PEDIATRIC HISTORY TAKING Dr Pourmirzaiee History Taking Definition














 • Location • Duration (")







 • Any others at daycare/")














- Slides: 40
PEDIATRIC HISTORY TAKING Dr. Pourmirzaiee
History Taking - Definition • History taking can be defined as a systematic inquiry into the patient’s condition. • It is the process of obtaining relevant information from the patient or patient’s caretaker (such as the mother or father) for the purpose of making a diagnosis. • The pediatric history is the foundation upon which the future physician/ patient/ parent relationship is built.
Objectives • To understand the content differences in obtaining a medical history on a pediatric patient compared to an adult. • To understand how the age of the child has an impact on obtaining an appropriate medical history. • To highlight the role of parents during taking pediatric history.
Objectives • To highlight the fact that modern technology must be used when appropriate only to enhance the clinical assessment of the patient, not to replace it. • Understand the appropriate wording of questions in taking a pediatric history, and appropriate use of questions. • Children are not just small adults!
Goals of the history • To determine why the patient/parent came to see the physician. • To determine what the patient/parent is worried about most and why. • Direct appropriate examination and investigation • Reach a correct diagnosis (or form a differential diagnosis)
Differences of a Pediatric History Compared to an Adult History II. Parent as Historian • Parent’s interpretation of signs, symptoms o Children above the age of 4 may be able to provide some of their own history o Reliability of parents’ observations varies o Adjust wording of questions - “When did you first notice Majid was limping”? instead of “When did Majid’s hip pain start”? • Observation of parent-child interactions • Parental behaviors/emotions are important
Listening to Mothers
Listening to Mothers • A good doctor is a good listener. • Mothers are excellent observers of their children and do know when they are sick. • She may not know what’s wrong but she certainly knows something is wrong. • No one can replace the mother in providing an accurate and thorough description of the child and his complaints.
Listening to Mothers • Ask her to define her terms (What do you mean by. . . ? ). • A good opening is, ‘Tell me about your baby’, and then simply let the mother talk. • Learn through history taking to be a good listener.
Listening to Mothers • Always ask the parents to relate the sequence of events leading to the present complaints. • A suitable start ‘When was he last well? ’ • Patients appreciate a doctor who gives them individual attention and devoted time. • Mothers may, of course, unintentionally deceive. • A common complaint is: ‘I can’t get him to eat anything’ and a strong overweight toddler!
Listening to Mothers • Always ask the parents to relate the sequence of events leading to the present complaints. • A suitable start ‘When was he last well? ’ • Patients appreciate a doctor who gives them individual attention and devoted time. • Mothers may, of course, unintentionally deceive. • A common complaint is: ‘I can’t get him to eat anything’ and a strong overweight toddler!
Outline of the Pediatric History
History – General, Personal • • • Date Patient's name Birth date……. . Age Gender, be careful to use the correct gender Residence The person giving the history (relationship to patient and perceived reliability)
Presenting complaint - Chief complaint • In the patient's or parent's words. • A brief statement of the primary problem (including duration). • It is important to establish the duration of each complaint.
OLD CARTS • Onset (timing , acute , gradual) • Location • Duration ( acute , chronic , days ) • • • Characteristics ( quality, sharp, aching) Aggravating factors Relieving factors Treatments ( previously tried , results) Severity( mild. Moderate , severe)
History of the Present Illness • Any significant prior laboratory or radiology studies should be noted here. • Child maltreatment or abuse should be considered if the history and physical exam are not consistent with one another or if there is a delay in seeking care.
Past Medical History • • • Hospitalizations Surgeries Drug allergies Vaccinations Recent travel Recent exposure
Past Medical History • The relative importance of these items depends on: – the age of the patient and – the reason for the visit • In general, the birth history is not significant for an acute minor trauma visit for an adolescent!
Perinatal history • Prenatal: o Length of gestation. Age of mother at delivery o Any maternal insults [alcohol, smoking] or illnesses during gestation. • Natal: o Where born: hospital, clinic, home. o Birth weight, mode of delivery, difficulties in delivery. o Resuscitation, Apgar score • Postnatal: o Cyanosis, pallor, jaundice, convulsions, malformations, feeding or respiratory difficulties. o How baby was fed in first few days. o Whether the child went home with mother
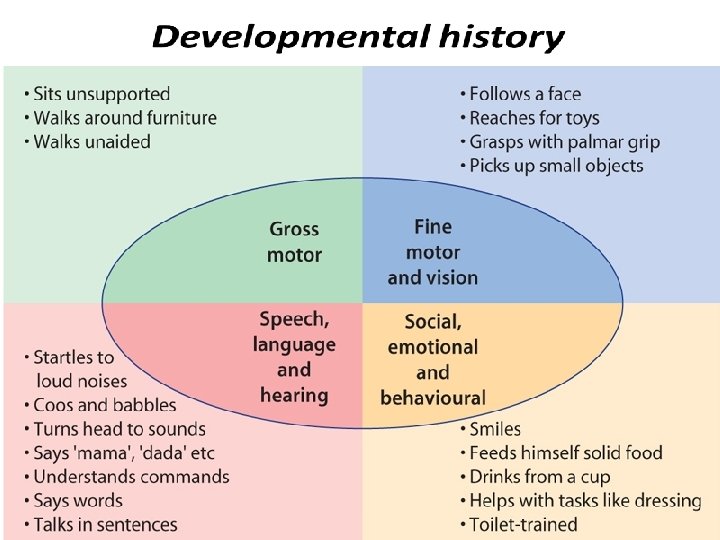
Developmental history • Age when able to… – Hold head erect when in sitting position – Roll from front to back; back to front – Sit alone; unsupported – Stand with support; without – Use words – Talk in sentences – Dress self – Age when toilet trained
Social History
Social history - Items • Living accommodation • Who lives at home with the patient, including extended family members • Age and parents' occupation • Level of parental education • Sibling relationships • The type of discipline used
Social history - Items • School performance (Education history) • Any others at daycare/ school with the same complaint. • Travel: where, how lived when there, immunization/ prophylactic status when went. • Smokers in the home. • Pets in the home. • Nationality and migration of parents.
Social History
Family history • Families share genes and diseases. • A family tree that includes the last two generations. • Childhood diseases or adult diseases with childhood onset. • History of unexplained recurrent miscarriages or SIDS.
Family history • • Neonatal deaths. Parents/siblings: age, health, where living. Height and weight of parents. Age of parents at the birth of this child.
Let The Children Speak
Let The Children Speak • Don’t forget the child!! • Children need to be heard and to be noticed. • Children over 4 years should be asked to give their account of events with parental comments. • If he does not like to talk, or shy don’t push him.
Case study
A general practitioner asks about the presenting complaints and takes a present but no other history from a mother and her 10 year-old daughter. The child has a fever and a rash. After a quick general inspection, he lifts the child’s shirt and looks at the rash. After writing a brief note in the hospital folder he tells the mother that the child has measles.
1. What mistake has the doctor made in taking a history?
1. What mistake has the doctor made in taking a history? Only a present history was taken. It is important always to take a past, social and immunization history as well.
2. Why is an immunization history important? It is important to know whether this child has been fully immunized, especially against measles and rubella.
A general practitioner asks about the presenting complaints and takes a present but no other history from a mother and her 10 year-old daughter. The child has a fever and a rash. After a quick general inspection, he lifts the child’s shirt and looks at the rash. After writing a brief note in the hospital folder he tells the mother that the child has measles.
What is a problem list? • This is a clear & simple list of the patient’s problems. • The problem list is drawn up during the assessment at the end of the complete examination. • The problem list is the most important part of summarizing the findings of the history, physical examination and investigations. • A problem list must always be made even if the diagnosis is not known.
History Taking - Summary • Personal History: Name, age, sex and address • Complaint: Main symptom(s) that necessitate medical advice • Present History: Onset, course and duration including medical care given (if any) • Past History: Perinatal, developmental, nutritional, vaccinations, …. • Social History: Home and school • Family History: siblings, similar conditions
Thank You