Role of Omega3 Fatty Acids in Cardiovascular Disease




 • Trans")


 18,")


 0. 4 Placebo 1014/3481 (29·")


 - Underpowered Alpha-Omega (2010)- Underdosed Su.")











: C 22: 6ω-3 H 3 C Eicosapentaenoic")

")
 similar across treatment groups")









 p=0. 03 p for trend")
- Slides: 42
Role of Omega-3 Fatty Acids in Cardiovascular Disease Prevention Tara Dall, MD Advanced Lipidology Diplomate American Board Clinical Lipidology www. advlip. com
Outline üOmega-3 Fatty Acids üOmega-3 Intake and CHD Death üEffects of Omega-3 on CHD Events üOmega-3 Mechanisms of Action üThe HS-Omega-3 Index üRecommended Intakes
3 Types of Fat
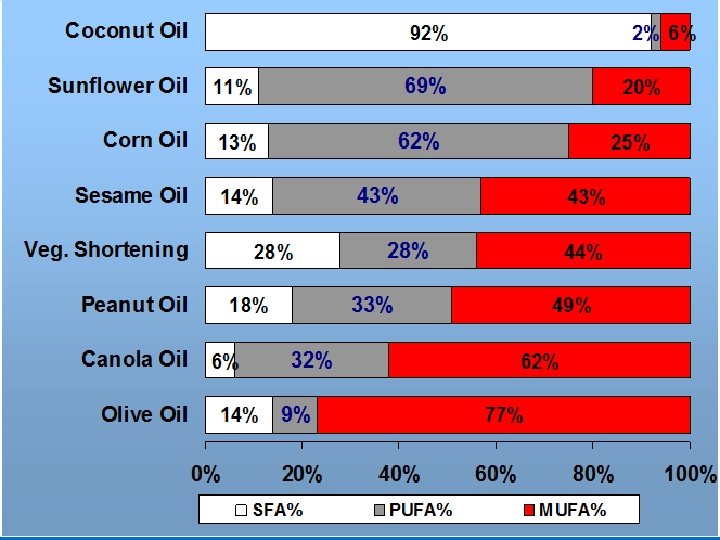
Essential Fatty Acid Families ω-3 family ω-6 family H 3 C C 18: 2 ω-6 • Corn Oil • Safflower Oil • Sunflower Oil H 3 C C 20: 4 ω-6 • Meat • Eggs H 3 C COOH Linoleic* (~6% en) C 18: 3 ω-3 • Flaxseed Oil • Canola Oil • Soybean Oil H 3 C C 20: 5 ω-3 COOH Arachidonic (0. 05% en) H 3 C C 22: 6 ω-3 • Oily Fish • Fish Oil *Conversion to AA and EPA ~ 0. 2 -0. 25% (Hussein et al. J Lipid Res 2005; 46: 269) COOH -Linolenic* (~0. 6% en) COOH Eicosapentaenoic (EPA) COOH Docosahexaenoic (DHA) (Combined ~0. 07% en)
Fat effect on cholesterol • Saturated: most LDL-C, some neutral (Stearic acid) • Trans Fatty Acids: LDL-C and HDL-C • Monounsaturated: Maintain or LDL-C and or maintain HDL-C • Polyunsaturated: Must be balanced – need more omega-3: Triglycerides, LDL-C, small dense LDL-P – most get too much omega-6
Relations between EPA+DHA intake and risk for CHD death in US-based prospective cohort and casecontrol studies STUDIES • MRFIT • Nurse’s Health • Health Professionals • Physician’s Health • Cardiovascular Health • Seattle Primary Cardiac Arrest Harris, Kris-Etherton, Harris. Curr Athero Repts 2008; 10: 503 -509.
GISSI-Prevenzione: Time Course of Clinical Events >11, 300 post-MI patients were given usual care with or without 850 mg EPA+DHA (1 cap/d omega -3 acid ethyl esters) for 3. 5 years Control (9. 9%) 1. 0 Omega-3 (8. 4%) 0. 79 (0. 66 -0. 93), p<0. 01 Control (2. 7%) 1. 0 Omega-3 (2%) 0. 55 (0. 35 -0. 77), p<0. 001 Total mortality reduced by 21% Marchioli R et al. Circulation 2002; 105: 1897 -1903. Sudden death reduced by 45%
Japan EPA Lipid Intervention Study-JELIS (Yokoyama et al. Lancet 2007; 369: 1090 -98) 18, 645 Japanese (70% women, 61 yrs) randomized to statin alone or statin+EPA (1. 8 g/d) and followed for 5 years Entire Cohort N=18, 645 1 a Prevention=14, 981 RRR=18% P=0. 13 2 a Prevention=3, 664 RRR=19% P=0. 048 RRR=19% P=0. 011 MCE = Major coronary events were considered to be sudden cardiac death, fatal and nonfatal MI, unstable AP, and angioplasty/stenting or CABG
JELIS: Effects of EPA on MACE in High TG-Low HDL (Saito et al. Atherosclerosis 2008; 200: 135 -140) In the primary prevention cohort, EPA was most effective in patients with the metabolic syndrome
GISSI – Heart Failure Gruppo Italiano per lo Studio della Sopravvivenza nell'Infarto miocardico 6, 975 patients n-3 PUFA 1 g (3, 494) Placebo (3, 481) • Patients with HF from any etiology were included • All treatments of proven efficacy for chronic HF (e. g. , ACE-inhibitors, beta-blockers, diuretics, digitalis, spironolactone) were encouraged 3. 9 years of follow-up Primary end point: All-cause mortality GISSI HF Investigators. Lancet 2008; 372: 1223 -30.
GISSI-HF: All Cause Mortality Intention to treat analysis (n=6975) 0. 4 Placebo 1014/3481 (29· 1%) Rel Risk Reduction* = 9% (P=0. 041) Probability of death Per protocol (n=4, 995) RRR = 14% (P=0. 004) 0. 3 0. 2 n-3 PUFA 955/3494 (27· 3%) 0. 1 0. 0 0 6 12 18 24 30 36 42 48 54 Months since randomization TG=126 TG=120 TG=119 GISSI HF Investigators. Lancet 2008; 372: 1223 -30. *Cox proportional hazards model adjusted for HF hospitalization in the previous year, prior pacemaker, and aortic stenosis No change TC, LDL, HDL
Effects of Omega-3 Supplementation on Total Mortality in Post CABG Patients • 2100 patients • 44% put on omega-3 at d/c • 56% not on omega-3 • Compliant patients followed for 5 years Benedetto, et al. Ann Thorac Surg 2011; 91: 1169 – 75
Effects of Omega-3 Supplementation on Total Mortality in Post CABG Patients • 2100 patients • 44% put on omega-3 at d/c, 56% not • Compliant patients followed for 5 years Diabetes Prior PCI Prior MI LDL @ d/c < 100 TG @ d/c < 150 Omega-3 41% 22% 14% 57% 68% No omega-3 32% 15% 8% 65% 77% Factors different <0. 05 between groups; 25 other factors not different including demographics, procedural factors, drug Rx
Neutral Omega-3 Studies • • • OMEGA (2010) - Underpowered Alpha-Omega (2010)- Underdosed Su. Fol. Om 3 (2010) – Underdosed? DART-2 (2003) – poorly controlled? A-Fib (2010) – No effect ICD (n=3) – No effect
Lipid and Lipoprotein Metabolism in the Normal Person Cholesteryl ester Glycerol Apo B DGAT 2 Triglyceride VLDL (Very–low-density lipoprotein) TG: Cholesterol=5: 1 ratio Fatty acids Liver
Lipid and Lipoprotein Metabolism in the Normal Person Muscle and adipose tissue Fatty acids Lipoprotein lipase Lipase Bloodstream LDL IDL LDL receptor VLDL Liver Hepatocyte
Lipid and Lipoprotein Metabolism in Hypertriglyceridemia Increased triglyceride secretion Cholesteryl ester VLDL Triglycerides TG: Cholesterol 5: 1 Liver
Lipid and Lipoprotein Metabolism in Hypertriglyceridemia Muscle and adipose tissue Lipoprotein lipase Lipase Bloodstream LDL Decreased conversion to LDL VLDL Liver
Lipid and Lipoprotein Metabolism in Hypertriglyceridemia Lipase Bloodstream CETP Increased VLDL ↑ Small, dense LDL CE T P Rapid degradation Small, dense HDL ↑ Free fatty acids ↑ Triglycerides ↑ Apo-B Lipase Liver ↓ HDL
Normalizing Lipid and Lipoprotein Metabolism Muscle and adipose tissue Lipoprotein lipase Lipase Bloodstream Proper conversion to LDL VLDL Liver LDL
Potential Triglyceride-Lowering Mechanisms of Omega-3 FA NEFA Hormone-Sensitive Lipase Adipose TG Cell membrane – FA Uptake + В-oxidation Mitochondria CPT-I, -II Acyl-Co. A dehydrogenase Glucose Uptake Acyl-Co. A synthase FA Acetyl-Co. A carboxylase FA synthase Lipogenesis – + Β-oxidation DAG Glycerol-3 -P PA PAP Lyso PA + Peroxisome – Phospholipids DGAT TG – VLDL – Apo B-100 + Acyl-Co. A oxidase (rodents only? ) Acetyl Co. A Degradation Harris WS and Bulchandani D. Curr Opin Lipidol 2006; 17: 387 -393. Slide Source: Lipids Online www. lipidsonline. org
Omega-3 Ethyl Esters and Lipid Levels in Patients with Triglycerides >500 mg/d. L Baseline (mg/d. L) TG 816 HDL-C 22 Non. HDL-C 27 Chol 296 VLDL-C 175 LDL-C 89 45. 0 9. 1 6. 7 0. 0 -13. 8 -45. 0 Placebo -0. 9 -1. 7 -3. 6 P<0. 006 all -4. 8 -9. 7 -42. 0 Omega-3 Acid Ethyl Esters (4 g/day) Pooled analysis: Harris WS et al. J Cardiovasc Risk 1997; 4: 385 -391 & Pownall HJ et al. Atherosclerosis 1999; 143: 285 -297.
Lovaza Effect on Lipids in Statin-treated Patients with TG 200 -499 mg/d. L Patients stabilized on simvastatin (40 mg) x 8 weeks then randomized to placebo or Lovaza (4 g/d) for 8 weeks Avg Baseline (mg/d. L) P<0. 001 284 138 46 P=0. 052 91 P<0. 001 4. 1 COMBOS. Davidson et al. Clin Therap 2007; 29: 1354 -1367
Over the counter vs Prescription Omega 3
Composition of Prescription Omega-3 FA • Less than 90 mg of n-6, n-7, and n-9 fatty acids • Heavy metals not detectable • Dioxins and halogenated polycarbons not detectable • No Trans fatty acids
Forms of Omega-3 Fatty Acids Docosahexaenoic (DHA): C 22: 6ω-3 H 3 C Eicosapentaenoic (EPA): C 20: 5ω-3 O C H 3 C O C O C H 3 C Natural Triglyceride – Fish Oil (most supplements) H 3 C H 3 C O C Re-esterified Triglyceride H 3 C O ll C-OH Free Fatty Acid – Epanova (Omthera) choline-PO 3 O C Phospholipid – Krill Oil (Neptune/Acasti, Aker Biomarine) O C H 3 C O ll C-O-CH 2 -CH 3 Ethyl ester – Lovaza (EPA+DHA; GSK) - AMR 101 (EPA only; Amarin)
Marine Study EPA only product • The MARINE study (Multi-Center, Pl. Acebo. Controlled, Randomized, Double-Bl. INd, 12 week study with an open-label Extension) investigated the efficacy and safety of AMR 101 in reducing TG levels in patients with very high TG (≥ 500 mg/d. L) evaluated the effect of AMR 101 on other lipid and lipoprotein parameters
The MARINE Study Median Placebo-Adjusted Change from Baseline for Efficacy End Points (ITT population) ****P<0. 0001; ***P<0. 001; **P<0. 01; *P<0. 05; NS=Not Significant (P 0. 05) P-values reflect differences between AMR 101 versus placebo Apo B=apolipoprotein B; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol; Lp. PLA 2=lipoprotein-associated phospholipase A 2; TC=total cholesterol; VLDL-C=very–low-density lipoprotein cholesterol; VLDLTG=very–low-density lipoprotein triglycerides.
The MARINE Study Safety Assessments • Treatment-emergent adverse events (TEAEs) similar across treatment groups – Most were mild to moderate and deemed not related to study drug • 2 serious adverse events (SAEs) deemed unrelated to study drug – Noncardiac chest pain (AMR 101 2 g/day) – CAD (AMR 101 4 g/day) • 4 discontinuations due to TEAEs (3 placebo; 1 AMR 101 2 g/day) • No deaths occurred during the study • No significant changes in FBG, Hb. A 1 C, vital signs, electrocardiograms, or liver or kidney function with either AMR 101 dose Hb. A 1 C=hemoglobin A 1 C
Our tests of 16 leading pill brands found that all contained roughly as much omega-3 s as their labels claimed, and none were contaminated or spoiled. So choose on price
Price Comparison: Supplements vs Lovaza Brand E+D/cap Cost/1 g E+D Kirkland 300 $0. 02 $0. 07 Natures Made 360 $0. 04 $0. 11 Kirkland 684 $0. 09 $0. 13 Natures Made 3 -6 -9 434 $0. 10 $0. 23 Metagenics 720 $0. 32 $0. 44 Wild Alaska Salmon 200 $0. 09 $0. 45 Lovaza 840 $1. 33 $1. 58 Meg-Red Krill 72 $0. 21 $2. 92 Prices as of Sept 10, 2010 at Sam’s Club, Sioux Falls, SD
AHA Scientific Statement on Fish, Fish Oils and Omega-3 Fatty Acids Population Recommendation Patients without documented CHD Eat a variety of fish (preferably oily) at least twice a week, include oils and foods rich in ALA Patients with documented Consume ~1 gm of EPA+DHA per day, preferably from fish, CHD supplements could be used in consultation with a physician Patients needing TG lowering Kris-Etherton, Harris, Appel. Circulation, 2002 2 – 4 gm of EPA+DHA per day provided as capsule under a physician’s care
AHA Scientific Statement on Fish, Fish Oils and Omega-3 Fatty Acids Population Recommendation Women with high blood cholesterol or triglycerides; for primary or secondary prevention Consumption of omega-3 fatty acids in the form of fish or capsules (e. g. , EPA 1800 mg/d) Mosca et al. Circulation Mar 22, 2011.
Ways to Get 1 g/d EPA+DHA • Fish - 2– 3 oz salmon, sardines, mackerel per day • Dietary Supplements - Low Potency: 300 mg EPA+DHA/g (Typical drug store capsules; 3 g/d) - Mid Potency: 500– 700 mg EPA+DHA/g (Mail-order, online, etc; 2 g/d) • Prescription medication - High Potency: 850 mg EPA+DHA/g (Omega-3 acid ethyl esters; 1 g/d) • Cod Liver Oil - 1 tsp (RDA for vitamin D; 2 RDA for vitamin A )
Easy habits to more Omega-3 s • Eat fish twice a week – Tuna or salmon salad made with canola mayo – Salmon on most menus, reasonable cost, easy to prepare – Anchovies on pizza, snack on herring • • Use ground flax on cereal, salad, yogurt Sauté with canola oil Bake with canola or walnut oil Salad – Avocado and walnuts, dressing made with canola or walnut oil – Dark salad greens • Add side veggies dark green leafy veggies, kale, rapini, broccoli • Canola non-hydrogenated margarine • Canola mayonnaise
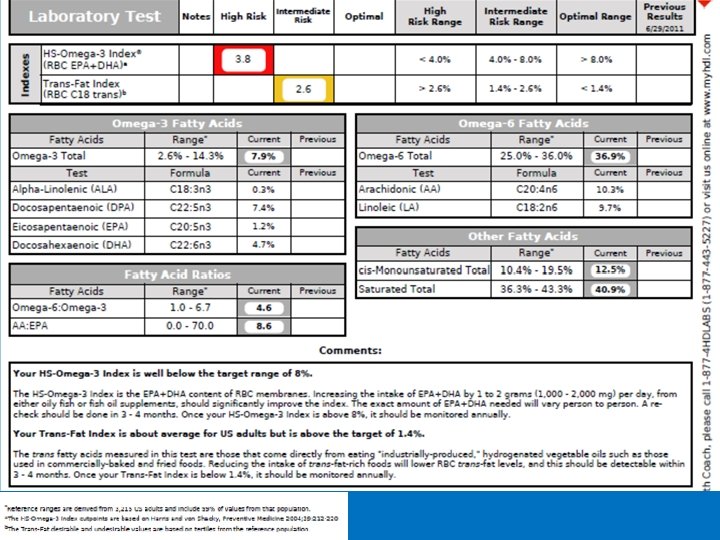
HS-Omega-3 Index® A measure of the amount of EPA+DHA in red blood cell membranes expressed as the percent of total fatty acids There are 64 fatty acids in this model membrane, 3 of which are EPA or DHA 3/64 = 4. 6% HS-Omega-3 Index = 4. 6% Harris WS and von Schacky. Prev Med 2004; 39: 212 -220. “HS” stands for “Harris Schacky”
Omega-3 Index Risk Zones Japan USA/EU Undesirable Intermediate 4% Desirable 8% Percent of EPA+DHA in RBC Harris WS and von Schacky. Prev Med 2004; 39: 212 -220. Itomura, in vivo 2008; 22: 131 -136.
Risk for Primary Cardiac Arrest and Red Blood Cell EPA+DHA Level Cross Sectional Prospective 6. 5 5 4. 3 3. 3 Omega-3 Index (%) Adapted from Siscovick DS et al. JAMA 1995; 274: 1363 -1367. Adapted from Albert CM et al. N Engl J Med 2002: 346: 1113 -1118.
Omega-3 Index and Acute Coronary Syndromes (768 case-control pairs) p=0. 03 p for trend < 0. 0001 p<0. 001 p=0. 017 Multivariable logistic regression model including: age; race; gender; history of diabetes mellitus, hypertension, hyperlipidemia and/or myocardial infarction; a family history of coronary artery disease; and LDL-C, HDL-C, and triglycerides. Block RC, et al. Atherosclerosis 2008; 197 : 821 -828.