Plasma cell neoplasms Plasma cell neoplasms Plasma cell









 are large usually oval with round")
 myeloma cells have higher nuclear/cytoplasmic ratio and round nucleus")






 and monoclonal immunoglobulin (“M Band”) in multiple myeloma")
- Slides: 20
Plasma cell neoplasms
Plasma cell neoplasms • Plasma cell neoplasms are a group of B cell neoplasms associated with the monoclonal proliferation (single clone) of immunoglobulinsecreting plasma cells. • These are also known as dyscrasias.
Laboratory Findings • Peripheral Blood • Hemoglobin: Decreased and usually between 6 and 10 gm/d. L. • Peripheral smear • RBCs: • WBCs: • Platelets
Laboratory Findings • Peripheral Blood • Peripheral smear • RBCs: • Usually normocytic normochromic anemia • Tendency for the red cells to adhere to one another and form columns in the blood film referred to as rouleaux formation. • This is due to increased immunoglobulins. • Rouleaux formation is characteristic but not diagnostic, as it may be seen in any condition with elevated immunoglobulins.
Laboratory Findings Peripheral Blood Peripheral smear RBCs: WBCs: Total and differential leukocyte count is normal. In terminal stages of the disease, few plasma cells may be observed in the peripheral blood. • If number of plasma cells is higher than 2 × 109/L, it is labeled as plasma cell leukemia. • Platelets: Platelet count is usually within normal limits. • • •
Laboratory Findings • ESR: Increased because of rouleaux formation due to high immunoglobulin levels. • Bleeding time: Platelets may get coated by M-component which impairs platelet aggregation resulting in increased bleeding time
Laboratory Findings • Bone Marrow • Cellularity: • Bone marrow is hypercellular, as a result of increased number of plasma cells and myeloma plasma cells (neoplastic plasma cells).
Laboratory Findings
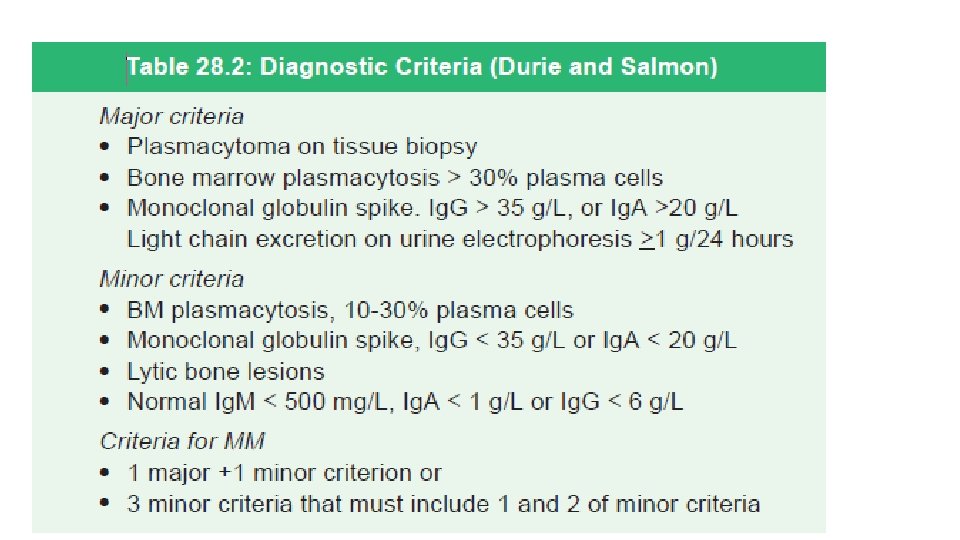
Laboratory Findings • Increased number of myeloma plasma cells more than 30% of the cellularity is diagnostic • When their number is less than 10%, demonstration of their monoclonal (κ or λ) nature is highly suggestive of myeloma. • Myeloma plasma cells are neoplastic plasma cells that vary from mature plasma cells, plasmablasts (immature) and pleomorphic plasma cells.
Laboratory Findings • Myeloma plasma cells (mature type) are large usually oval with round to oval eccentrically placed nucleus and abundant pale blue cytoplasm. • Nucleus may show “spoke wheel” or “clock-face” chromatin without nucleoli. • A perinuclear hof (clearing) due to a prominent Golgi apparatus is present. • Few of these cells may show binucleation and multinucleation.
Laboratory Findings • Plasmablastic (immature) myeloma cells have higher nuclear/cytoplasmic ratio and round nucleus with vesicular/dispersed chromatin often with prominent single nucleolus. • Presence of these cells is associated with a worse prognosis. • Pleomorphic plasma cells are multinucleated or polylobated.
Laboratory Findings Other morphological findings • Flame cells: These cells show peripheral fiery red (vermilion staining) glycogen-rich immunoglobulin A and have irregularly shaped or flame -like cytoplasm and hence the name. • Grape (morula/mott) cells: These cells have multiple bluish-white, grapelike rounded cytoplasmic droplets. • Russell bodies: These are globular, eosinophilic (cherry red), refractile inclusions in the cytoplasm. • Cells with a variety of other inclusions: These include fibrils (Gaucher -like cells, thesaurocytes), crystalline rods and globules. • Dutcher bodies: They represent intranuclear pseudo inclusions.
Laboratory Findings
Laboratory Findings • Erythropoiesis: It is diminished and is normoblastic. • Myelopoiesis: It shows normal maturation. • Megakaryopoiesis: Normal. • As the tumor progresses, it may compromise erythroid, myeloid and megakaryocytic progenitors resulting in pancytopenia
Laboratory Findings • Urine: It may show Bence Jones protein
Laboratory Findings • Serum β 2 microglobulin: It is a useful prognostic marker and high values signify poor prognosis. • Hypercalcemia: It is due to extensive osteolytic lesions and osteoporosis and there also increased levels of serum phosphate and serum alkaline phosphatase. • Blood urea, serum creatinine and uric acid: They are often raised when there is impairment of renal function. This is associated with reduced creatinine clearance. • Serum albumin: Decreases in advance stages of the disease.
Electrophoretic Studies on Serum and Urine • Electrophoretic studies reveal raised levels of immunoglobulins in the blood and/or light chains (Bence Jones proteins) in the urine. • The monoclonal immunoglobulin (“M protein”) is identified as abnormal protein “spikes” in serum or urine electrophoresis and is then further characterized by immunofixation. • The most common M protein is Ig. G type, followed by Ig. A.
Serum electrophoresis showing normal pattern: (A) and monoclonal immunoglobulin (“M Band”) in multiple myeloma (B)