFR or i FR Advantage Disadvantage of Physiology





























 Correlation between FFRCT & FFR Nørgaard BL, et")

 X-ray")






 PCI deferred 31% PCI performed 69% Lesions")




- Slides: 47
FFR or i. FR: Advantage & Disadvantage of Physiology in Daily Practice Takashi Akasaka, MD, Ph. D, FESC, FAPSC, FJCS Department of Cardiovascular Medicine Wakayama Medical University
disclosure Takashi Akasaka, MD, Ph. D Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. • Grant/Research Support: • Consulting Fees/Honoraria: Abbot Vascular Japan Heart. Flow Japan Nipro Inc. Terumo Inc. Abbott Vascular Japan Boston Scientific Japan Nipro Inc. Terumo Inc.
Concept of FFRmyo Pijls N, et al. Circulation 1 993; 86: 1354 -1367
No stenosis Measurement of FFRmyo Pa FFR = Max flow under the condition with stenosis / without stenosis Pd During HE; Pd=Pa Pd / Pa=1. 0 Stenosis(A) Pa Pd A FFR (A) = Pd / Pa during HE Rest Pd<Pa, During HE Pd <<Pa
Advantage of FFR in daily clinical practice Ø Easy to measure mean coronary pressure by PGW. Ø Normal value of FFR is 1. 0. Ø Cut-off value for demonstrating ischemia is 0. 75. Ø Cut-off value for revascularization is 0. 8.
Clinical Evidence in FFR DEFER: J Am Coll Cardiol 2007; 49: 2105 -2111 FAME I: New Engl J Med 2009; 360: 213 -224 absolute difference in MACE-free survival FFRguided 30 days 2. 9% 90 days 180 days Angio-guided 3. 8% 360 days 4. 9% 5. 3% Cumulative incidence (%) FAME II: New Engl J Med 2014; 371: 1208 -1218 PCI+OMT vs. OMT: PCI+OMT vs. Registry: p<0. 001 OMT vs. Registry: 30 25 RCT: OMT RCT: PCI+OM T REGISTRY: OMT HR 0. 32 (0. 19 -0. 53); HR 1. 29 (0. 49 -3. 39); p=0. 61 HR 4. 32 (1. 75 -10. 7); p<0. 001 20 15 10 5 0 No. at risk MT PCI+MT Registry 0 1 2 3 4 441 447 166 414 156 370 388 145 322 351 133 283 308 117 5 6 7 8 Months after randomization 253 277 106 220 243 93 192 212 74 162 175 64 9 10 11 12 127 155 52 100 117 41 70 92 25 37 53 13 Intracoronary imaging & physiology in ESC guideline 2014 Eur Heart J. 2014; 35: 2541 -2619
Relationship between FFR & functional tests Pijls N. H. J. , et al. N Engl J Med 1996; 334: 1703 -1708 Exercise test Thallium scan Stress echo 0. 3 0. 4 0. 5 0. 6 0. 75 Fractional flow reserve (FFR) 0. 8 0. 9 1. 0
Relationship between FFR & other tests Kern MJ & Samady H. J Am Coll Cardiol 2010; 55: 173 -185 Authors Number Auth ors Auth ors Auth ors Auth ors Ischemic tests Best cut-off value Accuracy
Conceptual relationship between FFR & outcomes 0. 70? 0. 85? Johnson NP, et al. J Am Coll Caridol 2014; 64: 1641 -1654
Hazard Ratio of MACE in each FFR Ahn JM, et al. Circulation 2017; 135: 2241 -2251
Incidence of MACE in deferred lesions according to each FFR group Ahn JM, et al. Circulation 2017; 135: 2241 -2251
Incidence of MACEs in deferred lesions Ahn JM, et al. Circulation 2017; 135: 2241 -2251
Key integrated information from hundreds of studies Risk to die or experience myocardial infarction in the next 5 years related to a coronary stenosis: Ø Non-ischemic stenosis; <1% per year (NUCLEAR studies, DEFER, FAME, PROSPECT, CCTA) Ø Ischemic stenosis, if left untreated; 5 -10% per year (Many historical registries, ACIP, etc. ) Ø Stented stenosis; 2 -3% per year (e. g. DEFER, FAME, SYNTAX, many large studies & registries)
Cox Model 1 year MACE Rate estimated by FFR Johnson NP, et al. J Am Coll Caridol 2014; 64: 1641 -1654
Hazard Ratio of Cardiac Death & MI in each FFR Ahn JM, et al. Circulation 2017; 135: 2241 -2251
Global Adoption of Coronary Physiology to Guide Revascularization Decision Making in 2016 Gōtberg M, et al. J Am Coll Cardiol 2017; 70: 1379 -1402
Coronary flow velocity recordings Aortic stenosis* HCM** * Yoshikawa J, Akasaka T, et al. J Am Soc Echocardiogr 1993; 6: 516 -524 ** Akasaka T, Yoshikawa J, et al. J Am Soc Echocardiogr 1994; 7: 9 -19
Individual FFR in AS patients before and after TAVI Pesarini G, et al. Circ Cardiovasc Interv. 2016; 9: e 004088
FFR variations in patients with AS before and after TAVI %DS <50 FFR <0. 8 pre- & post TAVI %DS ≥ 50 FFR <0. 8 pre- & post PCI Pesarini G. , et al. Circ Cardiovasc Interv. 2016; 9: e 004088
Coronary flow-pressure relationship Pressure ≈ flow Coronary pressure-derived indices, such as i. FR and FFR, are based on the fundamental principle that the trans-lesional pressure ratio approximates coronary flow when micro-vascular resistance is minimized in diastole.
Wave free period & i. FR Nijjer SS, et al. Circ J 2015; 79: 1172– 1184.
Coronary Autoregulation as a Means of Quantifying Stenosis Severity Under Resting Conditions GŌtberg M, et al. J Am Coll Cardiol 2017; 70: 1379 -1402
DEFINE-FLAIR Cumulative Risk of the Primary Endpoint Davies JE, et al. N Engl J Med 2017; 376: 1824 -34. SWEDEHEART Kaplan-Meier Curve for the Primary Endpoint Gōtberg M, et al. N Engl J Med 2017; 376: 1813 -23.
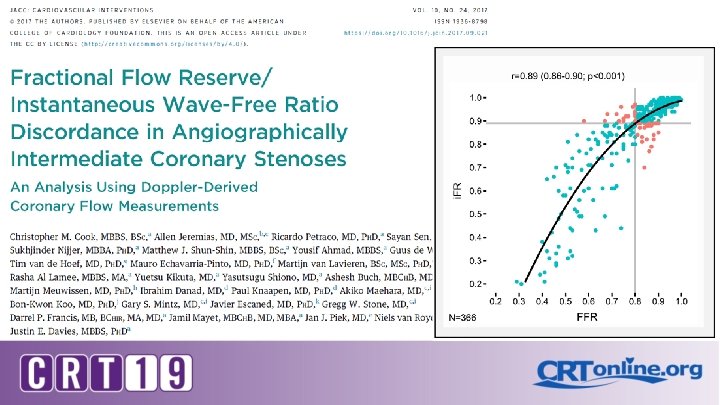
Comparison among different diastolic indexes & i. FR van’t Veer M, et al. J Am Coll Cardio 2017; 70: 3088 -3096.
Diagnostic Values of Diastolic Indexes At Cutoff Value of ≦ 0. 89 vs FFR 0. 8 Correlations & AUC Values >0. 99 for All Resting Pd/Pa Ratios Over Different Periods in Diastole compared with i. FR van’t Veer M, et al. J Am Coll Cardio 2017; 70: 3088 -3096
PCI case with i. FR co-registration
Prediction of post PCI i. FR by Syncvision i. FR predicted Short STENT ? 0. 86 i. FR predicted Long STENT ? (with two stents) 0. 93
Prediction of post PCI i. FR by Syncvision 2. 5 × 23 DES We chose a short stent and the final angio & i. FR was demonstrated the ideal result as we predicted before PCI.
Advantage of i. FR Pullback Nijjer S, et al. JACCint 2014; 12: 1386 -1396. Rest Flow HE Flow GŌtberg M, et al. J Am Coll Cardiol 2017; 70: 1379 -1402
Representative Examples of FFRCT (NXT trial) Correlation between FFRCT & FFR Nørgaard BL, et al. J Am Coll Cardiovasc Imag 2016 doi. org/10. 1016/j. jcmg. 2015. 11. 025 Norgaard BL, et al. J Am Coll Cardiol 2014; 63: 1145 - 1155
High Accuracy of FFRCT Compared to Gold Standard DISCOVER-FLOW Koo et al, JACC 2011. N=103 patients De. FACTO Min et al, JAMA 2012. N=252 patients NXT Norgaard et al, JACC 2014 N=254 patients NXT Per-Vessel Performance • Specificity: 86% • Sensitivity: 84% • Accuracy: 86% NXT data supported 2014 FDA Clearance
Computation of FFR From 3 D QCA and TIMI Frame Count (A, B) X-ray angiography Tu S, et al. JACC: Cardiovasc Interv, 2014; 7: 768– 777 ,
Correlation & Agreement between FFR and f. QFR or c. QFR Between FFR and f. QFR Between FFR and c. QFR Emori H, et al. Circ J, 2018 doi: 10. 1253/circj. CJ-17 -0949
ROC curves for assessing the accuracy of QFR for predicting functionally significant stenosis (FFR≦ 0. 80) 77% 87% Emori H, et al. Circ J, 2018 doi: 10. 1253/circj. CJ-17 -0949 87% 92%
Take home message Although FFR might have a limitation based on diastolic coronary pressure-flow relationship, there are many evidence demonstrating clinical usefulness. Furthermore, several non-invasive FFR measurement systems such as FFRCT, QFR and so on are developing according to the evidence of invasive FFR, and clinical evidence have been demonstrated by these methods. Although timing of measurement is thought to be ideal in i. FR based on diastolic coronary pressure-flow relationship, there are still limitted data demonstrating clinical usefulness. There are several resting indexes similar to i. FR, and clinical usefulness of them should be demonstrated in the near future. Although non-inferiority of i. FR for PCI guidance compared with FFR has been reported in DEFINE-FLAIR study and i. FR SWEDEHEART Trials and class I recommendation has been obtained in i. FR and FFR in ESC guideline 2018, there are still unresolved issues which should be investigated adequately and further investigation would be required in this field.
Thank you for your kind attention !! Welcome to APSC 2020 in Kyoto, Japan!!
SYNTAX II Serruys P et al. EUROPCR 2013
Lesion treatment ater i. FR/FFR interrogation (n=1177) PCI deferred 31% PCI performed 69% Lesions treated per pa&ent (n) in SYNTAX II and SYNTAX I 5 P < 0. 001 4. 02 4 3 Cases of three-vessel PCI (%) in SYNTAX II and SYNTAX I 100 80 83. 3 60 2. 64 2 40 1 20 0 SYNTAX II P < 0. 001 SYNTAX I 0 37. 2 SYNTAX II SYNTAX I
Primary endpoint: MACCE
Exploratory End-Point: MACCE PCI vs. CABG 11. 2% 10. 6% *Non-inferiority margin of 5% with a one-sided alpha of 5%
Comparison between FFR & i. FR at present FFR Pressure Wire Hyperemia free Typical measurement time Pressure damping unlikely Cost saving(add to FAME) Optimized for pullback Peri-PCI assessment Evidence against ischemia Clinical outcome data i. FR ✗ 5 -10 min 1 -2 min ✗ ✗ Adenosine / Time Equipment ✗ ✗ Just Coming !
Comparison among FFRs & i. FR Imaging modality On-Line Pressurewire use Analysis time Hyperemia FFR p-wire Angio Yes <5 mim Yes FFR CTA-HF CTA No No 24 hrs No FFR CTA-SM CTA No No >35 min No QFR 3 D-Angio Yes No <4 min No i. FR Angio Yes <5 min No/yes