Solitary Pulmonary Nodule Samson Munn M D Solitary







, or have")


")
 Exogenous lipid pneumonia")



 and “densely diffusely” calcification patterns are typical of granuloma")

 in half or more of cases.")



 for lung Ca is rarely")























- Slides: 54
Solitary Pulmonary Nodule Samson Munn, M. D.
Solitary Pulmonary Nodule • • • “Coin lesion” Defined as < 3 cm Completely surrounded by lung parenchyma
Solitary Pulmonary Nodule • • • Incidence of cancer reportedly 10 – 70% Found on 0. 09 to 0. 20 % of all CXRs (approximately 1 in 500) 90% are incidental findings > 150, 000 SPNs found annually Most are incidental findings on CT
Solitary Pulmonary Nodule • • SPN cancers are usually the best stage, IA (T 1 N 0 M 0) SPN cancers usually have the best 5 -year survival after surgery; can be as high as 8090% Half of all lung cancers have extrapulmonary spread by time of diagnosis Overall lung Ca 5 -year survival = 10 – 15%
Solitary Pulmonary Nodule • • • Most SPNs are histologically benign Of those not benignly calcified, primary malignancy found in about ~ 1/3 Of those not benignly calcified, solitary metastases may account for ~ 1/4
Differential Diagnosis • • • Neoplasm Infection/inflammation Vascular lesion Lung cyst, filled Pulmonary infarct Amyloid nodule • • Rheumatoid nodule Intrapulmonary LN Plasma cell granuloma Sarcoidosis Mucoid impaction Hematoma Nipple
CXR • • • Non detection of lung cancer by CXR is one of most frequent non diagnoses in radiology Reported non detection rates of 25– 90% 20– 50% non detection rate is generally accepted
CXR Retrospection Nodules not detected are generally smaller (median diameter 16 mm), or have more superimposed structures (such as ribs, blood vessels or both) and less welldefined margins.
CXR • • Delay in diagnosis is typically about a year or a year and a half. Results in 43% of lesions being upstaged from T 1 to T 2 during the delay period.
Bad Margin • • Corona radiata sign Fine linear strands extending 4– 5 mm outward Spiculated on CXRs 85– 90% malignant
Same Bad Margin (cancer)
Same Bad Margin (not cancer) Exogenous lipid pneumonia
Less Bad Margins • • Scalloped border has an intermediate probability of cancer Smooth border suggestive of more likely benign diagnosis
Other Characteristics • • Air bronchograms more commonly malignant, particularly adeno. Ca or bronchioloalveolar Ca (adeno. Ca in situ) Cavitation with a thick wall more often malignant than thin
Calcification • • Suggests diagnosis is more likely benign CXR: poor ability to discern Ca++ in a nodule • • sensitivity only 50% specificity 87% PPV 93% for identifying calcification CXR is not standard of care in demonstrating a benign pattern of Ca++
Benign Calcification Multilaminar (concentric circles) and “densely diffusely” calcification patterns are typical of granuloma
Popcorn Calcification Classic “popcorn” pattern is often seen in hamartomas.
Hamartoma CT shows fat and calcification (often cartilage) in half or more of cases.
Non Benign Calcification Faint, stippled or eccentric patterns can occur in cancers
Eccentric Calcification
Rounded Atelectasis characteristic whorl pattern
Growth Rate • • • Volume doubling time (VDT) for lung Ca is rarely < 1 month or > 1 year. 170 -200 days would be typical. Longer for adeno. Ca, including bronchioloalveolar Ca (adeno. Ca in situ), shorter for SCCa. VDT shorter (faster) in younger patients; worse prognosis. If spherical, a 30% increase in diameter represents a doubling of volume.
Growth • • Traditionally: stability of SPN on CXR for ≥ 2. 0 years diagnostic of benign disease. Recently: need 3. 0 years if ground-glass or partially ground-glass. Bronchioloalveolar cell Ca (adeno. Ca in situ) or adeno. Ca does rarely appear stable for more than 2 years; those will be at least partially ground-glass. Hamartomas do sometimes grow.
Growth Rate When can one be comfortable and confident regarding a pulmonary nodule or mass with only two years’ stability? • • when there is no ground-glass component, which means CT (not CXR); and, when it is ≥ 2. 0 years, not merely 2 years.
Growth Rate When can one be comfortable and confident regarding a pulmonary nodule or mass with a ground glass component with three years’ stability? • • when it is by CT; and, ≥ 3. 0 years, not merely 3 years.
Growth Rate When can one be comfortable and confident regarding a pulmonary nodule or mass by CXR alone? Debatable. . What about 10 years? Yup. 5 years? I would again say, Yup; others might not. What about 3 years? Possibly not, medicolegally, since CXR sees ground-glass component poorly. Probably OK if the mass is very well-defined, smoothly contoured, and round. What about 4 years? Very likely, for any nodule or mass.
Growth Rate • • • The use of stability in prognostication is predicated on accurate measurement of growth. This, in turn, is reflected by the resolution of the imaging technique. Thin-section CT offers better measurement of nodule size and thus growth characteristics (and margins).
Growth Rate • • • The limit of detectable changes on CXR is estimated to be 3– 5 mm. CT has a resolution of << 1 mm. Thus, it is reasonable to use two-year stability on CT as a practical guideline for solid nodules, and 3 years for partially solid or fully ground-glass nodules.
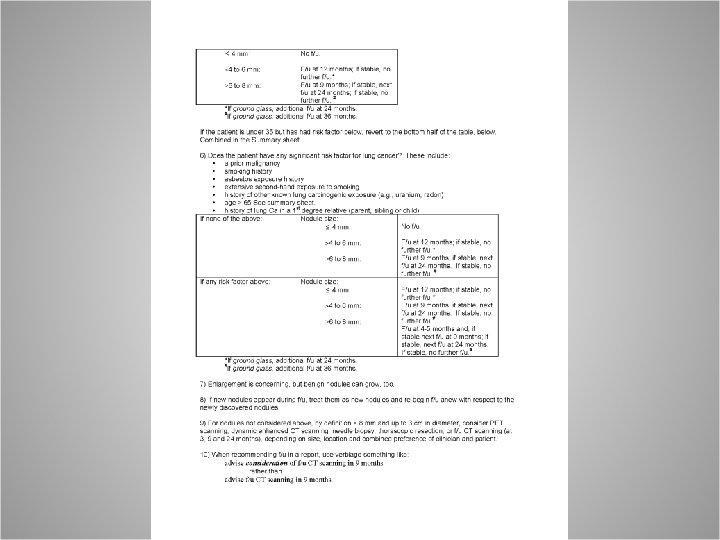
Follow-Up • • • Optimal intervals not known. Traditionally, pulmonologists and oncologists have recommended and still recommend following every three months for first year, then each six months. That is wrong-headed, since it ignores that: • • • CTs cause lung and other cancers; lung Ca grows ~ biologically; i. e. , by doubling; and, risk factors should also be considered in f/u setting.
Nonsurgical Approaches to the Nodule Itself • • Contrast-enhanced CT Bronchoscopy Transthoracic fine needle aspiration biopsy Positron emission tomography
Contrast-Enhanced CT • • Degree of nodule contrast-enhancement One study used an increase in attenuation of 20 Hounsfield units as threshold for malignant lesions • • • Sensitivity 95– 100% Specificity 70– 93% Needs further validation Local expertise varies Not widely used nor trusted
Bronchoscopy • • Useful for lesions of at least 2 cm diameter Diagnostic yield 20– 80%, depending on size of nodule, patient population and proximity to the bronchial tree
Bronchoscopy • Yield: • • ~ 10% for < 1. 5 cm ~ 40% for 2– 3 cm ~ 60% for > 3 cm ~ 70% yield when CT reveals a bronchus leading right up to or into the lesion
Bronchoscopy • • • Relatively low risk according to pulmonologists Overall complication rate 5% 3% risk of pneumothorax 1% risk of significant hemorrhage Yet: 0. 24% – one out of 400 – risk of death !
Transthoracic FNA Biopsy • • • Diagnostic yield up to 95% in peripheral lesions Higher complication rate However, usually, complications less severe 20– 30% pneumothorax rate Yet, only 5– 10% chest tube rate
Positron Emission Tomography • • Tumors have greater uptake of FD Lung Ca • • • sensitivity = 92– 99% specificity = 75– 90% False negatives: • • • bronchioloalveolar cell carcinoma (adeno. Ca in situ) carcinoid tumors < 1 cm in diameter
Positron Emission Tomography • • Infection also has greater uptake of FD Benign nodules • • • sensitivity = 96% specificity = 88% False positives due to inflammation or infection.
Positron Emission Tomography • • Resolution is currently only ~ 5– 10 mm Imaging of nodules < 1 cm is unreliable Yet, often provides staging information Up to 14% of patients otherwise eligible for surgery have occult extra-thoracic disease on whole-body PET, nixing a surgical approach to therapy.
PET Small LN by CT would not be classified as lymphadenopathy. Yet, the LN is clearly + by PET in axial and coronal images.
PET Images An even more dramatic example of the same thing.
Positron Emission Tomography Decision-analysis to assess cost effectiveness showed PET-CT for staging was superior to conventional approaches: • • Reduced number of surgeries – patients who otherwise would be offered false hope and arduous, painful and risky surgery – by 15% Estimated cost savings per patient ranged from $91 to $2, 200
Positron Emission Tomography • • More expensive than other imaging modalities Medicare reimbursement as of ~ 2000: • • • PET = $1, 912 chest CT = $276 transthoracic needle aspiration = $560.