Neuroproteo no RN prematuro Sulfato de Magnsio e

 é um grupo heterogêneo de síndromes clínicas permanentes, não progressivas, caracterizadas")








 na Obstetrícia.")









 and")
 were eligible for this review. Antenatal magnesium sulphate therapy")



























: 227 -231 Background: To compare neonatal mortality and")



- Slides: 56
Neuroproteção no RN prematuro Sulfato de Magnésio e Via de parto Silândia Amaral da Silva Freitas Brasília, 22 de novembro de 2014 www. paulomargotto. com. br
Paralisia cerebral (PC) é um grupo heterogêneo de síndromes clínicas permanentes, não progressivas, caracterizadas por disfunção motora e postural, devidas a anormalidades do desenvolvimento do cérebro. Updated: Sep 10, 2014
3 É multifatorial. Causas conhecidas - pequena proporção. Maioria - fatores pré-natais. Hipóxia / isquemia perinatal - algum papel. Prematuridade - associação comum.
4 E S P O N T N E A PREMATURIDADE I N D U Z I D A Nos Estados Unidos, 2% partos menos 32 semanas de gestação. Magnesium sulfate for the prevention of cerebral palsy American Journal of Obstetrics & Gynecology JUNE 2009
Melhor assistência neonatal tem aumentado incidência de prematuros, bem como a sobrevida deles. Paralisia cerebral – 42 a 49% associados a prematuridade.
6 Sobrevida e morbidade em prematuros com menos de 32 semanas de gestação na região central do Brasil Márcia Pimentel de Castro 1; Lígia Maria Suppo Souza Rugolo 2; Paulo Roberto Margotto 3 Estudo prospectivo de coorte, no qual todos os RN prematuros, com IG entre 25 e 31 semanas e 6 dias, sem malformações maiores, nascidos vivos na Maternidade do Hospital Regional da Asa Sul (HRAS), em Brasília, e internados na UTI neonatal desse Hospital, no período de 1º de novembro de 2009 a 31 de outubro de 2010 foram incluídos. Os RNs foram estratificados em três faixas de IG, constituindo 3 grupos: G 25, IG entre 25 e 27 semanas e 6 dias; G 28, 28 a 29 semanas e 6 dias; G 30, 30 a 31 semanas e 6 dias. Rev Bras Ginecol Obstet. 2012; 34(5): 235 -42
7
8 DANOS CEREBRAIS NA PREMATURIDADE Limitado entendimento das causas e desenvolvimento de estratégias para prevenção primária.
9 DANOS CEREBRAIS NA PREMATURIDADE Risco PC quase 80 vezes maior entre os bebês nascidos entre 23 e 27 semanas de gestação do que entre bebês nascidos a termo. Updated: Sep 30, 2014 Lesão da substância branca Hemorragia intraventricular Leucomalácia periventricular Ecodensidade Intraparenquimatosa.
10 DANOS CEREBRAIS NA PREMATURIDADE Resulta de lesão neuronal ou insulto ao cérebro em desenvolvimento. Inflamação, lesão hipóxica, excitatória ou oxidativa.
11 SULFATO DE MAGNÉSIO PARA NEUROPROTEÇÃO Sulfato de Magnésio (Mg. SO 4) na Obstetrícia. Dados observacionais (1990) menos morbidades neurológicas em prematuros expostos ao sulfato de magnésio.
12 SULFATO DE MAGNÉSIO : MECANISMOS DE AÇÃO Estabiliza pressão arterial, reduzindo a constrição nas artérias cerebrais Restaura perfusão cerebral. Estabilidade hemodinâmica • Antenatal Exposure to Magnesium Sulfate and Neuroprotection in Preterm Infants Obstet Gynecol Clin N Am 38 (2011) 351– 366
13 SULFATO DE MAGNÉSIO : MECANISMOS DE AÇÃO Lesão HI fase aguda o oxigênio é esgotado feto metabolismo anaeróbico acúmulo intracelular de sódio, cálcio, cloreto e água (edema citotóxico) neurotransmissores excitatórios. Prevenção de lesões e estabilização neuronal excitatória Antenatal Exposure to Magnesium Sulfate and Neuroprotection in Preterm Infants Obstet Gynecol Clin N Am 38 (2011) 351– 366
14 SULFATO DE MAGNÉSIO : MECANISMOS DE AÇÃO Bloquea fluxo de NA Estabiliza membrana para impedir a sua despolarização persistente resultante da falha da bomba NA-K ATP-dependente. Restauração do permeabilidade da barreira hemato-encefálica depois de uma injúria HI. Antenatal Exposure to Magnesium Sulfate and Neuroprotection in Preterm Infants Obstet Gynecol Clin N Am 38 (2011) 351– 366
15 SULFATO DE MAGNÉSIO : MECANISMOS DE AÇÃO Radicais livres de oxigênio atacam a membrana celular, causando a fragmentação celular e morte. Propriedades antioxidantes • Antenatal Exposure to Magnesium Sulfate and Neuroprotection in Preterm Infants Obstet Gynecol Clin N Am 38 (2011) 351– 366
16 SULFATO DE MAGNÉSIO : MECANISMOS DE AÇÃO Mediadores inflamatórios, interleucina-1 b e fator de necrose tumoral, aumentados 1 a 4 h após a lesão HI citotoxicidade de lesão HI. Mg. SO 4 diminui essas citocinas pró-inflamatórias. Propriedades anti-inflamatórias Antenatal Exposure to Magnesium Sulfate and Neuroprotection in Preterm Infants Obstet Gynecol Clin N Am 38 (2011) 351– 366
17 JUNHO / 2009
18
19 TABELA I: Effect of magnesium sulfate on cerebral palsy Antenatal magnesium sulfate for the prevention of cerebral palsy in preterm infants less than 34 weeks’ gestation: a systematic review and misanalysis JUNE 2009 American Journal of Obstetrics & Gynecology
20 TABELA II: Effect of magnesium sulfate on cerebral palsy and pediatric mortality Nº of events/total number Outcome Nº of trials Magnesium No magnesium Relative risk (95% CI) I² (%) Cerebral palsy 6 104/2658 152/2699 0. 69 (0. 55 -0. 88) 4. 4 Moderate/severe cerebral palsy 3 45/2169 72/2218 0. 64 (0. 44 -0. 92) 0. 0 Mild cerebral palsy 3 54/2169 74/2218 0. 74 (0. 52 -1. 04) 0. 0 Total pediatric mortality 6 401/2658 400/2699 1. 01 (0. 89 -1. 14) 38. 9 Fetal mortality 5 17/2254 22/2298 0. 78 (0. 42 -1. 46) 0. 0 Under 2 y of corrected age mortality 5 217/2254 220/2298 1. 00 (0. 84 -1. 19) 47. 3 Death or cerebral palsy 6 505/2658 551/2699 0. 92 (0. 83 -1. 02) 43. 3 Antenatal magnesium sulfate for the prevention of cerebral palsy in preterm infants less than 34 weeks’ gestation: a systematic review and misanalysis JUNE 2009 American Journal of Obstetrics & Gynecology
21 SULFATO DE MAGNÉSIO PARA NEUROPROTEÇÃO. American College of Obstetricians and Gynecologists (ACOG) and Society for Maternal-Fetal Medicine - março 2010. “A evidência disponível sugere que o sulfato de magnésio administrado antes do nascimento prematuro reduz o risco de paralisia cerebral”.
22 Five trials (6145 babies) were eligible for this review. Antenatal magnesium sulphate therapy given to women at risk of preterm birth substantially reduced the risk of cerebral palsy in their child (relative risk (RR) 0. 68; 95% Confidence interval (CI) 0. 54 to 0. 87; five trials; 6145 infants). There was also a significant reduction in the rate of substantial gross motor dysfunction (RR 0. 61; 95% CI 0. 44 to 0. 85; four trials; 5980 infants). No statistically significant effect of antenatal magnesium sulphate therapy was detected on paediatric mortality (RR 1. 04; 95% CI 0. 92 to 1. 17; five trials; 6145 infants), or on other neurological impairments or disabilities in the first few years of life. Overall there were no significant effects of antenatal magnesium therapy on combined rates of mortality with cerebral palsy, although there were significant reductions for the neuroprotective groups RR 0. 85; 95% CI 0. 74 to 0. 98; four trials; 4446 infants, but not for the other intent subgroups. There were higher rates of minor maternal side effects in the magnesium groups, but no significant effects on major maternal complications.
23 Authors' conclusions The neuroprotective role for antenatal magnesium sulphate therapy given to women at risk of preterm birth for the preterm fetus is now established. The number of women needed to be treated to benefit one baby by avoiding cerebral palsy is 63 (95% confidence interval 43 to 155).
24 SULFATO DE MAGNÉSIO PARA NEUROPROTEÇÃO. • Quando está indicado? • Como prescrever? Magnesium for fetal neuroprotection - American Journal of Obstetrics & Gynecology MARCH 2011
25 Algorithm for selection of candidates and administration of magnesium sulfate for fetal neuroprotection American Journal of Obstetrics & Gynecology JUNE 2009
26
27
28
29
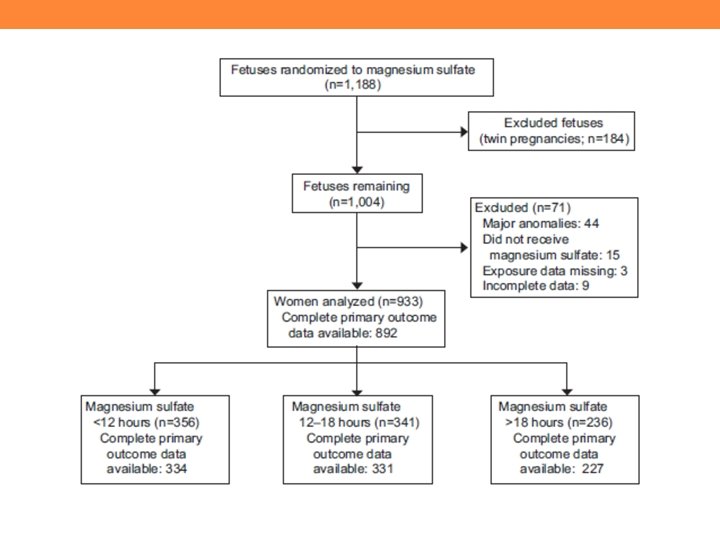
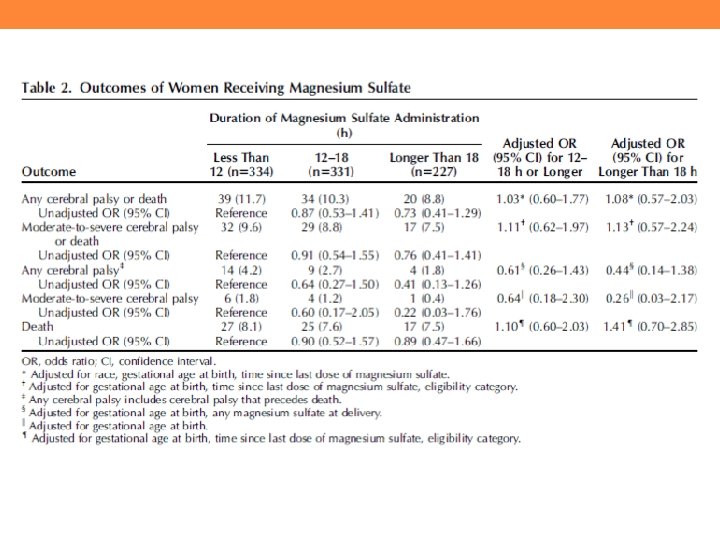
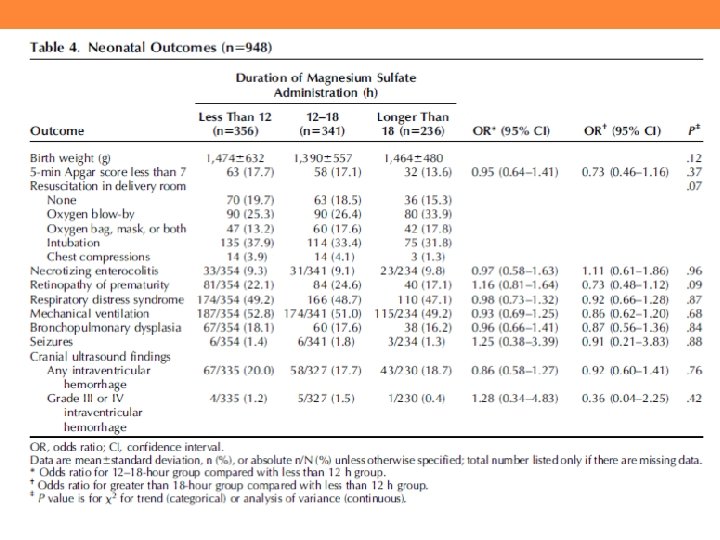
Association of duration of neuroprotective magnesium sulfate infusion with neonatal and maternal outcomes. Mc. Pherson JA 1, Rouse DJ, Grobman WA, Palatnik A, Stamilio DM. Obstet Gynecol. 2014 Oct OBJETIVO: Avaliar a associação da duração da infusão de sulfato de magnésio com natimorto ou morte, paralisia cerebral, e resultados adversos maternos e neonatais.
34 Association of duration of neuroprotective magnesium sulfate infusion with neonatal and maternal outcomes. Mc. Pherson JA 1, Rouse DJ, Grobman WA, Palatnik A, Stamilio DM. Obstet Gynecol. 2014 Oct CONCLUSÃO: A duração da infusão de sulfato de magnésio pré-natal não está associada a risco de morte ou paralisia cerebral. A duração ótima do tratamento necessária para a neuroproteção máxima permanece desconhecida.
Nenhum estudo randomizado IG <24 semanas. Cada serviço deve avaliar a viabilidade. Se a família optar por intervenções neonatais nesta idade gestacional, deve-se administrar sulfato de magnésio. updated: Sep 30, 2014
36
37 METHODS We conducted a cohort study of singleton and twin gestation extremely low birth weight infants (1000 g birth weight) born at Duke University Medical Center (Durham, NC, USA) and admitted to the Duke Neonatal Intensive Care Unit. The following three groups were defined: those born before magnesium sulfate for neuroprotection protocol (Mg. Pro) (1 January 2009 to 14 July 2010); during Mg. Pro (15 July 2010 to 30 November 2010); and after Mg. Pro (1 January 2011 to 30 October 2011). DISCUSSÃO Análise de dados demonstrou uma maior taxa de SIP e morte com Mg. Pro em relação antes / depois do protocolo, com uma sugestão que o magnésio pré-natal exerce um efeito quantitativo fortemente influenciado pela idade gestacional, ao invés de um efeito geral sobre as crianças de todos os pesos e idades gestacionais de nascimento. FETOS < 25 SEMANAS – REAVALIAR DOSE? - CONTROLAR NÍVEIS SÉRICOS DE Mg?
38 Objectives To assess the effectiveness of magnesium sulphate given to women at term as a neuroprotective agent for the fetus. Authors’ conclusions There is currently insufficient evidence to assess the efficacy and safety of magnesium sulphate when administered to women for neuroprotection of the term fetus. As there has been recent evidence for the use of magnesium sulphate for neuroprotection of the preterm fetus, high-quality randomised controlled trials are needed to determine the safety profile and neurological outcomes for the term fetus. Strategies to reduce maternal side effects during treatment also require evaluation. The Cochrane Library 2013
39 SULFATO DE MAGNÉSIO PARA NEUROPROTEÇÃO. IG 34 0/7 a 36 6/7 – sem evidência de benefício. Antenatal magnesium sulfate for the prevention of cerebral palsy in preterm infants less than 34 weeks’ gestation: a systematic review and misanalysis JUNE 2009 American Journal of Obstetrics & Gynecology
40
41
42 Mulheres com alto risco de parto dentro de 24 horas, espontâneo ou indicado, entre 24 e 32 semanas de gestação, são candidatas ao sulfato de magnésio para neuroproteção. updated: Sep 30, 2014
43 Efeitos colaterais - sudorese, rubor, náuseas, dor de cabeça. Toxicidade grave é rara, mas pode levar a parada cardíaca, depressão ou parada respiratória. Magnésio atravessa livremente a placenta. A concentração no sangue do cordão aproxima da do soro materno. Efeitos tóxicos ou neuroprotetores fetais dependem da dose. Updated: Sep 30, 2014
Antenatal magnesium sulfate exposure and acute cardiorespiratory events in preterm infants - July 18, 2014 Objetivo Magnésio pré-natal (ante. Mg) é usado para várias indicações obstétricas, incluindo a neuroproteção fetal. Crianças expostas a ante. Mg pode estar em risco de depressão respiratória na sala de parto (DR). O objetivo do estudo foi comparar o risco de eventos cardiorrespiratórios agudos entre os prematuros que foram ou não expostos a ante. Mg.
Resultados Foram avaliadas 1. 544 crianças <29 semanas de idade semanas gestacional (1. 091 no grupo ante. Mg e 453 no grupo não expostos). Mães do grupo ante. Mg eram mais propensos a ter ensino superior, hipertensão induzida pela gravidez, e corticosteróides pré-natais, enquanto seus filhos eram mais jovens na gestação e pesava menos (P <0, 05). O desfecho primário (odds ratio [OR], 1, 2; 95% intervalo de confiança [IC], 0, 88 -1, 65) foi semelhante entre os grupos. O tratamento da hipotensão (OR, 0, 70; 95% CI, , 51 -0, 97) e ventilação mecânica invasiva (OR, 0, 54; IC 95%, 0, 41 -0, 72) foram significativamente menores no grupo ante. Mg. conclusão Entre prematuros <29 semanas de gestação , a exposição ante. Mg não foi associada com um aumento de eventos cardiorrespiratórios no período neonatal precoce. A segurança de ante. Mg medida pela necessidade de intubação ou suporte respiratório no dia 1 de vida era comparável entre os grupos.
46 School-age outcomes of very preterm infants after antenatal treatment with magnesium sulfate vs placebo. JAMA. 2014 Sep 17; 312(11): 1105 -13. doi: 10. 1001/jama. 2014. 11189. Importance Antenatal magnesium sulfate given to pregnant women at imminent risk of very preterm delivery reduces the risk of cerebral palsy in early childhood, although its effects into school age have not been reported from randomized trials. Objective - To determine the association between exposure to antenatal magnesium sulfate and neurological, cognitive, academic, and behavioral outcomes at school age. Design, Setting, and Participants The ACTOMg. SO 4 was a randomized clinical trial conducted in 16 centers in Australia and New Zealand, comparing magnesium sulfate with placebo given to pregnant women (n = 535 magnesium; n = 527 placebo) for whom imminent birth was planned or expected before 30 weeks’ gestation. Children who survived from the 14 centers who participated in the school-age follow-up (n = 443 magnesium; n = 424 placebo) were invited for an assessment at 6 to 11 years of age between 2005 and 2011.
47 Main Outcomes and Measures Mortality, cerebral palsy, motor function, IQ, basic academic skills, attention and executive function, behavior, growth, and functional outcomes. Main analyses were imputed for missing data. Results Of the 1255 fetuses known to be alive at randomization, the mortality rate to school age was 14% (88/629) in the magnesium sulfate group and 18% (110/626) in the placebo group (risk ratio [RR], 0. 80; 95% CI, 0. 62 -1. 03, P = . 08). Of 867 survivors available for follow-up, outcomes at school age (corrected age 611 years) were determined for 669 (77%). Comparing the magnesium sulfate and placebo groups revealed no statistically significant difference in proportions with cerebral palsy (23/295 [8%] and 21/314 [7%], respectively; odds ratio [OR], 1. 26; 95% CI, 0. 84 -1. 91; P = . 27) or abnormal motor function (80/297 [27%] and 80/300 [27%], respectively; OR, 1. 16; 95% CI, 0. 88 -1. 52; P = . 28). There was also little difference between groups on any of the cognitive, behavioral, growth, or functional outcomes. Conclusions and Relevance - Magnesium sulfate given to pregnant women at imminent risk of birth before 30 weeks’ gestation was not associated with neurological, cognitive, behavioral, growth, or functional outcomes in their children at school age, although a mortality advantage cannot be excluded. The lack of long-term benefit requires confirmation in additional studies.
SOGC CLINICAL PRACTICE GUIDELINE ´ Magnesium Sulphate for Fetal Neuroprotection - No. 258, May 2011 1. Para as mulheres com parto prematuro iminente (≤ 31 semanas e 6 dias), a administração de sulfato de magnésio deve ser considerada para neuroproteção fetal. (I-A) 2. Embora haja controvérsia sobre a idade gestacional superior, sulfato de magnésio para neuroproteção fetal deve ser considerado a partir de viabilidade até ≤ 31 + 6 semanas. (II-1 B) 3. Se o sulfato de magnésio pré-natal foi iniciado para neuroproteção fetal, tocólise deve ser interrompida. (III-A) 4. O sulfato de magnésio deve ser interrompido se o parto não é mais iminente ou se administrado por 24 horas. (II-2 B)
5. Para as mulheres com parto prematuro iminente, sulfato de magnésio deve ser administrado como uma dose de ataque de 4 g IV, ao longo de 30 minutos, seguido por um 1 g / h de manutenção até o nascimento. (II-2 B) 6. Para parto prematuro planejado por indicações maternas e fetais, sulfato de magnésio deve ser iniciado de preferência dentro de 4 horas antes do nascimento. (II-2 B) 7. Não há evidências suficientes de que um curso de repetição do sulfato de magnésio deve ser administrado. (III-G) 8. Parto não deve ser adiado a fim de administrar sulfato de magnésio para a neuroproteção fetal , se houver indicação materna e / ou fetal para parto de emergência. (III-E)
9. Quando o sulfato de magnésio é dado para a neuroproteção fetal, prestadores de cuidados devem usar protocolos existentes para monitorização. (III-A) 10. Indicações para monitorização fetal devem seguir as recomendações de vigilância fetal. (III-A) 11. Uma vez que o sulfato de magnésio tem o potencial de alterar a avaliação neurológica do recém-nascido, causando hipotonia ou apnéia, prestadores de cuidados de saúde que cuidam de recém nascido devem ter uma maior consciência deste efeito. (III-C)
51 QUAL A MELHOR VIA DE PARTO ? ? ? Na ausência de indicação de cesariana, fetos com baixo peso devem ser submetidos à prova de trabalho de parto. A via de parto não é um fator independente importante na mortalidade perinatal ou neurodesenvolvimento. Cesariana eletiva - riscos para a mãe. Benefícios para o recém-nascido de BPN em apresentação cefálica são incertas. Updated: Oct 27, 2014.
52 Compressão da cabeça do feto BPN pelos tecidos moles maternas não é um dos principais determinantes do IVH. Por esta razão, sugerimos evitar episiotomia ou fórceps de forma eletiva. Vácuo é contra-indicado antes de 34 semanas de gestação. Analgesia - necessidades maternas. Na cesárea, a incisão na pele não devem ser menor que o habitual. Updated: Oct 27, 2014.
53 World J Pediatr 2014; 10(3): 227 -231 Background: To compare neonatal mortality and neurodevelopmental outcomes at two years of age in very low birth weight infants (≤ 1500 g) born by cesarean with those by vaginal delivery.
54 Methods: In this retrospective, case-control study, we evaluated neonatal mortality, medical conditions and neurodevelopmental outcomes at two years of corrected age in 710 very low birth weight (VLBW) infants born between January 2005 and December 2010. Of the 710 infants, 351 were born by the cesarean and 359/710 by vaginal route. Results: There were no significant differences in neonatal mortality between the cesarean delivery group and vaginal delivery group [56/351 (15. 9%) vs. 71/359 (19. 8%), P=0. 20]. VLBW infants delivered by the cesarean procedure had a higher incidence of respiratory distress syndrome than those born by the vaginal route [221/351 (63. 0%) vs. 178/359 (49. 6%), P<0. 001]. There were no differences in other neonatal morbidities, including intraventricular hemorrhage [126/351 (35. 9%) vs. 134/359 (37. 3%), P=0. 69], bronchopulmonary dysplasia [39/351 (11%) vs. 31/359 (8. 6%), P=0. 38] and necrotising enterocolitis [40/351 (11. 4%) vs. 32/359 (8. 9%), P=0. 32] between the two groups. The incidence of poor neurodevelopment after cesarean delivery was similar to that after vaginal delivery [105/351 (29. 9) vs. 104/359 (29. 0%), P=0. 78].
55 Conclusions: In neither neurodevelopment nor neonatal mortality did cesarean birth offered significant advantages to VLBW infants. Moreover, the operation might be associated with an increased risk of respiratory distress syndrome for VLBW infants. The mode of delivery of VLBW infants should be largely based on obstetric indications and maternal considerations rather than perceived better outcomes for the neonate.
56