Omega3 Fatty Acids and Cardiovascular Disease HDL Medical






 18,")


 0. 4 Placebo 1014/3481 (29·")


 - Underpowered Alpha-Omega (2010)- Underdosed Su.")











 p=0. 03 p for trend")


")
: C 22: 6ω-3 H 3 C Eicosapentaenoic")





- Slides: 37
Omega-3 Fatty Acids and Cardiovascular Disease HDL Medical Advisory Board Mtg Sept 2011 William S. Harris, Ph. D. Research Professor, Sanford School of Medicine University of South Dakota Sr. Scientist Health Diagnostic Laboratory Richmond, VA
Outline üOmega-3 Fatty Acids üOmega-3 Intake and CHD Death üEffects of Omega-3 on CHD Events üOmega-3 Mechanisms of Action üThe HS-Omega-3 Index üRecommended Intakes
Essential Fatty Acid Families ω-3 family ω-6 family H 3 C C 18: 2 ω-6 • Corn Oil • Safflower Oil • Sunflower Oil H 3 C C 20: 4 ω-6 • Meat • Eggs H 3 C COOH Linoleic* (~6% en) C 18: 3 ω-3 • Flaxseed Oil • Canola Oil • Soybean Oil H 3 C C 20: 5 ω-3 COOH Arachidonic (0. 05% en) H 3 C C 22: 6 ω-3 • Oily Fish • Fish Oil *Conversion to AA and EPA ~ 0. 2 -0. 25% (Hussein et al. J Lipid Res 2005; 46: 269) COOH -Linolenic* (~0. 6% en) COOH Eicosapentaenoic (EPA) COOH Docosahexaenoic (DHA) (Combined ~0. 07% en)
Relations between EPA+DHA intake and risk for CHD death in US-based prospective cohort and casecontrol studies STUDIES • MRFIT • Nurse’s Health • Health Professionals • Physician’s Health • Cardiovascular Health • Seattle Primary Cardiac Arrest Harris, Kris-Etherton, Harris. Curr Athero Repts 2008; 10: 503 -509.
1800’s 1900’s 1950 1970 1980 1990 Correlation = Causation?
GISSI-Prevenzione: Time Course of Clinical Events >11, 300 post-MI patients were given usual care with or without 850 mg EPA+DHA (1 cap/d omega -3 acid ethyl esters) for 3. 5 years Control (9. 9%) 1. 0 Omega-3 (8. 4%) 0. 79 (0. 66 -0. 93), p<0. 01 Control (2. 7%) 1. 0 Omega-3 (2%) 0. 55 (0. 35 -0. 77), p<0. 001 Total mortality reduced by 21% Marchioli R et al. Circulation 2002; 105: 1897 -1903. Sudden death reduced by 45%
Japan EPA Lipid Intervention Study-JELIS (Yokoyama et al. Lancet 2007; 369: 1090 -98) 18, 645 Japanese (70% women, 61 yrs) randomized to statin alone or statin+EPA (1. 8 g/d) and followed for 5 years Entire Cohort N=18, 645 1 a Prevention=14, 981 RRR=18% P=0. 13 2 a Prevention=3, 664 RRR=19% P=0. 048 RRR=19% P=0. 011 MCE = Major coronary events were considered to be sudden cardiac death, fatal and nonfatal MI, unstable AP, and angioplasty/stenting or CABG
JELIS: Effects of EPA on MACE in High TG-Low HDL (Saito et al. Atherosclerosis 2008; 200: 135 -140) In the primary prevention cohort, EPA was most effective in patients with the metabolic syndrome
GISSI – Heart Failure Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto miocardico 6, 975 patients n-3 PUFA 1 g (3, 494) Placebo (3, 481) • Patients with HF from any etiology were included • All treatments of proven efficacy for chronic HF (e. g. , ACE-inhibitors, beta-blockers, diuretics, digitalis, spironolactone) were encouraged 3. 9 years of follow-up Primary end point: All-cause mortality GISSI HF Investigators. Lancet 2008; 372: 1223 -30.
GISSI-HF: All Cause Mortality Intention to treat analysis (n=6975) 0. 4 Placebo 1014/3481 (29· 1%) Rel Risk Reduction* = 9% (P=0. 041) Probability of death Per protocol (n=4, 995) RRR = 14% (P=0. 004) 0. 3 0. 2 n-3 PUFA 955/3494 (27· 3%) 0. 1 0. 0 0 6 12 18 24 30 36 42 48 54 Months since randomization TG=126 TG=120 TG=119 GISSI HF Investigators. Lancet 2008; 372: 1223 -30. *Cox proportional hazards model adjusted for HF hospitalization in the previous year, prior pacemaker, and aortic stenosis No change TC, LDL, HDL
Effects of Omega-3 Supplementation on Total Mortality in Post CABG Patients • 2100 patients • 44% put on omega-3 at d/c • 56% not on omega-3 • Compliant patients followed for 5 years Benedetto, et al. Ann Thorac Surg 2011; 91: 1169 – 75
Effects of Omega-3 Supplementation on Total Mortality in Post CABG Patients • 2100 patients • 44% put on omega-3 at d/c, 56% not • Compliant patients followed for 5 years Diabetes Prior PCI Prior MI LDL @ d/c < 100 TG @ d/c < 150 Omega-3 41% 22% 14% 57% 68% No omega-3 32% 15% 8% 65% 77% Factors different <0. 05 between groups; 25 other factors not different including demographics, procedural factors, drug Rx
Neutral Omega-3 Studies • • • OMEGA (2010) - Underpowered Alpha-Omega (2010)- Underdosed Su. Fol. Om 3 (2010) – Underdosed? DART-2 (2003) – poorly controlled? A-Fib (2010) – No effect ICD (n=3) – No effect
Effects of Omega-3… • Reduced platelet aggregation • Lower triglyceride levels • Reduced susceptibility to cardiac arrhythmias All mediated by…. • Altered cell membrane physiochemical properties • Shifts in eicosanoid production • Altered gene expression Courtesy Wu and Mozaffarian, unpublished
Omega-3 Ethyl Esters and Lipid Levels in Patients with Triglycerides >500 mg/d. L Baseline (mg/d. L) TG 816 HDL-C 22 Non. HDL-C 27 Chol 296 VLDL-C 175 LDL-C 89 45. 0 9. 1 6. 7 0. 0 -13. 8 -45. 0 Placebo -0. 9 -1. 7 -3. 6 P<0. 006 all -4. 8 -9. 7 -42. 0 Omega-3 Acid Ethyl Esters (4 g/day) Pooled analysis: Harris WS et al. J Cardiovasc Risk 1997; 4: 385 -391 & Pownall HJ et al. Atherosclerosis 1999; 143: 285 -297.
Lovaza Effect on Lipids in Statin-treated Patients with TG 200 -499 mg/d. L Patients stabilized on simvastatin (40 mg) x 8 weeks then randomized to placebo or Lovaza (4 g/d) for 8 weeks Avg Baseline (mg/d. L) P<0. 001 284 138 46 P=0. 052 91 P<0. 001 4. 1 COMBOS. Davidson et al. Clin Therap 2007; 29: 1354 -1367
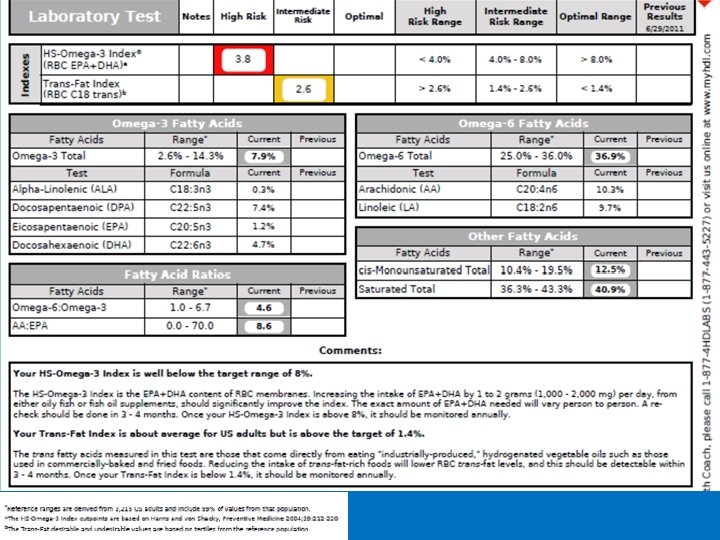
HS-Omega-3 Index® A measure of the amount of EPA+DHA in red blood cell membranes expressed as the percent of total fatty acids There are 64 fatty acids in this model membrane, 3 of which are EPA or DHA 3/64 = 4. 6% HS-Omega-3 Index = 4. 6% Harris WS and von Schacky. Prev Med 2004; 39: 212 -220. “HS” stands for “Harris Schacky”
The Omega-3 Index in National Media Men’s Health TEST DRIVE Omega. Quant HS-Omega-3 Index $150, omegaquant. com THE CLAIM Mail in a few drops of blood to find out if your body has healthy levels of omega-3 fatty acids. US News & World Report, August 2008 DOES IT WORK? Three MH editors pricked their fingers. The first, who eats fish once a week and supplements with 1, 680 mg of EPA/DHA daily, was in the desirable zone. The second supplements with 580 mg a day but rarely eats fish. He was in the intermediate zone. The third doesn’t supplement and is fish-phobic. No surprise, his score was “undesirable. ” JAMA 2010 One of 200+ scientific papers published by Harris SECOND OPINION There is now substantial data that associates desirable omega-3 levels with good health, ” says Joseph R. Hibbeln, MD, acting chief of the National Institutes of Health’s nutritional neuroscience section. “This is a valid way to monitor your health. ” April 2010, page 17
From Fish Oil to Medicine Bernadine Healy, MD. US News and World Report. August 7, 2008 “This is no fish story: Raising omega-3 s could be as important to public health as lowering cholesterol. Think about that comparison. Reining in our nation's cholesterol levels over the past 40 years has yielded great benefit to health and longevity. The change was a grass-roots effort driven by individuals—patients motivated by test results and doctors who helped monitor and manage them. The National Cholesterol Education Program even launched a "know your number" campaign. But who knows their levels of omega-3 s? ” “Before long, your personal omega-3 index just could be the new cholesterol—the number you want to brag about. ”
RBC Fatty Acid Classes Saturated Monounsaturated Polyunsaturated – Omega-6 and Omega-3 Trans Omega-6 Polyunsaturated Fatty Acids COOH Linoleic acid (LA) C 18: 2 n-6 Non-Essential Fatty Acids COOH Palmitic acid (PA) C 16: 0 Saturated Fatty Acid COOH -Linolenic acid (GLA) C 18: 3 n-6 COOH Arachidonic acid (AA) C 20: 4 n-6 Oleic acid (OA) C 18: 1 n-9 Monounsaturated Fatty Acid COOH Elaidic acid (EA) C 18: 1 n-9 trans; Trans Fatty Acid Omega-3 Polyunsaturated Fatty Acids COOH -Linolenic acid (ALA) C 18: 3 n-3 COOH Eicosapentaenoic acid, EPA C 20: 5 n-3 COOH Docosahexaenoic acid, DHA C 22: 6 n-3
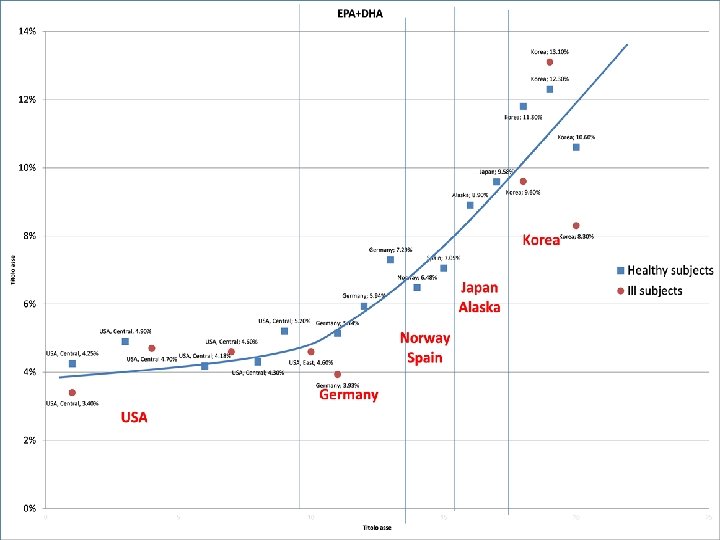
Omega-3 Index Risk Zones Japan USA/EU Undesirable Intermediate 4% Desirable 8% Percent of EPA+DHA in RBC Harris WS and von Schacky. Prev Med 2004; 39: 212 -220. Itomura, in vivo 2008; 22: 131 -136.
Why Test? HS-Omega-3 Index® • Because it is an independent risk factor for clinically-important outcomes (sudden cardiac death, total mortality, etc. ) • Because it is safely, cheaply, quickly and effectively actionable
Risk for Primary Cardiac Arrest and Red Blood Cell EPA+DHA Level Cross Sectional Prospective 6. 5 5 4. 3 3. 3 Omega-3 Index (%) Adapted from Siscovick DS et al. JAMA 1995; 274: 1363 -1367. Adapted from Albert CM et al. N Engl J Med 2002: 346: 1113 -1118.
A high omega-3 diet does not guarantee protection against sudden death
Omega-3 Index and Acute Coronary Syndromes (768 case-control pairs) p=0. 03 p for trend < 0. 0001 p<0. 001 p=0. 017 Multivariable logistic regression model including: age; race; gender; history of diabetes mellitus, hypertension, hyperlipidemia and/or myocardial infarction; a family history of coronary artery disease; and LDL-C, HDL-C, and triglycerides. Block RC, et al. Atherosclerosis 2008; 197 : 821 -828.
Blood Omega-3 Predicts Rate of Cellular Aging: Telomere Shortening
Blood Omega-3 and Rate of Telomere Attrition: Heart & Soul Study Adapted from Farzanah-Far, et al. JAMA 2010; 303: 250 -257 P<0. 001 for trend
Omega-3 Index and Time to Death in 982 CHD Patients (Heart & Soul Study) < 4. 6% ≥ 4. 6% 1. 2 yrs ≥ 4. 6% < 4. 6% Pottala et al. Circ CV O&Q; 2010
Forms of Omega-3 Fatty Acids Docosahexaenoic (DHA): C 22: 6ω-3 H 3 C Eicosapentaenoic (EPA): C 20: 5ω-3 O C H 3 C O C O C H 3 C Natural Triglyceride – Fish Oil (most supplements) H 3 C H 3 C O C Re-esterified Triglyceride H 3 C O ll C-OH Free Fatty Acid – Epanova (Omthera) choline-PO 3 O C Phospholipid – Krill Oil (Neptune/Acasti, Aker Biomarine) O C H 3 C O ll C-O-CH 2 -CH 3 Ethyl ester – Lovaza (EPA+DHA; GSK) - AMR 101 (EPA only; Amarin)
Our tests of 16 leading pill brands found that all contained roughly as much omega-3 s as their labels claimed, and none were contaminated or spoiled. So choose on price
Price Comparison: Supplements vs Lovaza Brand E+D/cap Cost/1 g E+D Kirkland 300 $0. 02 $0. 07 Natures Made 360 $0. 04 $0. 11 Kirkland 684 $0. 09 $0. 13 Natures Made 3 -6 -9 434 $0. 10 $0. 23 Metagenics 720 $0. 32 $0. 44 Wild Alaska Salmon 200 $0. 09 $0. 45 Lovaza 840 $1. 33 $1. 58 Meg-Red Krill 72 $0. 21 $2. 92 Prices as of Sept 10, 2010 at Sam’s Club, Sioux Falls, SD
AHA Scientific Statement on Fish, Fish Oils and Omega-3 Fatty Acids Population Recommendation Patients without documented CHD Eat a variety of fish (preferably oily) at least twice a week, include oils and foods rich in ALA Patients with documented Consume ~1 gm of EPA+DHA per day, preferably from fish, CHD supplements could be used in consultation with a physician Patients needing TG lowering Kris-Etherton, Harris, Appel. Circulation, 2002 2 – 4 gm of EPA+DHA per day provided as capsule under a physician’s care
AHA Scientific Statement on Fish, Fish Oils and Omega-3 Fatty Acids Population Recommendation Women with high blood cholesterol or triglycerides; for primary or secondary prevention Consumption of omega-3 fatty acids in the form of fish or capsules (e. g. , EPA 1800 mg/d) Mosca et al. Circulation Mar 22, 2011.
How REAL Men Get Their Omega-3’s